Rayner Backs Down in Islamophobia Free Speech Row
By Will Jones

Angela Rayner has backed down on “secretive” plans for a new definition of Islamophobia, expanding and extending a public consultation on the proposals, after the Free Speech Union threatened legal action. The Telegraph has more.
The Deputy Prime Minister has expanded and extended a public consultation over the proposals, which critics fear will rubber-stamp a controversial definition.
The consultation will now run for an extra week and a link for responses to the plans has been made public.
The move followed complaints by the Free Speech Union (FSU), which said the new definition was being drawn up behind closed doors.
The FSU wrote to Ms Rayner expressing concern that the process would enshrine a definition which treats Islamophobia as a type of racism.
The definition has been criticised for being so expansive that it could threaten free speech, act as a de facto blasphemy law and stifle legitimate criticism of Islam as a religion.
In his letter, Lord Young, the General Secretary of the FSU, said the consultation questions appeared to be “heavily weighted” in favour of a “predetermined outcome”, endorsing a definition “closely aligned” with that put forward by the all party parliamentary group (APPG) on British Muslims.
The APPG definition was adopted by Labour and stated that “Islamophobia is rooted in racism and is a type of racism that targets expressions of Muslimness or perceived Muslimness”.
Lord Young said key groups that might challenge the definition over its impact on free speech and provide alternative views had not been invited to submit evidence.
He listed Christian Concern, the Christian Institute, the Adam Smith Institute and the Equality and Human Rights Commission.
Ms Rayner’s department has extended the deadline to July 20th and widened the consultees. Lord Young said it needed to give sufficient time to take on board all the responses to the plan.
Worth reading in full.






The Economic Illiteracy of UK Energy Policy is a Sight to Behold
By Tilak Doshi

It seems that economic illiteracy is now a job requirement for leadership positions in the country’s energy policymaking. Few spectacles rival the ongoing comedy of errors that is the United Kingdom’s energy strategy under the stewardship of Michael Shanks, the Parliamentary Under-Secretary of State for Energy since July 2024, and his superior, Secretary of State for Energy Security and Net Zero, Ed Miliband. Mr Miliband has been derisively dubbed ‘Mad Ed‘ by those who see through the haze of eco-utopian rhetoric. Mad Ed’s economic and energy illiteracy has already been the subject of several articles in these pages (here and here).
Mr Shanks’s recent claim that there is “no material difference” between importing oil and gas and producing it domestically in the North Sea is not just a misstep; it is economic illiteracy, a statement so divorced from basic economic principles that it would make an Econ 101 student blush. This is not merely a gaffe but a symptom of a deeper malaise: a leadership that prioritises ideological posturing over the prosperity and security of the British people.
Mr Shanks – with a degree in history and politics and a working background in teaching ‘modern studies’ at a high school and ‘community’ and ‘charity’ work – has no obvious qualifications to hold a senior leadership position in energy affairs of the country. But that seems to present no problem for this Government.
Mr Shanks’s boss, Mr Miliband, alas, fares no better, oblivious to the economic devastation his policies invite. Together, the duo embodies a dangerous trend: the elevation of economic illiterates to senior policymaking roles in a sector critical to the UK’s survival.
The Aberdeen & Grampian Chamber of Commerce Morning Bulletin July 4th
Let us begin with Shanks’ stunning assertion, reported by the Aberdeen & Grampian Chamber of Commerce on its Friday morning bulletin. Mr Shanks believes there is no “material difference” between oil and gas imports and UK’s domestic North Sea production.
This claim is not just wrong; it is economically absurd. Any first-year economics student could recite the basic tenets of gross domestic product (GDP) accounting: domestic production adds to GDP, while imports subtract from it. The North Sea oil and gas industry, despite its decline since its 1999 peak, remains a cornerstone of the UK economy, contributing approximately 50% of the nation’s oil and gas needs, supporting 200,000 jobs and generating billions in tax revenue.
In 2022, North Sea producers handed the Treasury nearly £10 billion in windfall taxes alone, a fourfold increase from £2.6 billion the previous year, thanks to elevated global energy prices following Russia’s invasion of Ukraine. To suggest that importing the same resources — often from Norway, a country that sensibly continues to drill and profit from its own North Sea reserves with properties right beside the UK’s — is equivalent to domestic production is to ignore the economic multiplier effects of local industry: jobs, investment, tax revenues and energy security.
To this day, neither ‘Mad Ed’ nor his sidekicks like Shanks have explained just how importing oil and gas from neighbouring Norway is superior to having Britain produce its own oil and gas from properties in the North Sea adjoining that of Norway’s. How can someone sucking on the milkshake straw in the same glass that I have my straw in be told that, “yes, go ahead, young man, suck it all out, but I can’t because I am the good guy”. Is there a stranger story for my ‘I can’t make it up even if I tried’ file?
The North Sea still holds an estimated four billion barrels of oil equivalent, capable of meeting half of the UK’s oil and gas needs through 2050 and contributing £150 billion to the economy. Yet, under Miliband’s ideological crusade and Shanks’ imbecilic complicity, the Labour Government has chosen to throttle this vital sector.
Labour’s ban on new North Sea licences, coupled with punitive taxation — offshore producers face an effective tax rate of 78% — has accelerated the decline of domestic production at a staggering 11% per year, more than double the rate forecast before these policies took hold. The result? Britain is now haemorrhaging jobs, investment and energy security.
Contrast this with Norway, the UK’s neighbour across the North Sea, which Shanks and Miliband seem to view as a model for outsourcing Britain’s energy needs. Norway, a social democratic state, has no qualms about exploiting its natural resources. Its state-owned energy giant, Equinor, recently inked a £20 billion deal with British Gas owner Centrica to supply gas to the UK, a deal that underscores the absurdity of Miliband’s policies.
