
An unresolved puzzle of the pandemic is why COVID-19 death rates have been so low in East Asia. We know this can’t be due to different ways of counting COVID-19 deaths because it shows up in comparisons of excess mortality.
The most recent published estimates of excess mortality, taken from a paper in eLife by Ariel Karlinsky and Dmitry Kobak, are shown below. In this analysis, excess deaths since the start of the pandemic are given as a percentage of annual baseline mortality (see grey numbers).
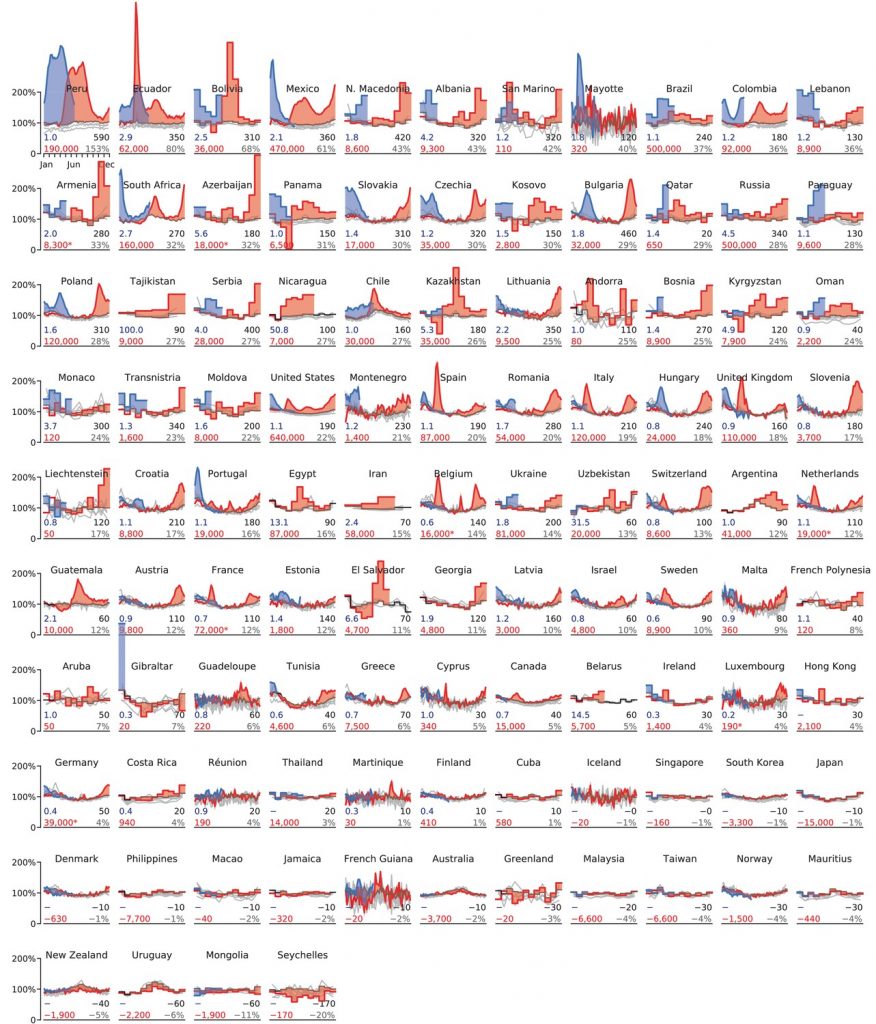
Excess mortality in Europe ranges from –4% in Norway to 43% in North Macedonia, and most countries are in the 10–30% range. In East Asia, by contrast, excess mortality ranges from –11% in Mongolia to 4% in Hong Kong. (Note: excess deaths in East Asia may have increased slightly in more recent months.)
As I’ve argued before, it’s unlikely this difference is due to lockdowns as Japan has seen negative excess mortality despite having some of the least restrictive policies in the world. In 2020, for example, there were zero days of mandatory business closures and zero days of mandatory stay-at-home orders.
