
There follows a guest post by a doctor in Australia, who prefers to remain anonymous, about his experience of the pandemic Down Under.
I entered General Practice 34 years ago in rural New South Wales. Needless to say, the changes since then have been immense.
In 1988, most GP’s admitted and cared for patients in hospitals, did regular house calls, delivered babies, performed surgery and practiced anaesthetics. Now, other than in remote rural locations, very few provide any of these services. As many patients inform me, most GPs seem to want to only look at their computers, order tests, prescribe drugs, give immunisations and refer to the specialists.
Twenty years ago, I underwent specialist training in Sports and Exercise Medicine, and now work purely in that area. I remain, however, registered as a General Practitioner. The Australian health system has plenty of similarities with the British system, though has a number of features which differentiate the two. In Australia, the vast majority of GPs work in the private system, working as contractors to health centres, being employed by private practices, running practices themselves, or in a dwindling number of cases working as solo GPs. Very few work as employees of the public sector or NGOs.
Each state has a Health Department, which can impose different regulations on GPs, such as Covid vaccination requirements, and runs the public hospitals in that state; the Federal Government also has a Health Department which oversees the registration of doctors, pharmaceutical benefits scheme and health budgets. Registration is governed by the Australian Health Professional Regulation Agency (AHPRA) via the Medical Boards. The Therapeutic Goods Administration (TGA) controls drug and device availability. There are both Federal and State Chief Medical Officers (CMOs) dictating policy settings. The Australian Medical Association (AMA) is a lobby group representing less than 15% of doctors, but has political sway. Continuing education and training is provided by the Colleges – in the case of General Practice, this is both the Royal Australian College of General Practice (RACGP) and Australian College of Rural and Remote Medicine (ACCRM).
Early on after the advent of the Covid vaccination program, the TGA banned prescription of hydroxychloroquine and ivermectin for Covid infections, partly as they were seen as possible threats to vaccine uptake. Recently, the prescription of hydroxychloroquine for Covid infections again became legal, though only in Queensland.
Payment is essentially fee-for-service and underscored by the Medicare system. This is a Government-owned insurance program paying doctors for their services. A fee is set by Medicare for over 5,000 different ‘services’. Doctors may choose to ‘bulk bill’ the patient, being paid directly by Medicare, or privately bill the patient where the patient receives a rebate covering part of the fee.
An example of a Medicare fee is the one for a standard 15 minute GP consultation. This is currently around $40 (£20), meaning a GP seeing four patients per hour would gross $160 per hour. After practice costs and rent are deducted (all costs are the responsibility of the doctor), the hourly rate for a Bulk Billing doctor may be as low as $60-$70 before tax. This has led to GPs looking for ways to increase their income, and Health Departments devising methods to pay GPs extra for conforming to additional bureaucratic programs.
It is under this complex and ever changing array of rules and regulations that GPs practice. The Covid pandemic has, as with all countries, seen massive changes in the structure of General Practice.
Lockdowns have varied state by state, with Melbourne being the most locked down city in the world, complete with curfews. Other states have been less affected, though rules have changed capriciously.
All states currently require all health workers to be vaccinated against Covid, though in some states this means three jabs and others two. In Victoria, farm workers on remote rural properties cannot drive a tractor without being jabbed, but can go to a pub or restaurant without the requirement.
State borders have imposed rigid boundaries periodically which has affected access of patients to hospitals as well as outpatient services.
Mask mandates have also varied state by state and over time, as well as by situation.
Current medical practice mask rules in N.S.W. appear to be similar to those in the U.K. with no mandates in General Practice clinics, though the RACGP strongly advises their use. My observation suggests that most clinics are still advising the wearing of masks by both practitioners and patients. My clinic has a large number of GPs and specialists (at least 40) and mask wearing is almost uniform. I don’t wear one for the reason that evidence suggests no benefit and possible adverse effects from their use. I advise all patients who enter my consulting room that they may remove their mask if they wish – I could count those who refuse my offer on the fingers of one hand!