Norway drills, sells and grows rich, maintaining balanced budgets, pristine public services and a sovereign wealth fund swollen with petrodollars. Meanwhile, Britain, under the stewardship of Shanks and Miliband, shutters its own fields, exports jobs and imports gas at a higher carbon footprint. Piping it hundreds of miles across the North Sea adds emissions, not reduces them. This is not just economic self-harm; it is environmental hypocrisy dressed up as virtue. But hey, the Labour Government can claim in international circles that the UK is a ‘climate leader‘.
Where did these guys learn what they did?
Michael Shanks’s educational background offers a clue to his baffling pronouncements. With a degree in history and politics, his expertise lies, perhaps, in teaching ‘modern studies’ in high schools – as he in fact did. His stint as a high school teacher and ‘community and social work’ does not equip him to navigate the complexities (or for that matter, simplicities) of energy economics. His career trajectory hardly equips him to grapple with the basics of GDP contributions, energy security or affordable electricity.
Instead, he finds himself out of his depth, parroting Miliband’s Net Zero dogma without questioning its economic fallout. His claim that imports and domestic production are materially equivalent betrays a fundamental misunderstanding of trade balances and economic multipliers. Imports drain national wealth; domestic production builds it. This is not rocket science — it’s basic economics.
Ed Miliband, Shanks’ boss, is no less culpable. His Oxford degree in Philosophy, Politics and Economics (PPE), ‘the degree that rules England‘, might suggest a grasp of economic principles, but his tenure as Energy Secretary reveals a man more enamoured with climate ideology than with practical governance. Dubbed ‘Mad Ed’ by critics like Net Zero Watch’s Andrew Montford, Miliband has earned this moniker through a series of economically disastrous decisions: shutting down the UK’s last coal plant, rushing approvals for solar farms over community objections, and capitulating to Greenpeace lawsuits that jeopardise North Sea investments.
His refusal to defend a legal challenge against drilling in the Rosebank field, which holds 500 million barrels of oil, exemplifies his priorities: appeasing eco-activists over safeguarding jobs and economic growth. Miliband’s policies have already cost the UK its place among the top 10 manufacturing nations, a ignominious first in its industrial history.
The economic illiteracy of this duo – Miliband and Shanks – manifests most starkly in their failure to recognise the strategic folly of import dependence when the country is blessed with oil, gas and coal resources. By choking off North Sea production, they leave Britain vulnerable to global energy shocks. When Russia invaded Ukraine, oil prices soared, and the UK’s domestic producers provided a critical buffer, funnelling billions in tax revenue to the Treasury.
Miliband’s claim that renewables will shield Britain from “petrostates and dictators” ignores the reality that ‘clean’ energy technologies — wind turbines, solar panels, batteries — rely on critical minerals controlled by countries like China. Trading a relatively diversified dependence (oil and gas imported mainly from the US, Norway and Qatar) for another one focused on China (which dominates the solar, wind and EV battery supply chains) is not security; it’s an idiocy which seems to have no problems with a ruling communist party-run country as the preferred partner.
The environmental argument for importing over producing domestically is a sham. Reducing the UK’s carbon footprint by pushing its manufacturing base out to China and elsewhere does reduce territorial carbon emissions. It is something that Keir Starmer and Ed Miliband can boast about in fancy circles of diplomats and virtue-signalling magnates gathered around Davos and UN COP meetings. But the carbon footprint of Britain that consumes energy-intensive products from China and other countries nonetheless has little impact on global emissions which are all that matter – assuming you buy into the narrative that the climate future of the globe is controlled by CO2 levels in the atmosphere.
Transporting gas from Norway or liquefied natural gas (LNG) from further afield like the US or Qatar generates higher emissions than extracting it locally. A Deloitte study estimated that exploiting domestic gas fields, such as the untapped Lincolnshire shale gas reserve, could significantly reduce CO2 emissions compared to imports. Yet Miliband, with Shanks’s apparent concurrence, dismisses such opportunities, leaving billions in potential GDP and tax revenue underground while pensioners freeze due to soaring energy bills. The GMB Union, a Labour ally, has called this approach “bonkers” and “absolute madness”, warning of catastrophic job losses and environmental harm. Even Labour’s own supporters see the insanity of this policy.
God Save This Nation
The social cost of this economic illiteracy is staggering. UK energy bills, already among the highest in the developed world, are set to rise further, with Ofgem announcing price cap hikes. Miliband’s promise to cut household bills by £300 through his Net Zero policies has vanished, replaced by vague talk of a “positive vision”. Blaming high energy bills on high natural gas prices is bogus on the face of it as has been incontrovertibly shown by experts like Kathryn Porter and David Turver and as natural gas prices have gone back to the low levels prior to the Ukraine war.
Meanwhile, the closure of Grangemouth, Scotland’s last oil refinery, and the decline of Aberdeen’s oil sector signal a broader industrial collapse. Steelworks and car factories are buckling under high energy costs, and pensioners face cuts to winter fuel payments while the Government pledges £22 billion for unproven carbon capture technologies.
The irony is that renewables, which Miliband champions, are not yet ready to replace fossil fuels – nor are they likely to be in any credible scenario. On days of low wind or sun, gas-powered stations provide up to 75.4% of the UK’s electricity. Even by 2030, the UK will need 42 billion cubic meters of gas annually. Miliband’s rush to decarbonise by 2030 ignores this reality, risking blackouts and further bill hikes
What, then, is to be done? First, Shanks and Miliband must be held accountable for their economic ignorance. Shanks’ lack of expertise disqualifies him from advising on energy policy; he should step aside or be reassigned to a role befitting his actual talents.