So what can explain East Asia’s low COVID death rates? One factor that’s often mentioned on social media is their low rates of obesity. As I’ll explain, however, this can’t explain more than a small part of the difference between East Asia and the rest of the world.
To begin with, obesity’s effect on the risk of death from COVID-19 – conditional upon on infection – is actually quite modest. (By comparison, the effect of age is enormous.)
While it’s often said that most COVID-19 patients in the U.S. are overweight or obese, this is isn’t very surprising. After all, most U.S. adults are overweight or obese. For example, a CDC study published in March found that 50.8% of COVID-19 patients were obese. Yet the figure for adults as a whole is only slightly lower, at 42.4%.
Earlier this year, the BBC radio program More or Less (which deals with statistics in the news) calculated that if the global obesity rate dropped to zero, the total number of COVID-19 deaths would fall by only 7%.
If you look at the chart above, there is no obvious clustering of highly obese countries on the first two rows. For example, the obesity rate in Peru – which has seen excess mortality of 153% – is less than one in five.
What’s more, two recent studies estimated that there have been around 4 million excess deaths in India. This equates to excess mortality of around 40%, which would place India on the top row of the chart above. Yet the country has an obesity rate of only 3.9% – one of the lowest in the world.
All this suggests that something other than lack of obesity explains the low COVID-19 death rates in East Asia.
Stop Press: For an alternative view on the relationship between obesity and COVID mortality, see this post on Swiss Policy Research.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Fat people get more Covid.
Ban fat people!
Old people get iller from Covid and take up hospital beds.
Ban old people!
Black people are less likely to obey the Gauleiters.
Ban black people!
Outrageous?
Yes. So ban the unvaxxed, the one minority it’s ok to persecute.
“Yes. So ban the unvaxxed, the one minority it’s ok to persecute.2
Massive Worldwide BACKLASH Against Forced Vaccinations!!!
https://www.youtube.com/watch?v=prPUvKSGKC0
This why we need to get join in with Worldwide BACKLASH as much as possible before it’s too late
Next events:
5.30pm Tuesday 31st August
Roundabout (County Lane/Jigs Lane N)
Outside Tesco Superstore
17 County Ln,
Warfield,
Bracknell RG42 3JP
5.30pm Friday 3rd September
Loddon Bridge, (Winnersh Garden Centre/Showcase Cinema)
Reading Rd, Winnersh,
Wokingham RG41 5HG
Stand in the Park – Bracknell – Telegram Group
http://t.me/astandintheparkbracknell
India death rate with covid 314 per million, UK 1940; I am confused by this article, this is an example of why.
Its what you eat more than how much. Plus they had SARS1 and don’t use the same ACE-inhibitors as the west. This was known in march 2020, this article adds nothing.
COVID does seem to be a lipid in the lungs disorder (still not certain it’s viral caused or auto-immune over-reaction), so it’s reasonable to assume the probability those with disordered lipids (probably from chronic dietary fructose) will be worse hit.
Lipid pneumonia, caused by the ‘wrong’ sort of fat getting in the lungs. Its what you eat.
The symptoms are identical to later stage ‘covid’. Who the hell can the difference! Maybe a viral infection, actually any reasonably agressive viral infection can set this off in old people and people with high ‘bad’ cholesterol.
So you go looking for a particular virus with a defective PCR test and hey presto you define pnuemonia deaths as ‘covid’.
Why are we still having this conversation, its been known since March 2020?
Exactly we’re basically testing for “dihydrogen monoxide”.
Looking at the graphs does seem to lead one to the conclusion… There doesn’t seem to be any correlations with anything.