Covid vaccination rates in Australia are amongst the highest in the world. The most recent data for N.S.W. suggest 96.3% of those over the age of 15 have had one shot; 94.8% two shots; 63.0% three shots. General Practice with all its governing bodies has been an extremely strong encourager of vaccination. I am aware of some doctors who have refused to see unvaccinated patients. The medical profession, Colleges, AHPRA, the TGA, CMO’s, Health Ministers and the mainstream media have uniformly disparaged those sceptical of the vaccines. Medical practitioners have been deregistered by AHPRA for publicly advising against the vaccine. AHPRA has suggested that doctors have a responsibility to uphold public health directives (lockdowns, masks, vaccine mandates) even if this contradicts the evidence. Failure to do this involves risk of deregistration. Personally, I’ve treated around 100 patients for vaccine side effects, ranging from mild to severe. I’ve reported many of these to the TGA.
With clear evidence that significant risk factors for adverse outcomes in Covid cases are obesity, low Vitamin D levels and diabetes, there has been a conspicuous lack of public health education from GPs, the Colleges, or the CMOs. The message to those infected has always been to go home, rest and go to hospital if you become seriously ill. Nowhere have I seen mention of regular exercise, checking for or treating low Vitamin D, losing weight or reducing alcohol intake. It could be suggested that the public health measures of lockdowns, curfews and school closures may actually worsen these lifestyle risk factors.
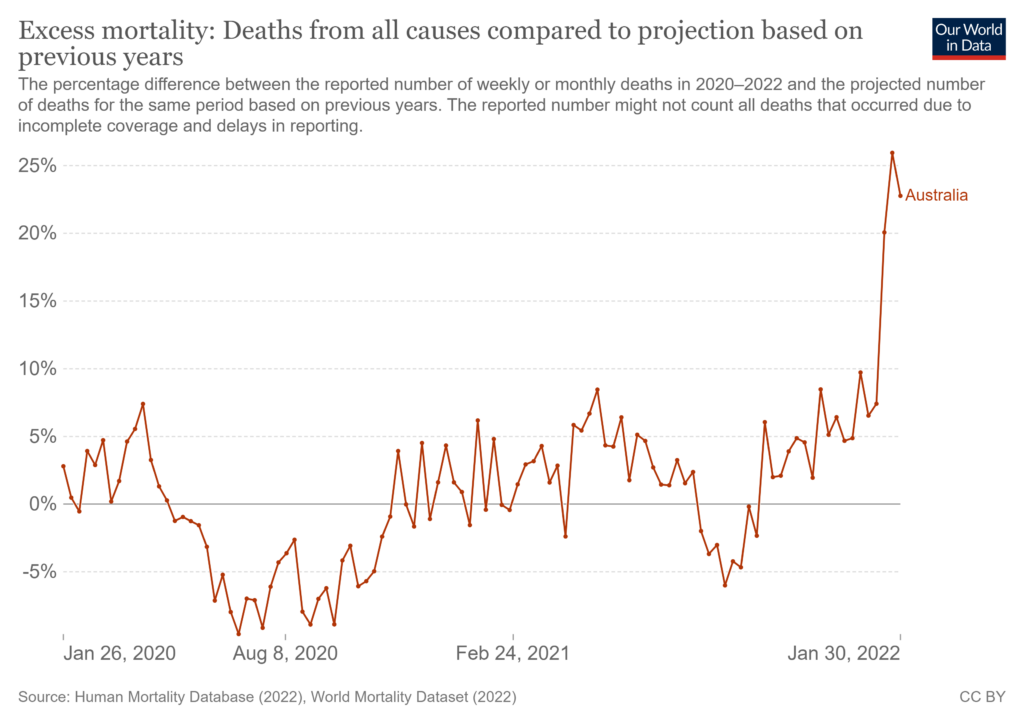
For example, in 2022, there were 15,805 deaths that occurred by January 31st and were registered by March 31st, 2,865 or 22.1% more than the historical average. Of these, there were 486 deaths due to diabetes in January 2022. This is 38.1% higher than the baseline average, and 42.5% more than January 2021 (341). There were also 1,398 deaths from dementia, including Alzheimer disease, in January 2022. This is 29.2% higher than the baseline average and 13.6% higher than in January 2021.