Miliband, for his part, must abandon his ideological crusade and adopt a modicum of economic sense. The Government should reverse the ban on new licences, reduce punitive taxes on North Sea producers, and prioritise domestic energy over imports. Fracking, too, should be revisited — Lincolnshire’s shale gas could fuel the UK for seven years, adding £112 billion to GDP and saving lives by lowering energy costs.
The UK stands at a crossroads. It can follow Norway’s path of pragmatic prosperity or continue down the current economically imbecilic road to economic ruin. The choice is clear, but it requires leaders who understand basic economics — not climate zealots or PPE dilettantes. The British people deserve better than to be governed by those who don’t know the difference between producing domestically and importing. It is time to end this embarrassing charade and restore sanity to UK energy policy.
Ed Miliband and Michael Shanks have not provided leadership in energy policy; it is ideological miasma. It’s like Rousseau expecting Voltaire to walk on all fours to re-discover the noble savage within.
Dr Tilak K. Doshi is the Daily Sceptic‘s Energy Editor. He is an economist, a member of the CO2 Coalition and a former contributor to Forbes. Follow him on Substack and X.
No, 170 Londoners Didn’t “Die of Climate Change” Last Week
By Will Jones

According to Imperial College and the London School of Hygiene and Tropical Medicine, 170 Londoners died due to climate change in last week’s heatwave. But it’s just more modelling make believe, says Ross Clark in the Spectator. Here’s an excerpt.
So, 260 Londoners died as a result of last week’s heatwave, of which 170 can be attributed to climate change. So claims Imperial College and the London School of Hygiene and Tropical Medicine.
There’s just the one problem with this: the researchers haven’t actually counted any deaths at all. The study rushed out this week is nothing more than a piece of modelling, which estimates the number of deaths which might be expected to have been caused by the hot weather, as well as trying to guess how much hotter last week’s weather was than it would have been without man-made climate change. We won’t know whether there really were any excess deaths during the hot weather until the Office for National Statistics (ONS) publishes its figures in a few weeks’ time.
Why rush out a piece of modelling when we will shortly have some real-world data? The researchers will have to explain their reasoning, but it is as well to note that both the participants in this study have a bit of previous when it comes to modelling alarming numbers of deaths.
Both were heavily involved in modelling during the Covid pandemic. Many of their predictions were not able to be tested against real data: we will never know, for example, whether 500,000 people really would have died of Covid were it not for social distancing measures – as Imperial College claimed in its paper of March 16th 2020 – because, of course, the government did impose a lockdown.
But towards the end of the crisis, one prediction was able to be tested against reality. On December 11th 2021, the London School of Hygiene and Tropical Medicine put out a paper claiming that 24,000 people would die as a result of the Omicron variant of Covid, with daily hospitalisations peaking above those in January 2021, unless the government introduced a return to lockdown -style measures. Perhaps it was counting on ministers taking its advice, but in the event the cabinet resisted – and the prediction was exposed for what it was: a gross exaggeration.
Worth reading in full.
Why are Taxpayers Being Charged £1.2 Million for ‘Inclusive’ GCSE History?

Is the history curriculum ‘diverse’ enough? Apparently not, according to a group of university researchers who’ve been awarded £1.2 million in taxpayer funding for their project ‘Inclusive Histories’.
The three-year project is being led by Royal Holloway and the AQA exam board, so as to “inform future GCSE specification reform at AQA and other awarding bodies”. AQA is one of the three main GCSE exam boards in England, Wales and Northern Ireland (along with Edexcel (Pearson), OCR and WJEC (Welsh Joint Education Committee). It marks up to half of all GCSEs and A-levels taken in the UK every year.
The abstract makes clear what problem the researchers are trying to solve, claiming that “the taught curriculum for secondary schools often fails to incorporate new, diverse histories, acting as a barrier to Global Majority Engagement”, and that students themselves are calling for “better representation of gender, sexuality, disability, neurodiversity and class [and] the intersectionality of these identities and lived experiences”.
Inclusive Histories will support the AQA specification “Britain: Power and the People c1170 to the present day”, charting “the struggle for rights of representation from Magna Carta” to now.
