
Oxford University released a new study on vaccine effectiveness this week based on the ONS Infection Survey. Its headline finding was that, for the period dominated by the Delta variant, the AstraZeneca jab declined from 97% vaccine effectiveness against symptomatic infection to 71% and Pfizer’s declined from 97% to 84%. The researchers note that vaccine effectiveness (VE) appears to wane with time, putting this at 7% per month in the case of AstraZeneca and 22% per month in the case of Pfizer.
One odd thing about these results is that the 97% initial VE for AstraZeneca is very high compared to other estimates, including the vaccine trial which found it to be just 70.4%.
Here are their vaccine effectiveness results in full.
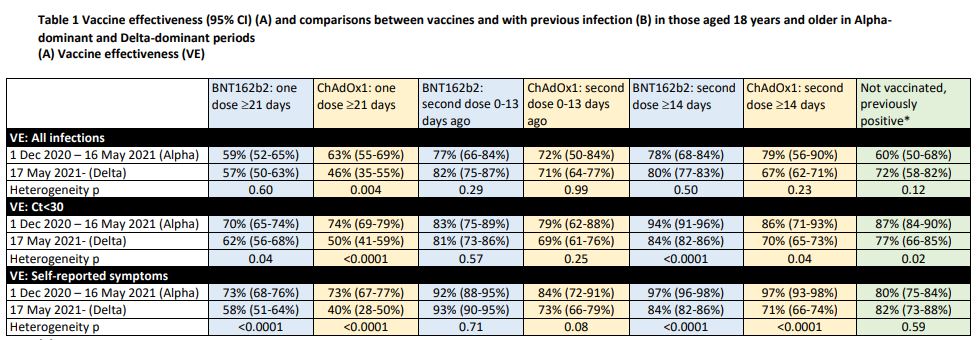
A second oddity is that for the all-infection (positive test) findings, the researchers found Pfizer VE was just 78% in the Alpha period, well below the usual figure – such as that from a major Israeli study, which put it at 92%. But then the researchers found it rose to 80% in the Delta period. A third oddity is that AstraZeneca VE was 71% in the 13 days after the second dose, up from 46% after the first dose even though that’s before the second dose is supposed to kick in. Yet once it is supposed to kick in, after 14 days, VE drops to 67%. These are strange results indeed.
Another perplexing aspect is that the VE estimates against Delta in this study, while (mostly) lower than against Alpha, are much higher than those indicated by recent data from Israel and the U.K., which have included 39% and 17%.
These various oddities piqued my suspicions, so I had a look at the raw data (shown below).
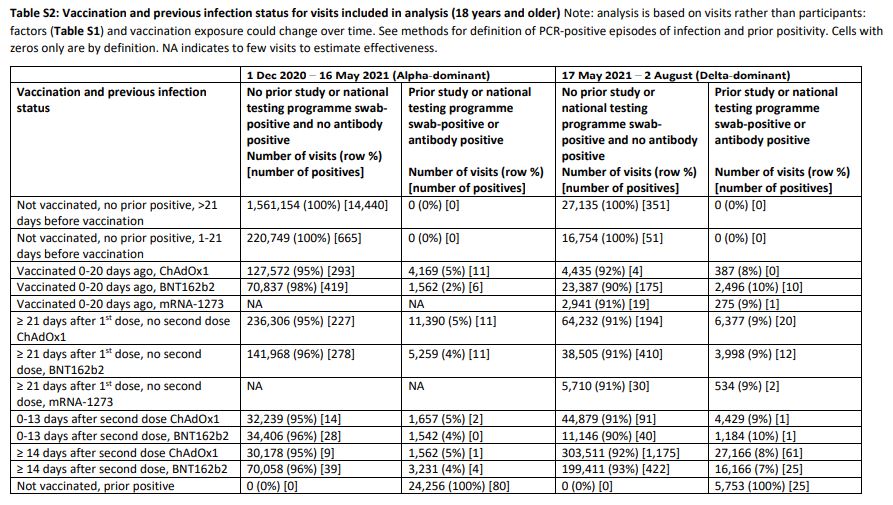
I converted some of these figures into positivity rates to get a clearer idea of where the VE results were coming from. I also added an unadjusted calculation of VE, given as 100% minus (vaccinated positivity/unvaccinated positivity). This assumes those tested are representative of the population, but since the purpose of the ONS Infection Survey is to survey a representative population sample this assumption didn’t seem unreasonable as a first pass.