My discussions with GPs suggest that many, or perhaps most, do not often read research papers into masks, lockdowns, vaccine efficacy or side effects, but enthusiastically follow the guidelines. I have found many patients are significantly better informed about the research than their doctors.
Unlike the U.K., there has been minimal opportunity for doctors to work from home or close their doors – this is both a function of the ‘fee-for-service’ basis for paying GPs as well as Medicare being quite restrictive with ‘item numbers’ for Telehealth services. Working from home for GPs means going broke.
In summary, there would appear to be many similarities between the U.K and Australia in General Practice Covid policy approaches. There are differences, however, largely relating to Australia’s division of Health Services between Federal and State, as well as the presence of Medicare in the funding of General Practice. Perhaps the main similarity, disappointingly, is the failure of the major players to engage in an open discussion of the Covid measures – benefits, costs, ‘The Science’, what went wrong and how to improve things when the next pandemic occurs.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Looks like we could be cancelling our holiday booked for Saturday then. Thanks Grant Shapps you twat.
are you vaccinated? presume not… same for me, although wife is. we’re supposed to be off to portugal but that’s shitcanned. oh well, small price to pay for me to keep my principles
I’m not and neither is my wife. She’s wavering because needs to go abroad for work.
I said ‘give it 6 months, either there’ll be a vacc induced catastrophe or theyre fine and I’ll get one too’
covid will have disappeared by then and it will be moot
I feel sorry for people that have to go abroad but for me I’ll just stay here until it all blows over
It will blow over. But what sort of “normality” will remain? Remember, we are ruled much more by convention than by laws written by politicians…
I don’t trust the mRNA vaccs nor does wife. Moved Spain hol to next summer.
Nasty feeling they’re going to force vacc on everyone, or you’ll be excluded from society.
We’d hold out for Valneva if pushed into a corner – it seems more like a traditional flu vacc with inactivated virus. Not heard anything negative on it (yet!)
I’ll just be surprised if any of them work. They’ve tried to get a corona vaccine for 40 years. They’ve tried to get an mRNA vaccine for 20 years.
All failed – the only way they could get them into arms was to skip trials and go for emergency licensing.
Agreed, none will work. But if it absolutely comes down to something or ‘concentration camp’ ( I exagerate for effect), then we too would reluctantly go for the Valneva jab if it ever gets approval. It is the least worst. I sincerely hope it won’t come to that.
Just finished booking flights via to two countries to Tampa that is currently a route that is ‘open’ for nonvaxed and border restrictions.
Fingers crossed it stays that way for a bit.
Not just your principles – how about your life?
Honestly I think the risks are low with the jab but it’s principle for me. I don’t need it, and don’t want it. Simple.
I expect the risks are low but we won’t know for a few years. This is the problem for me. I think its utterly wrong to rush out a vaccine (or any medicine) for the whole world 6 months out of the lab. Even if it turns out ok its still morally wrong because its luck. Next time might not be so lucky
“Even if it turns out ok its still morally wrong because its luck. Next time might not be so lucky“
Yes, having this debate with a doctor friend. He thinks “fingers crossed it looks like there won’t be any huge disaster so it will have been justified”.
It’s as though someone spins the cylinder on a revolver with one bullet in it, puts it to your head and pulls the trigger for a laugh, and you shrug and say hey it’s alright because the chamber was empty.
Exactly!!
So much for the “precautionary principle”, eh?
I disagree with your doctor friend.
None of it has been justified.
My position too. Not particularly worried about the health effects, for myself, but if someone pushes me I push back.
Tell that to the 1400+ people who have died or the 1 million + who have had serious adverse reactions in this country alone. Check out the yellow card reporting system which it is said counts for between 1 and 10% of the true number.