With the project beginning in September last year and due to finish the same month in 2027, the syllabus isn’t currently available to peruse. But you can get a sense of what might be involved from examining some of organisations involved, listed below:
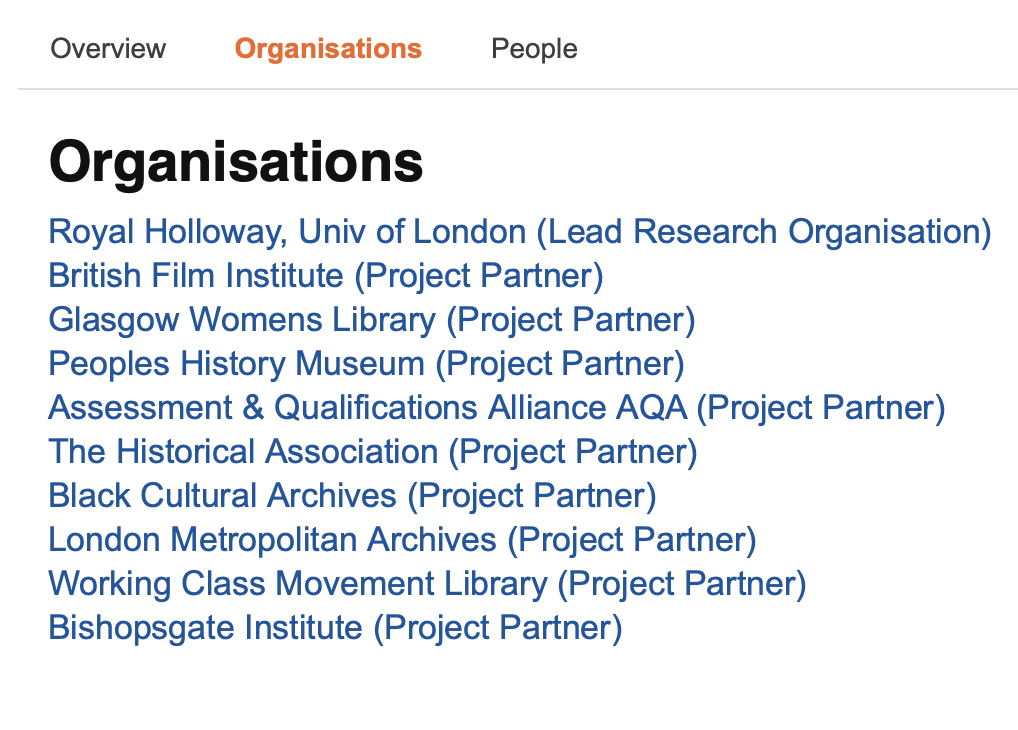
I’ve had a nose around some of their websites, to get an idea of what their ideas of ‘inclusivity’ look like. Today I shall spoil Daily Sceptic readers with what I found:
The Glasgow Women’s Library
The GWL looks innocuous enough, until you go onto its social media account and spot that it’s been deemed a “Library of Sanctuary”, a status “awarded to libraries that go above and beyond to create welcoming, inclusive, and empowering spaces for people who have experienced forced displacement.”
To add, I recently wrote about “Boroughs of Sanctuary” for the Daily Sceptic, which is effectively an open-borders scheme imported from the US Democrats.
The GWL has also praised Nicola Sturgeon and curated books for LGBTQ+ History Month, including “a feminist inclusive anti-racist non-binary field guide for graphic designers”.