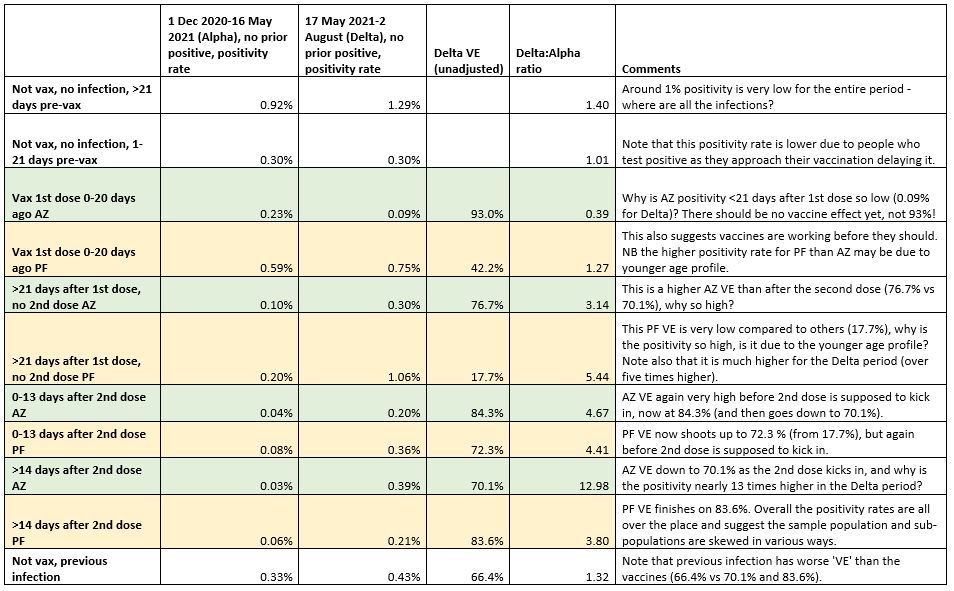
As can be seen (I have included comments in the table) these positivity rates and VE scores are all over the place. AstraZeneca VE hits 93% before the first dose is supposed to kick in, then drops to 76.7% as it kicks in, then rises to 84.3% before the second dose kicks in, and drops again to 70.1% as it kicks in. For Pfizer, we find the vaccine ‘working’ again before the first dose is supposed to kick in, with VE of 42.2%, but dropping to 17.7% as the first dose is supposed to start working, before rising to 72.3%, but again before the second dose is supposed to kick in, then rising to 83.6% as the second dose comes on line. Surprisingly, previous infection is found to be only 66.4% effective against new infection on these figures, lower than the vaccines.
The researchers adjust these raw figures for a large number of “potential confounders” (though not calendar week or background prevalence).
The following potential confounders were adjusted for in all models as potential risk factors for acquiring SARS-CoV-2 infection: geographic area and age in years (see below), sex, ethnicity (white versus non-white as small numbers), index of multiple deprivation (percentile, calculated separately for each country in the UK), working in a care-home, having a patient-facing role in health or social care, presence of long-term health conditions, household size, multigenerational household, rural-urban classification, direct or indirect contact with a hospital or care-home, smoking status, and visit frequency.
Even so, as we have seen, their results still don’t make much sense or correspond well with other studies. One problem is that the survey doesn’t appear to be finding very many infections at all – an overall positivity rate of around 1% in the unvaccinated both over the winter and in the Delta surge is very low given that most estimates find that around 10-15% of the population was infected in each period. However, this may be because they are testing each person several times before they test positive. Another point is that just 6% of the ONS survey tests during the Delta period were in the unvaccinated (43,889 out of 742,019), which is very low as a much greater proportion of the country between May and August was unvaccinated.
The main conclusion must be that the ONS sample is not suitable for this study. It is not representative enough of the population since it throws up implausible results even after adjustments, and requires too much adjusting, which is always a process riddled with guesswork and no substitute for starting with a better sample. This leads to further questions about how suitable the ONS sample population is for estimating infection prevalence as well.