They used ivermectin in India. State Uttar Pradesh in India – 47 deaths per million(pop. 230 million, 828 persons per km², UK 287 per km²) – early ivermectin treatment
There are several possibilities. The usual one is that Asians where masks more often. Okay, except mask wearing differences in Europe/North America show between a 0-10% reduction in infections, and cannot be the cause of these differences.
the two more likely causes are: higher interactions with Covid-related viruses over past two decades or that the ethnic genome of Asians has enough differences (and we see this in a number of diseases) that the risk of death is just lower by nature. It might be higher for the next virus that begins in the Americas or Africa. This may explain why the Chinese vaccines, tested only on Chinese genome trial participants, was so ineffective the further away from that population you went (South America and South Africa seeing the highest fail rates from it). Diseases are difficult, and viruses are evolutionary developed and the want to transmit. Killing hosts is not in their evolutionary interest. Viruses developing in Asia would be more likely to be less deadly for those nearer so that they can spread further. We may find out in the next decade. Or…the scientist and politicians will credit lockdowns and masks and move on quickly before we learn their errors.
“the two more likely causes are: higher interactions with Covid-related viruses over past two decades or that the ethnic genome of Asians has enough differences (and we see this in a number of diseases) that the risk of death is just lower by nature. “
almost certainly this is what it is
just to add – sars cov 1 seemed to rise in Asia and disappear – maybe a low consequence variant arose and vaccinated everyone in that area and that makes them less prone to sars cov 2
Can we please please please stop with this myth of mask wearing Asians.
IT IS COMPLETE AND UTTER BULLSHIT
i have lived most of my adult life in Asia, have travelled frequently all over, and the only place one would see masks occasionally was in large Chinese cities when the pollution was horrendous. And even then it was a TINY number of people.
Asians. Never. Wore. Masks.
Stop propagating this very inaccurate and very harmful myth.
Indeed – I worked in China for a while and no one wore masks.
Well said!
I see it as an attempt to normalize the practice.
The authorities saying: “Oh, but in Asia people always wear masks”
lying, not saying.
Sorry, I agree but I felt it necessary to address what all the media would inevitably credit this to. I’ve never lived in Asia but my fiends here in Oxford from Asia tell me that their families have never worn masks, and these are people from across the Pacific Rim. But you know that masks (and NPIs) always get the credit.
Japanese?
I disagree with you there.
I live in Thailand and it has always been common to see people wearing masks to provide some protection against the air pollution.
We don’t have any MOT’s on the vehicles here and the amount of smoke they produce is phenominal.
where do you get this shit from? They show nothing of the sort as a piece of cotton is not going to stop a virus. There’s been countless studies and they don’t even show a difference at stopping larger bacteria in a surgical setting.
Probably thinking of the Danmask study which did show a 10% reduction in those who wore masks diligently over non mask wearers. Not statistically significant, so not to be taken very seriously (the slacker mask wearers did even better) and there could have been behavioural confounders because the study was, obviously, not blinded to participants or the people around them.
I’m just repeating the studies. I don’t believe they do a darned thing either. But even the most pro-mask study can only project a 10% reduction in infections, and those among the most mobile, aka the least likely to get sick.
I lived for a time in the mountains of America and saw how snow passes right through chain link fences. I’ve used a screenshot of that to explain to people how pourous barriers can’t stop far tinier objects. Sure some sticks to the fence, but the pic I use show a snowball behind.
I’m anti mask to the max and even exempted my kid last March when they went back. But even the most pro-mask person can’t give any evidence for more than a trifle (10%) difference, and yes, those studies are flawed.
Even the paper’s authors didn’t try to claim there was anything to infer in 48 vs 53 infections other than random noise. One only needs to look at last year’s data before/after mandates to see there’s no signal there.
Or the Chinese faked their studies, of course, and lied about their figures in China.
Oh no, impossible….
A different age profile? A more racially homogeneous population with more people living in the climate and terrain for which their bodies have evolved? (no doubt that would be considered a ‘racist’ statement, but the evolution of physical characteristics to deal with the challenges of climate and terrain is what ‘race’ is). Inherent immunity to closely related viruses? Fitter bodies from walking, cycling and agricultural work? A diet with less sugar and dairy produce? (nearly half the Chinese are lactose intolerant).