People’s History Museum
Based in Manchester, the People’s History Museum describes itself as “the national museum of democracy”. Its website has resources for ages seven-plus on the Peterloo Massacre and Migration, the latter including animations on “the lived experiences of people who have migrated to the UK” and the tale of “Melina, who sought asylum in the UK due to facing discrimination based on her sexuality”.

The Black Cultural Archives
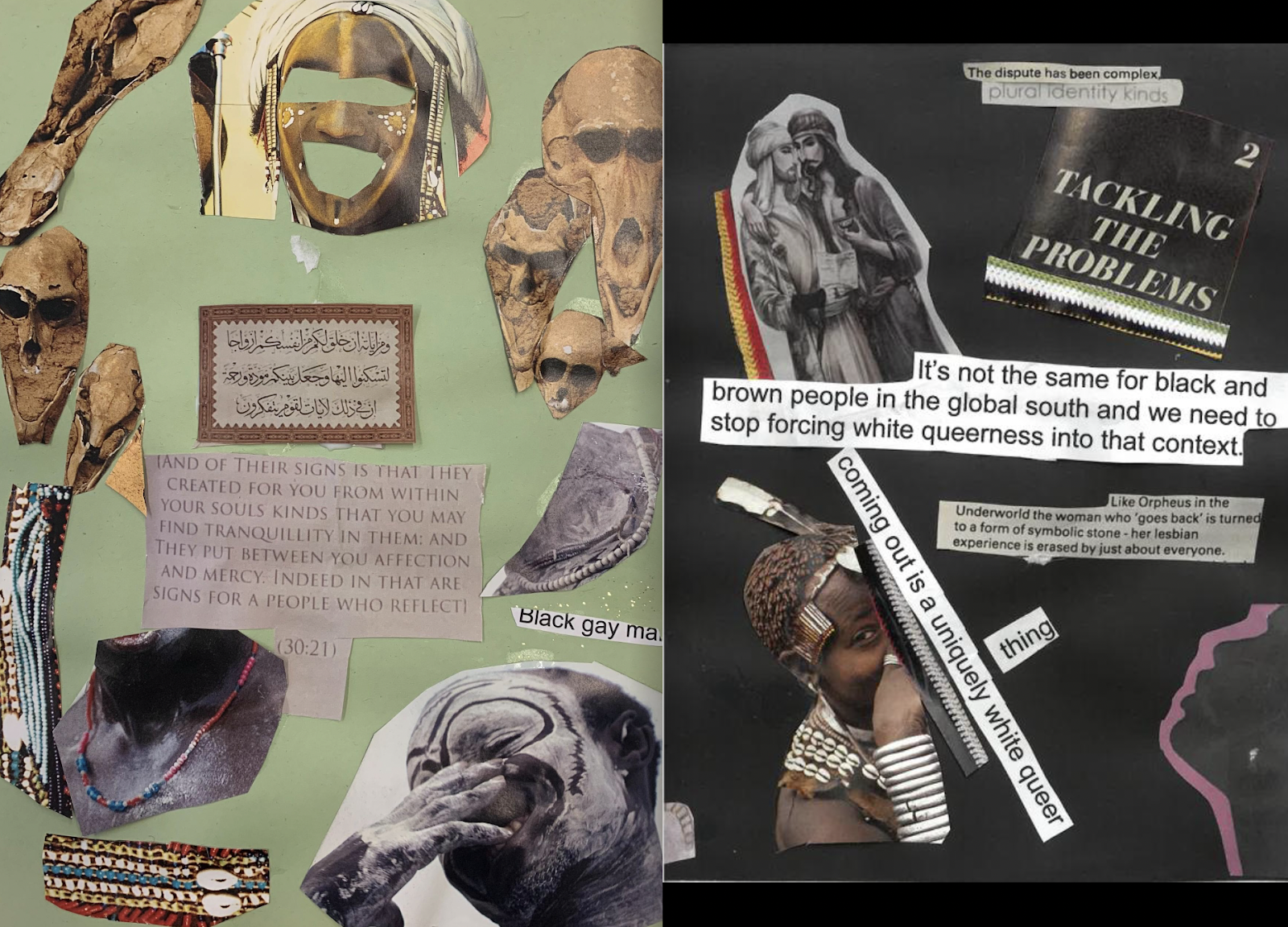
The organisation already runs its own Youth Programme, which gives an insight into what could soon be on AQA’s curriculum. In 2025, for instance, the Black Cultural Archives projects “explored the history of Brixton’s Black LGBTQ+ community” and students made a “commemorative zine” titled ‘Black, Queer, Always Here‘. Here are screenshots of it:
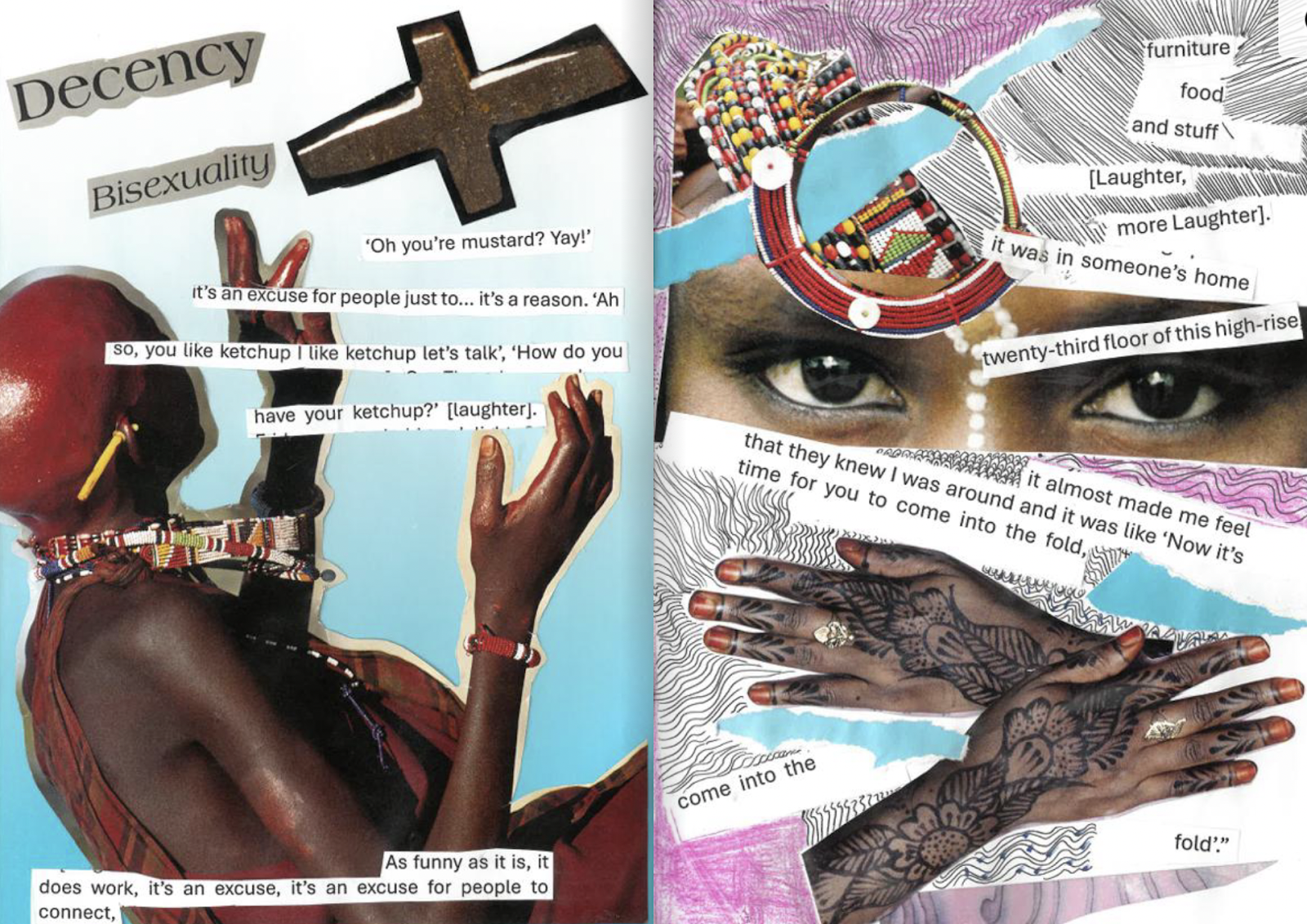
It includes a page which reads: “It’s not the same for black and brown people in the global south and we need to stop forcing white queerness into that context”; and “coming out is a uniquely white queer thing”.