None of us are. I’ve persuaded my husband our health & principles are more important than a holiday.
I’m sure he’d get it, but there’s no point if I won’t. And we both agree the children will never be jabbed.
Integrity.

Is it me or is keeping one’s principles harder than it used to be?
MILLIONS are seriously injured or dead from covid vaccines – EU database
https://www.naturalnews.com/2021-07-15-millions-seriously-injured-dead-covid-vaccines-database.html
Stand in South Hill Park Bracknell every Sunday from 10am meet fellow anti lockdown freedom lovers, keep yourself sane, make new friends and have a laugh.
Join our Stand in the Park – Bracknell – Telegram Group
http://t.me/astandintheparkbracknell
*****************************
if you do go you will have to self isolate for 6 days with early release and pay for 2 additional PCR tests (randox PCR tests £43 each with easyjet) – so holiday is still doable but certainly more inconvenient
I’m fine self isolating but my husband says he can’t (he has work…though I’m sure he’s trying to negotiate his leave right now).
The children I guess don’t have to isolate anyway? They’re 12 & 14
We have discussed and decided husband will do this. Or I might. Inspired by our politicians, I went online looking for a loophole and think we may have found one for him. There are LOTS of them. Lots and lots.
Why not go by private jet, the rules don’t seem to apply, and soon the fuel for private jets will be tax free, whoopee!
I like the way you’re thinking. My husband IS a pilot. We could just steal one maybe.
Well WITH-COVID might soon become the 23rd biggest thing mentioned on death certificates in May!!!
It’s obviously an emergency.
Shapps is typical of the thick headed scum that inhabit our present vile government. A face that needs kicking again and again.
Be careful or you’ll be accused of ‘antisemitism’.
of course – now only the vaxxed wont have to quarantine on return to UK – this is about punishing the unvaxxed – pure an simple
Even if I had been up for a jab, which I am not, I wouldn’t be 2 weeks post second dose most likely.
there is no reason for any country to be promoted from amber to green because amber is already green for the vaxxed
yes precisely. so they will never move stuff to green to punish the unvaxxed
The vaxxed still have to wear the masks throughout (can be pretty rough on long haul), still have to have a test on arrival and before departure. Doesn’t seem like much of a reward to me.
no quarantine on return to UK and 2 less PCR tests (if have early release test) – re masks, on my recent trip to spain I wore my life saving mask under my nose then took it off after take off – no problems from anybody. – but your right – I wouldnt be doing any long haul – but nowhere i usually go will let me in anyway
I did long haul last summer. It was fine. Nobody hassles you if you look asleep so just drink yourself unconscious
I would make a sandwich last three hours.
I made a small bottle of water last five.
It was empty for the last two hours.
No one has to wear a mask, even on a plane exemptions apply. Those who wear a mask do so for ease or because they like it. BA never said a word to me about a mask either journey.
Whatever happened to Freedom Air? Or did I imagine that bit?
https://www.vaxcontrolgroup.com/
Be careful where you leave any personal data, this may be a handy honey trap.
The thought had crossed my mind.
Lockdown Sceptics is a WordPress site. You think your email address is safe from an order to WP from the authorities to reveal your email address to them?
I post under my real name. They are welcome to come for me if that day arrives.
You think I didn’t set up an email address just for here?
Yes, my thoughts also, could be a sure fire way of getting a comprehensive list of the unvaxxed
they already know who is vaxxed, therefore they know everyone else is not
Precisely!
There is absolutely no information who is behind this, I would not hand my details over.
Check their Twitter feed. See what you think.
https://twitter.com/VaxControlGroup
Rooting out moles is a very difficult task. There is no replacement for knowing someone personally. I am trying to get more info.
IMPORTANT to say that I found them through LockdownSceptics.org
It would be great if it is bona fide, but the whole covid fiasco has been such an elaborate deceit on such an unprecedented level that it might well be just a ploy to locate the unvaccinated.
I wouldn’t worry about this site…I’m sure no matter how many opt-out things we’ve signed with the NHS that if the Govt wanted to find out from the NHS who hasn’t been vaccinated (under ’emergency powers’ etc!) they could, very easily!