What it isn’t is the masks that they wear in cities against pollution!
It is precisely the lack of lockdowns and associated measures – such as the removal of vulnerable people from hospital – which explain the lower mortality in East Asia.
Lockdowns -and associated measures – do this by perturbibg the normal social and economic functioning.
Japan, South Korea and Taiwan had no or few lockdowns until recently. There was a distinct lack of panic.
Lockdowns in China were for an average of about two weeks per city and were very different from the West with officials organizing food deliveries for residents for example.
All across the world (see Peru) excess mortality is correlated with the severity of lockdowns and associated measures.
“Experience has shown that communities faced with epidemics or other adverse events respond best and with the least anxiety when the normal social functioning of the community is least disrupted. Strong political and public health leadership to provide reassurance and to ensure that needed medical care services are provided are critical elements. If either is seen to be less than optimal, a manageable epidemic could move toward catastrophe.”
Dr. Donald Henderson (who led the effort to eradicate smallpox)
See also the work of Dr Denis Rancourt in this area:
https://denisrancourt.ca/entries.php?id=9&name=2020_06_02_all_cause_mortality_during_covid_19_no_plague_and_a_likely_signature_of_mass_homicide_by_government_response
https://denisrancourt.ca/entries.php?id=104&name=2021_08_06_analysis_of_all_cause_mortality_by_week_in_canada_2010_2021_by_province_age_and_sex_there_was_no_covid_19_pandemic_and_there_is_strong_evidence_of_response_caused_deaths_in_the_most_elderly_and_in_young_males
Terrific comment and links. Thank you.
Some interesting Denis Rancourt interviews mainly talking about C19 death distribution, how deaths were concentrated in certain areas and hospitals, not following the typical path of a pandemic, suggestive of foul play on the wards and in the care homes
Interview With Canadian physicist and interdisciplinary scientist, Denis Rancourt
https://www.bitchute.com/video/aS6mVyGt0xEq/
Prof Denis Rancourt : Doctors for Covid Ethics Symposium – Day 1
https://www.bitchute.com/video/gbbG9pgWInee/
It’s likely to be genetic. It is known for instance that East Asian people are more susceptible to influenza than Caucasian people, this is due to a genetic predisposition. Maybe their immune systems are more able to target corona viruses.
No, because otherwise a lower mortality would be noticed amongst East Asians in the West.
it would be interesting to split into
1 – east asians that have been in the west for decades
2 – east asians in the west but who were in the east for sars cov 1
You assume no gaining of immunity from past infections when younger that provide protection against viruses they are genomically weaker to. History plus genetics are important.
Interesting article.
Apart from possible genetic reasons, nutrition: seaweed and fish oils perhaps giving high zinc levels and strong immunity.
Higher levels in India despite less obesity maybe due to poor nutrient status of large numbers of people.
Possibility of some crossover immunity built up by local waves of prior infections of similar pathogen.
Possibility that obesity plus lack of activity (but not active people who are also obese) could explain it?
Possibly….
Possibly….
Possibly…
So basically, not interesting at all because it’s speculation based on…. nothing.
The underlying fact is simply that obesity diminishes well-being. Doh!
………eeeeerrrrr – previously acquired herd immunity?
Everywhere SARS got to has hugely low SARS-COV-2 mortality………(until they started jabbing at least).
………eeeeerrrrr – previously acquired herd immunity?
Everywhere SARS got to has hugely low SARS-COV-2 mortality………(until they started jabbing at least).
Mortality
Macau = 0
Samoa = 0
Laos = 14
New Zealand = 26
Singapore = 55
HK = 212
Fiji = 489
Taiwan = 835
Australia = 1,006
Cambodia = 1,903
S. Korea = 2,285
Thailand = 11,589
Japan = 15,994
Malaysia = 16,382
Philippines = 33,448 (figures are sketchy – but lockdown poverty has certainly killed more).