Bishopsgate Institute
Another organisation involved in reshaping the curriculum is the Bishopsgate Institute, which “holds one of the most extensive collections of LGBTQIA+ history, politics and culture in the UK”. It has held events including ‘Queer Tango’ and ‘Desi Queers: LGBTQ+ South Asian and Cultural Belonging in Britain‘, as well as flying the trans-inclusive Pride flag to celebrate Pride Month:

So there you have it; this is just a sample of the institutions that will be reshaping children’s GCSEs. That’s before we get to some of the experts involved in ‘Inclusive Histories’, such as Dr Amy Tooth Murphy, whose research profile is below:
To add, ‘Inclusive Histories’ is funded by the Arts and Humanities Research Council, which is funded by the UK Research and Innovation, a department funded by the Department for Science, Innovation and Technology (all ultimately adding up to being taxpayer funded).
You can find out even more about AHRC in my previous piece for the Daily Sceptic: ‘If Rachel Reeves Wants to Fill the £22 Billion “Black Hole” She Should Start by Abolishing the Arts and Humanities Research Council.’
Charlotte Gill regularly publishes about the use of taxpayers’ money to fund Left-wing causes and Left-wing researchers in Woke Waste, her Substack. You can subscribe here.
Schools Ban Children From Playing Outside During Heatwaves
By Will Jones

Schools are banning children from playing outside during heatwaves, keeping them inside for ‘hot play’ breaks when their playgrounds are deemed to be ‘too hot to use safely’. The Telegraph has more.
The move is designed to keep children away from outdoor surfaces that can become very hot to touch in the sun.
But the concept has been branded “absolute nonsense” by critics, who warned that it risked raising a generation of “wimps” taught to “hide from warm weather”.
Schools routinely hold ‘wet play’ sessions when it rains, where children play indoors between lessons instead of going outside.
But ‘hot play’, which is the equivalent for heatwaves, appears to be a relatively new idea.
The practice has been highlighted by the WWF, the environmental group, which is calling for schools to use more natural surfaces, as opposed to artificial ones, to “mitigate the effects of extreme weather”.
Chris McGovern, a former head teacher and Chairman of the Campaign for Real Education, warned that keeping pupils indoors during hot weather was the “worst thing” for them.
He said: “I taught for 35 years. Any teacher knows that the worst thing you can do on a hot day is to keep children confined in the classroom. It’s about the worst thing you can do.
“Of course, there can be situations where a particular child needs to stay indoors, and of course there should be areas of shade within the playground. But using common sense, it’s the worst possible way forward for helping these children.
“Just as in cold weather, they should be out running around. So we’re making them into wimps. We don’t want to make children into wimps. We want to toughen them up a little bit.”
He also warned that constraints on children’s freedom risked damaging their mental health in the long term.
He added: “It’s an awful childhood we’re inflicting on children. And, of course, it encourages them to use their iPads and mobile phones if they’re confined.
“The worst thing they can be doing is staying indoors, playing on their mobile phones, and this is sort of encouraging them to do that. So yeah, it’s the opposite of what we want.”
Greg Smith, the Tory MP for Mid Buckinghamshire, said it was “absolute nonsense” to attempt to “wrap children in bubble wrap and away from anything that might be a bit uncomfortable”.
“The correct answer is to take precautions in heat – hats, sun cream, light clothing – not hide from warm weather,” he said.
Worth reading in full.
The French Handed the Migrants Over – Then Asked for Their Life Jackets Back
By Will Jones

On the day Starmer and Macron announce their ‘migrant deal’, the Telegraph joins Nigel Farage in the Channel to witness the French handing 78 migrants over to the British – though not before asking for their life jackets back. Here’s an excerpt.
In a calm sea under clear blue skies, a French navy warship on Thursday escorted a dinghy crammed with nearly 80 migrants to the Channel’s midpoint for a handover with UK Border Force. But not before demanding their life jackets back from the asylum seekers to reuse them on the next trip.
The ‘rescue’ of the 78 migrants took little more than 30 minutes.
It was almost as if it was routine, despite the dangers of crossing one of the busiest shipping lanes in the world with powerful tidal currents.
Of the 78 migrants who made it, 74 were men. There was just one woman on board with three children.
No more than 300 yards away, on a fishing boat bobbing in the sun-specked water, was Nigel Farage, the Reform UK leader, marking the day when Sir Keir Starmer and Emmanuel Macron, the French President, announced their new deal to halt the crossings, in his own pointed political way.
“This is a classic day on the English Channel over the past five years when the sea is calm,” he said. “We are witnessing a crime but everyone seems happy.
“The French navy is happy. Border Force is happy. And what we saw was how calm and controlled it was, almost as if the two governments have agreed it is normal practice and can continue.”
The maritime operation began before dawn, when the French warship spotted the migrants’ flimsy overloaded dinghy with its balsa wood bottom as it left Wissant beach on the northern French coast. For the next 12 miles, the naval vessel escorted the boat ready for the migrants’ transfer to Hurricane, the Border Force cutter.
At a steady two to three knots, the boat made its slow progress through the calm but cold waters to the Channel’s midpoint by 7.30am before appearing to lose power. At that point, a rigid inflatable boat with sailors on board sped from the warship across the sea to recover the 40 life jackets earlier handed to the migrants by the French.
Observers said it was the first time they had seen life jackets recovered before the migrants had been towed and fully embarked on Hurricane. There was, however, no shortage of rescue backup with two British rigid inflatable boats accompanying the Border Force cutter.
Six vessels were involved in the handover, accompanied by a drone and at one point a helicopter, at a cost of tens of thousands of pounds. The sixth vessel was a large tug-like offshore supply boat with a winch, which lifted the empty dripping dinghy from the water to be taken back to Dover for forensic examination and storage. …
Mr Farage, who first highlighted the crisis by going out on the Channel over five years ago, said: “Nine years ago, the country voted decisively to take back control of its borders, to have an immigration policy that meant we could choose who came here.