Yet another MSM article parrotted uncritically
There is no scientific basis for any travel restrictions
Why isn’t LS making that case?
Why are they playing on the government’s terms?
This decision can be explained best by means of a Venn Diagram.
All being done to annoy people so that they cave in and get v@xxed
That is exactly what this is about and always has been.
As most of us predicted, the moral and intellectual midgets like Shapps will not easily give up the power to f. up people’s lives.
I’ve not planned to go abroad – but that’s beside the point.
yep, and its more coercion for the young to get the experimental gene therapy
He’s not the shappest knife in the drawer, is he?
They are fucking with us. Brazenly, arrogantly and openly.
Yes they are and have been ever since this started. it was and is nothing to do with our health and everything to do with controlling us. Watching the antics of the G7 in Cornwall should have bust this scam open wide!
A ninety four year old woman stands cheek by jowl with foreign visitors who have not been quarantined and we’re supposed to ignore what they do and believe what they say.
All part of The Project plan
BIG BLUBBER is MOCKING YOU
What an incompetent twat! Hes perfect cover for the cowardly idiot we have as PM, you know , the bastard who calls our enemies “ our friends” when they slap him down
I wonder when they’re going to make enough people angry that you start hearing more about it. A lot of people will take not going on holiday in stride, but tempting them and snatching it away must make even the most ardent lockdown proponent angry.
True, but to the Lockdown Zealots it will just be a chance to moan about the nasty tories, rather than focus on the elephant in the room.
..
Oh come on. Don’t be unfair. They’re outdoors and sitting down, and everyone knows that forces ALL infectious diseases (not only SARS-CoVID-2) to leave you well alone.
And, of course, there’s no “r” in the month.
Also private jets cleanse the body and VIP lanyards eliminate viral particles.
Is that being thrown out of the one or hanged with the other, with the eternal panacea being Death?
I suspect the change came about because the unvaccinated uber rich (hey, they don’t want some dodgy untested gene therapy that might kill them clogging up their veins do they, mammon forbid) will be casting off on their super yachts to all those newly amber-ed destinations where they’ll party with their fellow plutocrats like its 1939! and without the great unwashed spoiling their view except to pour them another glass of bubbles or to boil them a lobster. Couldn’t be fucking clearer.
It’s a total shambles. Outbound balls-ups, inbound cockups and queues, and every one a nice little earner for some crooks from the Government downwards. We did quite well in 1940, but is it really necessary to have the neglects and disasters of that year, just to be able to engender some sort of “Dunkirk Spirit”?
A sense of menace and near at hand danger that isn’t imminent threat of death is surprisingly popular amongst people inclined to obey officialdom without thinking.
This is now planned and deliberate – this endless uncertainty is designed to break peoples will and stop them from travelling.
I find it incredible that people put up with this crap from this evil government.
So the same mayhem as last summer, before there were jabs.
Governments the world desperately try to keep up the illusion that they are dealing with this made up problem while heaping more and more abuse on their populations.
Boy are the masses dumb as f**k.
It’s far, far worse and restrictive everywhere than last year.
That alone should make even sheep think and complain.
This after the vote by Parliament yesterday to make vaccines mandatory for care home workers …
The Pig Dictator and his lackays in ‘Parliament’ are intent upon officially signing away even the tiny rest of their sovereignty to the WHO in November.
From then on, the UK will officially be ruled from Geneva.
Ah, the new EU! Their revenge will be of the Carthaginian variety then?
Ah, a peasant’s revolt! Bring it on! Just don’t demand a flagon of ale or refuse to remove your hat when you meet the king like Watt Tyler did…
F ING farce.
The Gaurdian is never worth reading in full.
or in part.
Nor is it of any use in the jakes or lighting a stove. Too wet in both instances.
It does however provide a rich supply of pictures of arseholes on whose faces my hens can crap, whilst bedded down for the night in their coop.
Your poor hens.