The researchers also found that viral load, and thus likely infectiousness, is no lower in vaccinated than unvaccinated people, adding to the evidence that vaccination is not something that does much to protect others, undermining the case for vaccine passports, coercion and the vaccination of children.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Please watch and share this video – Reiner Fuellmilch and Mike Adams. Its about an hour long but is very worthwhile.
https://www.bitchute.com/video/q1ip5NDD6tJS/
Good peer review – one wonders whether any other peer review has been done. You do not say.
Not that so called academics are capable of doing it – but it might be better to just admit the study didnt produce clear conclusions, publish the data with the caveats above, as data is always useful even if not informative, and start again. What is not recommended is publishing clear conclusions that appear not to be fully supported by the evidence.
Possibly because most of those “previous infections” were false positive tests.
Its time to bring this nonsense to a close, tell the government to go hang and take back our lives. They’ve stolen enough from us!
As evidenced in recent news from New Zealand: Cases keep rising despite lockdown. Because of this, we need more lockdown!
Classic example of a bunch of one-trick-ponies lost in deep space.
I certainly look forward to the day when the government go hang.
Why would a random sample of a number of people much smaller than the population itself provide any kind of useful insight? The methodology is inherently fucked, or, to paraphrase Donald Knuth, a sequence of 200,000 snake eyes (throwing two dices and ending up with two ones) is perfectly random. That doesn’t mean it’s representative.
A random sample of people either forced or stupid enough to get tested.
They get paid! And they got offered an antibody test that is otherwise reserved for people in specific jobs.
Why would a random sample of a number of people much smaller than the population itself provide any kind of useful insight?
The size of the sample is what matters, not the size of population, and this sample size was very large. It is quite common to assume an infinite population size.
You’re really a fan of contradicting yourself in a single sentence, aren’t you? If the population size doesn’t matter, the sample size cannot possibly matter, either.
Eg, to use a contrived example, assuming a population size of six and a sample size of one, it must be prefectly reasonable to conclude that the outcome of a single roll of a dice will always be the outcome of any roll of a dice. That’s nonsense because there are six possible outcomes but only one was observed.
I think you need to read an introduction to statistics text book. This one is excellent and very cheap: https://www.amazon.co.uk/Elements-Statistics-Dr-Kevin-McConway/dp/0201422786. Almost all estimation of a population parameter assumes an infinite population. The population is treated as a probability density function (for continuous values) or a probability distribution function (for discrete values) with a parameter of interest (e.g. proportion vaccinated). This determines the probability of different samples given the value of the parameter. The size of the population plays no role in this.
There are exceptional circumstances where the population is very small, and where the sample is withdrawn from the population once taken, where the population size would matter – that is rare and totally irrelevant to the context of this study.
That’s not the problem.
Random sampling is the accepted way of testing any hypothesis, and is based on basic probability.
I think you need to do a bit of reading, as your misunderstanding is profound.
Your wrongness leads to the conclusion that there is no validity in the effectiveness of Ivermectin, either!
Just 6% of the ONS survey tests during the Delta period were in the unvaccinated
I think that was because they were visits not people. The same person might be visited once when unvaccinated and then later they would be vaccinated – but not the other way round!
From the paper (my emphasis):
During the Alpha-dominant period from 1 December 2020 to 16 May 2021 (Figure S1), nose and throat RT-PCR results were obtained from 384,543 individuals aged 18 years or older (221,909 households) at 2,580,021 visits (median [IQR] 7 [6-8]), of which 16,538 (0.6%) were the first PCR-positive in a new infection episode. During the Delta-dominant period from 17 May to 1 August 2021, results were obtained from 358,983 individuals (213,825 households) at 811,624 visits (median [IQR] 2 [2-3]), 3,123 (0.4%) being the first PCR-positive.
So, what you’re saying is that the bias in the testing is that:
So, maybe the ‘vaccine effectiveness’ in the young is higher simply because the ‘most scared’ have been vaccinated first.
Maybe the ‘vaccine effectiveness’ in the older age groups is lower simply because nearly everyone has been vaccinated (whether scared or not).
Who knows. Certainly not the scientists doing this research, because they’ve tried very hard to ignore such effects, even though they could have been estimated by being more careful in how the research was conducted.