“The most blatant betrayal of that is what you’ve just witnessed with me in the Channel: one vessel, 74 young undocumented males about whose history we know nothing entering the UK.”
In an interview with the Telegraph, he urged Sir Keir to declare a national security emergency to allow the Government to suspend the European Convention on Human Rights (ECHR) and Refugee Convention. This, he said, would then enable ministers to intern all illegal migrants in secure, converted former military camps.
“I would definitely intern everybody that arrives on the basis that not all, but some of them, will be dangerous. In recent weeks, we’ve seen suspected terrorists who came via Channel arrested. We’ve had the Casey report telling us child sexual grooming is carried on by people like this,” said Mr Farage.
“There might be some people here who are coming here from horrible backgrounds, but the first job of the Government is to protect the nation. The only way you stop this is by making people know that it’s not worth paying the trafficker out because you will be deported.
“And that’s what Rwanda was about. The problem is it couldn’t work because of Strasbourg courts, British courts, and the incorporation of ECHR into British law. It was never going to be a goer but the thinking behind it was right.”
One of his first acts, if he became Prime Minister – as the polls suggest is a possibility – would be to quit the ECHR. He declined to back Donald Trump-style mass deportations, but said there would be “significant” numbers and not just to “safe” countries but also nations like Afghanistan.
As a “last stop” he said he was prepared to bring in the Navy to forcibly return migrants at sea to France. “If we can’t solve this through other means, in the end the Royal Marines will have to take the boats back to France,” he said.
“Under the Law of the Sea, if lives are in danger, you can take them back to the safest place. It would be the ‘last stop’ measure. It would cause a diplomatic incident, as it did with the Australians in 2012 but it does work.”
Worth reading in full.
Britain “To Lose a Pub a Day” as Labour’s Tax Raid Bites
By Will Jones

One pub will close every day this year as Labour’s tax raid makes it “impossible to make a profit”, with 33% of sales revenue now going to the taxman, the British Beer and Pub Association has warned. The Telegraph has the story.
The British Beer and Pub Association (BBPA) predicted that 378 pubs will shut across England, Wales and Scotland before the end of the year – up from 350 closures last year.
It will take pub numbers to their lowest level in a century, the BBPA warned.
The body, which represents the pub industry, attributed the expected jump in closures to cost pressures on landlords. Worryingly, it said that for every £3 spent on pints and food in a pub, £1 now went straight to the taxman.
It comes after Labour launched a raid on pubs and retailers in the spring, pushing up employers’ National Insurance contributions (NIC) and lowering the threshold at which they needed to pay them.
The Chancellor also increased the minimum wage by 6.7% to £12.21 an hour from April, while changes to business rates have pushed costs even higher for pubs.
The BBPA has previously suggested the changes cost each UK pub about £14,000 on average.
On Thursday, the industry group warned that hundreds of pubs were now preparing to close their doors, which would lead to almost 6,000 jobs being axed by the end of the year.
Nigel Farage, the leader of Reform UK, labelled it an “absolute tragedy”.
He added: “Every publican that I’ve spoken to – and I’ve visited nine over the weekend in Clacton, just to go and chat and see how they’re getting on – every single person says that the NIC rise has taken away their profit. Every single one.”
Sir Tim Martin, the boss of pub giant Wetherspoon, said supermarkets were being allowed to undercut pubs and called for ministers to act.
Worth reading in full.
News Round-Up

- “Starmer and Macron agree ‘one in, one out’ Channel migrant swap pilot” – Sir Keir Starmer is facing serious questions over whether a new migrant returns deal agreed with France will make any difference to the Channel small boats crisis, reports the Mail.
- “‘I was a Border Force officer. Starmer’s ‘deal’ with Macron is worse than useless’” – There’s still no serious long-term plan for halting the increase in Channel crossings, let alone stopping them completely, says Tony Smith in the Telegraph.
- “Starmer and Macron won’t fix the Channel migrant crisis” – The sceptic might argue that the real problem in cracking the migrant crisis isn’t so much the criminal gangs as the human rights industry, writes Gavin Mortimer in the Spectator.
- “Starmer will rue the day he made Lord Hermer de facto deputy PM” – This is a Government of human rights lawyers, by human rights lawyers, for human rights lawyers, says Stephen Pollard in the Telegraph.
- “Cut benefits for depression and ADHD, Tories demand” – Kemi Badenoch claims that the Government could save up to £9 billion by cutting PIP and UC for claimants better off in work, reports the Mail.
- “Kemi is right. The benefits bill could cripple Britain” – In the Spectator, Michael Simmons says Badenoch is right on welfare – but not tackling pensions means Britain’s real crisis still looms.
- “Britain is killing itself with compassion” – A spiralling welfare bill, ballooning debt and political idealism are setting the stage for crisis, warns Sam Ashworth-Hayes in the Telegraph.
- “Moment police officer sobs after ‘being punched at Manchester Airport’” – The moment a female police officer was left sobbing and bleeding after being punched in the face during a brawl at Manchester Airport, has been shown in court, reports the Mail.
- “The unspoken truth about 7/7” – The way we have dealt with the 7/7 bombings is effectively to deny that they happened at all, says Rod Liddle in the Spectator.
- “‘My tips to avoid arrest by the Met’” – In the Spectator, Douglas Murray slams the Met’s double standards after 11 officers arrest a man for a sandwich board at Pride, suggesting he’d have been safer shouting “Jihad” or joining a grooming gang.
- “Heard the one about Rod Liddle and the police state?” – Brighton Council’s dullard Labour leader has reported Rod Liddle to the police over an obviously satirical column, writes Mick Hume in Spiked.