NarrativePaper is solely for composting.
Some of this really makes you wonder.
It’s quite obvious if you think about it that the travel restrictions make absolutely no difference because they aren’t close enough to 100% to stop any of the variants from coming in. After all, ten people can spread a virus just as easily as one hundred or one thousand. We can’t even have restrictions that are strong enough to stop infected people from coming in because we’re importing food via the Chunnel and the lorry drivers have a fast pass in via testing. Of course, the testing has a significant false negative rate and there are huge numbers of drivers going back and forth.
And, in fact, we have received each and every variant.
Shapps, Johnson, Hancock, etc, all know this because they’re not so unintelligent to fail to see that all of these measures aren’t going to make any difference at all.
So, this means that they are preventing families from seeing each other and people from taking holidays for what they know is no reason at all.
One wonders why the press doesn’t mention this…
They want to stop us travelling altogether. It is part of the Green Agenda and zero carbon policy.
They (the wealthy elite) will be still be zooming about in their private jets and making little forays to the edge of space because they will be off setting their carbon footprint elsewhere, of course.
Spot on Monica. That’s the only possible explanation for this madness. It certainly hasn’t got anything to do with Covid.
Agree, decimating the commercial airline industry was always part of the plan. Another instance of where Covid has been ‘weaponised’ to effect social change.
Theh are unintelligent, the aim is not to stop a spread of some virus. They are simply trying to make travel as difficult as possible. As Monica days below there is a different agenda here.
https://medicalxpress.com/news/2021-07-vaccine-hesitancy-young-adults-hamper.html
Medical Junta PR tries to guilt trip people into joining risky experiment
And ramping up the Long Covid (formerly known as post-viral fatigue) bogeyman!
https://medicalxpress.com/news/2021-07-greta-thunberg-effect-belies-autistic.html
And this is just nonsense on stilts.
Do… uh… do Our Vaccines work less efficaciously depending on which label the Home Office has put on a piece of geography?
Truly, this sentient Virus from Nowhere, and Our Vaccines, are redefining Our Settled Science every day, in every way.
I don’t go abroad on holiday, but this fiasco over the restrictions on travelling have had a knock-on making a holiday in the UK unaffordable, as there’s far more demand. It was bad enough normally during the school holiday season, but now the prices are eye-watering.
That is true.
It has another knock-on effect. Here in the Western Isles, the quotient of car-bound arseholes on single-track roads has rocketed, impairing the quietude. Mad Wee Krankie, Straight-Jacket Sridhar and armchair petrolhead pollution, to boot :-). Is there no escape?
“The Guardian report is worth reading in full.”
Now there’s a sentence you don’t see very often.
And it’s still a lie.
“Julia Hartley-Brewer
To clarify, if Mallorca and other Balearic Islands go back on the amber list from Saturday:
Anyone flying home this Thurs or Fri, no quarantine
Anyone flying home on Sat or Sun, 10 days quarantine
Anyone flying home from Mon, no quarantine
That makes perfect sense, right? ”
Since when did ‘sense’ have anything to do with it?
Does anyone have a template letter for mask exemption for travelling on a plane. The typical lanyard is not enough for easyjet, they want a doctor’s letter which most doctor’s are refusing to give as they say self-certify. Typical government loop of hell. Just want to get on a plane without suffocating and panicking…
I sympathize. But this is one thing GPs are getting right. No easy solution.
Fake one?
This is a load of bs and I’m not saying you should comply, but why don’t you just write the letter yourself from a fictional doctor? Even if they call them then they’re only going to get a receptionist who don’t even seem to be able to give out appointments let alone confirm that you’re a patient or any medical details.
If they phone my GP the won’t even get that. Just a long winded answerphone message wingding about Covid and tellIng them to log onto the practices website (or better still bugger off and not bother them at all – well they did not say that is those exact words but that is the general gist of the message).
Come on people – WAKE UP!!!
ITS OVER!