I could find no mention of symptoms in the data. It seems that any old positive test will do, people don’t have to be ill. This, in my view, has enormous implications for transmissibility despite all the latest scaremongering about viral load being the same whether vaxed or not.
More PCR based junk science.
Publicly Funded Propaganda…
No official confirmation of this yet, but there are reports that at least 2 Australian kids have died following the herding of 24,000 kids into a stadium, without their parents, to receive the experimental jabs.
That info got out? So the true numbers could be rather higher.
CDC Director Dr. Rochelle Walensky just stated in a recent ‘Covid-19 Response’ video there is:
“Increased risk of severe disease among those vaccinated early.”
Because this was never about taking a single injection and getting back to normal.
You will take regular booster shots to keep your vaccine passports valid like good little slaves.
Why is no one in Ireland reporting this story?!
It was reported…sort of.
It had to be because he was so well known. They simply said
“Talented Sportsman dies an untimely death after a short illness.”
No details of what the short illness was.
You can see the hugotalks.com video about this here…needless to say he’s not impressed.
https://brandnewtube.com/watch/ireland-footballer-23-dead-from-jab-msm-cover-it-up-hugo-talks-lockdown_vV5TwFZ9jtnbYlV.html
Please stop what you are doing and look at this chart.
It shows that the explosion in #covid19 variants happened as a direct result of the introduction of #covidvaccines. This was entirely predicted by @GVDBossche and this is proof.
https://twitter.com/arkmedic/status/1428631348911112200?s=20
This was obvious even before the official rollout. The AZ trials were held in the U.K., Brazil & South Africa. The first 3 ‘variants’ bore the same names, duh, face plant!!
The strategy to universally vaccinate in the middle of the pandemic is bad science and badly needs a reboot.This strategy will likely prolong the most dangerous phase of the worst pandemic since 1918 and almost assuredly cause more harm than good – even as it undermines faith in the entire public health system.
https://www.washingtontimes.com/news/2021/aug/5/biden-teams-misguided-and-deadly-covid-19-vaccine-/
Bad science or good strategy? The answer is obvious.
It is impossible to make any sense of anything to do with Covid-19 because ALL of it is corrupted by lies, errors and biased modelling / predictions.
For example, if PCR testing was wildly inaccurate, the pandemic has just been a figment of machination.
The only thing we really know is that there exists a fanatical desire to get a genetic chemical into the systems of all of us despite there being no need for it. Quite why they want to do this is an unknown, but it can only realistically be one of two things: 1) CCP style social control, or 2) Depopulation.
They were never that effective. It was all bullshit.
This amazing lady Anna De Buisseret represents one of the best hopes the UK has right now – a senior lawyer working with a team to take the legal fightback to the next level. They are serving notices of liability on UK vaccinators – if they continue to vaccinate without obtaining full informed consent, they are going to be prosecuted under Nuremberg and many other laws. Very interesting development
ANNA DE BUISSERET SERVES NOTICE OF CRIMINAL LIABILITY ON UK COVID VACCINATORS UNDER NUREMBERG CODE
https://www.bitchute.com/video/ITZ5hqqkqOzZ/
Credit to the reddit site.
This virologist from the Crick institute says that Pfizer vax leads to a LOWER number of neutralising antibodies.
Why is he so upset and tearful just before he answers interviewers question?
Why does his research (which he says shows that the Pfizer jab diminishes immunity) lead him to conclude that we must use boosters?
It increasingly appears that these vaxxines/genetic medications have no benefit, and may be harmful.
https://www.gettyimages.co.uk/detail/video/dr-david-bauer-interview-francis-crick-institute-gvs-news-footage/1325046154
Coronavirus: Dr David Bauer interview / Francis Crick 4th June 2021
Q: Looking at vaccines, what have you found? –
So they key message from our finding Pfizer, those who have had 2 doses, have 5-6 fold lower of the neutralising antibodies. Block virus from getting into cells in first place. 1 dose less likely to have See older you are, lower levels likely to be Time since 2nd jab, lower likely to be Shows need to prioritise boosters for older.
I think the interview linked to above relates to this research paper.