- “Peerless: the purge of the hereditaries” – In the Spectator, Charles Moore mourns Labour’s quiet purge of the hereditary peers.
- “Ofcom costs hit £4.6 million after losing GB News legal battle” – Ofcom’s spending on external advisers surged to £4.6 million last year after the watchdog lost a high-profile court battle against GB News, reports the Telegraph.
- “Starmer has pushed Miliband to make a rare good decision” – Plans for so-called zonal electricity have been quietly dropped following No10 scrutiny, notes Kathryn Porter in the Telegraph.
- “The true cost of our energy delusions” – In Net Zero Watch, Maurice Cousins warns that Britain’s crumbling energy policy has sabotaged its economy.
- “‘I tried circumnavigating the UK in an electric van – here’s why it was impossible’” – It’s green, it’s eco-friendly… and, as the Times’s Chris Haslam discovered, it can take up to six hours to charge. The road trip revolution is still a long way off.
- “Scotland’s tidal bet: Net Zero, net loss” – In WUWT?, Willis Eschenbach slams Scotland’s MeyGen tidal scheme as a £66 million vanity project that churns out power at ten times the price of gas.
- “A fresh start” – On Climate Scepticism, Robin Guenier argues that Britain’s Net Zero crusade is futile virtue-signalling in a world where global emissions are rising regardless.
- “2022-2024 warming mostly linked to natural factors, not CO2” – On the NoTricksZone, P. Gosselin reports that Prof Fritz Vahrenholt attributes recent warming to natural factors like El Niño and increased solar radiation, arguing that climate models overstate the role of CO2.
- “Al Jazeera wrongly hypes a climate connection to recent European heatwaves” – On Climate Realism, Linnea Lueken argues that Al Jazeera’s claims about worsening heatwaves and rising deaths ignore historic temperature data and overstate climate change’s role.
- “Natural gas is green and hugely beneficial economically” – In RealClearEnergy, Benjamin Zycher exposes the myths around green energy, showing natural gas is cleaner, cheaper and more reliable than renewables.
- “Dems’ climate pivot probably just smoke and mirrors” – Dems are dialling back some of their climate policies due to their mounting costs, but some policy analysts say the changes are merely symbolic, writes Melissa O’Rourke in the Daily Caller.
- “‘I’m a young meteorologist who questioned the idea of man-made climate change. The climate zealots wanted me punished, silenced and expelled’” – Science doesn’t support the theory that climate change caused the Texas floods, but any attempts to have science-based discussion about the issue are being repressed, says Chris Martz in the Free Beacon.
- “Texas soaked, Bloomberg smoked? Lefty billionaire blames ‘climate denialism’ for floods” – Lefty billionaire Michael Bloomberg is back in the spotlight exploiting the Texas floods to blow a gasket over his most obsessive political issue – you guessed it – climate change, writes Joseph Vazquez in NewsBusters.
- “Trump cancels wind and solar subsidies – Canada’s Net Zero policies are economic suicide” – While Trump focusses on energy security and dismantling the climate empire in the US, Canada still plods a Net Zero path to economic suicide, say the Friends of Science Society on Clintel.
- “The Green lobby’s dishonest crusade for solar and wind” – In RealClearMarkets, Vijay Jayaraj argues that the Green lobby’s push for wind and solar is a “dishonest crusade” built on flawed statistics and fantasy economics.
- “Energy policy vs climate dogma: why the voters aren’t marching to the Green Revolution’s tune” – Americans just aren’t buying the climate apocalypse, says Charles Rotter in WUWT?
- “Pope Leo appeals for more climate action” – The first US pope is just as green as his predecessor, writes Eric Worrall in WUWT?
- “The poisonous face of UN Israel-hatred has finally got her comeuppance” – The Trump administration has sanctioned Francesca Albanese, writes Jake Walllis Simons in the Telegraph; it’s a sign of the West’s sickness she was indulged for so long.
- “Women who claimed Brigitte Macron was born male cleared of defamation” – Two women convicted of defaming French First Lady Brigitte Macron by claiming she was “born a man” have been sensationally cleared on appeal, reports the Mail.
- “A response to the World Health Organization and their SAGO report” – On Substack, Jim Haslam takes aim at the WHO’s dodgy SAGO report, accusing it of whitewashing evidence of a US lab origin for Covid.
- “Why should the hunt for the next Archbishop of Canterbury be ‘inclusive’?” – Just when a change in culture is needed, the same culture has shaped the process for selecting the next Archbishop of Canterbury, writes Fergus Butler-Gallie in the Spectator.
- “I’m just ugly not trans, train driver told colleagues” – Aslef is pushing back against the Supreme Court’s ruling that “woman” means biological female, reports the Telegraph.
- “‘Toilet wars are over. It’s time to flush this nonsense for good” – The SNP Government and public servants, indoctrinated by the taxpayer-funded trans lobby, are still refusing to implement the ruling of the Supreme Court on gender, says Iain Mcwhirter in the Times.
- “BBC bans Gregg Wallace over ‘unsafe’ behaviour” – Gregg Wallace has been banned from working at the BBC after the corporation ruled that he was not safe to have in the workplace, reports the Standard.
- “Terrified of criticising Islam” – Toby appeared on Mike Graham’s TalkTV show yesterday to talk about the Government’s attempt to come up with an official definition of Islamophobia.
- “‘They’re trying to correct a problem that doesn’t exist!’” – On TalkTV, Mike Graham grills lawyer Luke Gittos over the Law Society’s decision to run free training courses for aspiring judges exclusively for BAME solicitors – with white applicants excluded.
If you have any tips for inclusion in the round-up, email us here.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.