One rule for them, another for us? Thousands of ministers and officials are escaping self-isolation rules thanks to ‘get out of jail free card’ pilot scheme that means they can take daily tests instead. Cabinet Office is among the bodies signed up to a pilot scheme replacing self-isolation with daily testing .
Thousands of ministers and government officials are escaping self-isolation thanks to a pilot scheme that amounts to a ‘get out of jail free card’, it was revealed today.
The Cabinet Office, Border Force and Transport for London are among the bodies signed up to a trial that replaces quarantine with daily testing – meaning they can continue working after being ‘pinged’ for close contact with a positive case. Michael Gove used the arrangements to avoid self-isolating when he returned from watching the Champions’ League final in Porto in May.
https://www.dailymail.co.uk/news/article-9787883/Ministers-officials-escaping-self-isolation-thanks-pilot-scheme.html
I reckon daily testing is more of a bind than quarantine – which you can ignore.
So some are now fighting to have the same ‘privilege’, Daily Testing, gimme gimme. The Behavioural Scientist wheels keep on turning
Ministers secretly take part in ‘get out of jail free’ Covid trial to avoid self-isolationStaff at three government departments sign up to pilot scheme, enabling them to return to work immediately after being notified by NHS app.
https://www.telegraph.co.uk/politics/2021/07/13/ministers-secretly-take-part-get-jail-free-covid-trial-avoid/
We are becoming more and more soviet like by the day.
If only they would review the emergency legal apparatus they are abusing to keep this farce going with such frequency.
I yearn for the day that these lot get carted off.
More proof if any any were needed not to engage in anyway whatsoever with this regime until it has been removed
Absolutely.
Who is going to remove it and how?
Some say that the jab is part of a global depopulation programme through sterilisation.
I am glad to see an increasing number of government ministers are doing their part in this programme by being total wankers.
Probably not satisfying even for them since most of them lack the cojones.
They do say that but the Chinese have just removed the 1/2 child law
Did Grant Shapps used to have a part as a puppet in Thunderbirds? I truly hope I never have to meet him.
And yet the rich and famous are on beaches all over the world, is this their NWO, Top of their pyramid scheme are the Rich and Famous bottom are the plebs. Island nations which traditionally travel more and by air are targeted first by the Greenies
Went for a walk near Leeds Bradford airport on Sunday. In 1 hour I saw 6 private jets land. They were the only aircraft I saw.
But why are they having these lists at all ifthe “vaccines” work? Or do they intend to permanently reduce the number of those who can holiday abroad (with opposition support)?
The Mirror etc. should be campaigning on this – “politicians’ plan to prevent working class foreign holidays” etc. – shoukldn’t they? (And I remember that story about a local newspaper editor who said “we are as independent as our budget allows”…).
Isn’t “The Science” so scientific!? Shapps, Khant, BoZo, SAGE, etc. need to go back to school ( or jail!).
Hold tight and sit it out. Bust the travel industry until they stand up to this tyrannical government.
Back to ‘jab and fly’ at the airport. How considerate. Bet the ‘boosters’ will be available soon at the local airport.
https://www.google.co.uk/amp/s/www.thelocal.de/20210713/stuttgart-airport-passengers-offered-covid-vaccine-without-appointment/%3famp
Good
The collaborators need to suffer by their own hand they enabled this
Mind Game Playing Power Drunk Fascism
The gormless Mr Shapps really has worked hard at making himself part of the problem. He has encouraged the spending of our money on divisive “low traffic” nonsense. He has fucked up numerous holiday and business travel plans, and he has weighed in on the highly divisive mask wearing “expectation”.
He’s like Sadiq Khan with his brains bashed out.
MILLIONS are seriously injured or dead from covid vaccines – EU database
https://www.naturalnews.com/2021-07-15-millions-seriously-injured-dead-covid-vaccines-database.html
Stand in South Hill Park Bracknell every Sunday from 10am meet fellow anti lockdown freedom lovers, keep yourself sane, make new friends and have a laugh.
Join our Stand in the Park – Bracknell – Telegram Group
http://t.me/astandintheparkbracknell