And the interview (prior to editing) must have included a discussion of the immunity generated to the new “variants”
The SARS-CoV-2 B.1.617.2 Variant of Concern (VOC)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8175044/
However, NAbTs were 5·8-fold reduced against B.1.617.2 relative to Wild-type (95% CI 5·0–6·9), significantly more reduced than against B.1.1.7 (2·6-fold vs Wild-type, 95% CI 2·2–3·1), and on a similar order to the reduction observed against B.1.351 (4·9-fold vs Wild-type, 95% CI 4·2–5·7).
Notably, across all variants, increased age significantly correlated with reduced NAbT ; −0·33<RS<–0·27; 2·2 × 10−5<p<5·6 × 10−4), whereas no correlation was observed for sex or body-mass index ). NAbTs reduced over time after administration of the second dose of BNT162b2: participants (n=14) who attended an additional study visit 8–16 weeks after their second BNT162b2 dose showed significantly reduced NAbTs against all variants
So this video clip is discussing the efficacy of the Pfizer vax against the new variants, and finding that the original vax does not produce an effective antibody response.
The impact of such a change is challenging to predict: it remains difficult to assess precisely to what extent the reduction in NAbTs we observe will impact vaccine efficacy and increase disease severity in a vaccinated population, especially given the multiple factors that contribute to this process, such as long-lived humoral immunity.3
Nevertheless, a recent analysis of available NAb and vaccine efficacy data4 has attempted to establish correlates of protection against earlier strains of SARS-CoV-2 and, in the context of this model, our data suggest that most participants that received two doses of BNT162b2 would be protected against B.1.617.2 infection and associated disease
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8175044/
Could be suggestive of a form of ADE? Because natural immunity would be effective against the variants. No mention of non-neutralising antibody levels rising in this paper.
It’s getting boring now the ” vaccine efficacy” story. It doesn’t fit the legal definition of a vaccine. It’s an experimental gene therapy still in trials. And here’s a FACT. No one actually needs an experimental gene therapy for a virus that has never been properly proven to exist and has never been isolated following proper protocols. Not saying people haven’t been sick and died- it’s life, it’s normal and it’s normal to get sick and for some to die of colds. flu, pneuomonia and many other viruses. Some years it can be many many thousands such as in 2018. Yet according to NHS whistleblowers they stopped testing for flu and they have the audacity to say it dissapeared yet miraculously this year (to cover up vax adverse reactions) it is going to be terrible. You can’t make this stuff up and the fact that people are that stupid to believe it all without doing some due diligence is mind boggling. FACT- studies have shown that the flu jab increases the chances of being sick from respiratory illnesses by 4 fold and soon they will be pushing that. FACT- this virus (if it exists at all) and all respiratory viruses can be prevented, reduced and treated by following a healthy lifetstyle and diet and taking appropriate support if needed such as Vit d3, c, zinc, quercetin etc and various medicines that have been approved for years. So people can talk and write about efficacy all they want but these vaccines are not a vials of vitamins and are killing and harming a great many all over the World.
I just don’t believe anything those in ‘officialdom’ say anymore.
In the words of the song… “There may be trouble ahead”…..
“A new study finds billions of vaccinated people are at real risk of suffering Antibody-Dependent Enhancement.”
“Since the 1st February 2021 and the 15th August 2021, there have been 390 deaths among the unvaccinated population, an increase of 137 on the last count made.”
“Up to the 15th August 2021, the fully vaccinated population has suffered a total of 679 deaths. This in an increase of 277 on the previous report.”
https://dailyexpose.co.uk/2021/08/21/study-finds-vaccinated-are-at-real-risk-of-suffering-antibody-dependent-enhancement/
https://www.bitchute.com/video/qHNixLWRxAwN/
Interview with Mike Yeadon. Seems to be fairly recent.
Warrant out for arrest of Delores Cahill:
https://extra.ie/2021/08/18/news/irish-news/dolores-cahill-uk-arrest-warrant
But we can always fall back on the MASK. Most people seem to have sussed out that it really doesn’t do anything to stop a virus – Chicken wire to a Mosquito – BUT because the BBC etc. recommenf it – err well perhaps i’ll give it a try ????????
Inexplicable findings?
New Normal Science requires the firm simultaneous belief in at least two mutually exclusive ‘explanations’ for any event.
Then nothing is inexplicable.
FIGHT. BACK. BETTER. Updated information, resources and links: https://www.LCAHub.org/