I love the way COVID statistics get thrown around as if they meant something.
Firstly. the underlying data is garbage. No one has a clue how many of the actual deaths counted in the COVID death basket are from the SarsCOV2 virus.
Apart from already well documented misattribution of deaths to COVID, SarsCOV2 is the only virus that is systematically tested for. I wonder how many other potentially deadly respiratory disease viruses like influenza would be found in the dying if they tested for them as obsessively as they do for this new one.
Secondly, there are so many factors which may or may not have contributed to people’s health over the last 18 months that trying to draw general conclusions is literally nothing more than guess work. There are simply too many variables.
Lastly, we just don’t know whether the vaccines make things better or worse. We all know what is being claimed, but only today Bloomberg is pointing out that our health overlords are at a complete loss regarding the efficacy of the vaccines and goes as far as to question whether they could result in more rather than less severe disease.
Searching for answers to why people die of coronavirus is a distraction from (a) the reality that it’s not particularly deadly regardless of how often and how rabidly is claimed otherwise (b) everything governments have done has made matter worse, not better (c) thanks to the persistent denial of those two realities our rights and freedoms continue to be trampled on mercilessly.
“I love the way COVID statistics get thrown around as if they meant something.”
This !!!
Excellent comment, totally agree.
+1 Absolutely agree.
If an amateur chump like me can work out that previously acquired immunity is the key – or at least merits investigation – then how come all those ‘professional’ public health officials can’t?
Is it because they are;
a) utterly ignorant charlatans?
b) so managerially incompetent that the simplest solution just doesn’t occur?
c) egotistically committed to proving their ‘scientific point’?
d) playing out a political strategy to socialise society and the economy permanently?
e) fundamentally corrupt – in the pay of Gates and Big Pharma?
f) just wicked?
g) all of the above?
I vote for “g) all of the above”.
Chasing single variables (with innumerable confounding possibilities) like this is a massively pointless exercise – especially given that the base data is entirely raddled.
… apart from, in this case, feeding the current fad for health fascism.
P.S. I note that Noah’s scepticism, and recognition of the unreliability of data and the nature of confounding variables suddenly comes into play when contemplating a study of the efficacy of Ivermectin in Africa (see Roundup).
by now analysis like this is totally pointless. It diverts resources and attention from what’s really going on. Of course lack of obesity makes a differencebut it has nothing to do with COVID. It’s called being healthy and that generally makes one better capable of handling diseases/viruses.
Please check that East Asians subscribe to traditional herbal medicine antiviral herbs and early treatment protocols. The key to winning with COVID is a strong and organized early treatment response.
Excess mortality data is open to manipulation too isn’t it? I mean if more/less people are actually dying than the data says, how would we even know?
The term ‘excess’ mortality is essentially a con. It presupposes a ‘correct’ level of mortality – which is actually a modelling variable based on the past. And we know about modelling, don’t we?
The jab that didn’t bark in the night.
There seems to be no sign that jabbing, lockdowns or mask scare-sharing did ANYTHING at all in this data either.
Might as well call it a set of red and blue herring graphs.
Maybe there IS no correlation between sars2 and death rates.
Can bullshitting predict the size of the bubble in academia?
https://medicalxpress.com/news/2021-08-high-vaccination-powerful-college-campus.html
“the model showed that if 90% coverage can be attained with a vaccine that is 85% protective against infection and 25% protective against asymptomatic transmission”
there’s your problem. the vaccine doesn’t reduce transmission but increases asymptomatic transmission (by suppressing symptoms)
Actually, it’s probably not ‘asymptomatic’ transmission, but transmission by the mildly symptomatic.
Yes. I know of a case of transmission by a secondary age pupil to parents, where the only symptom was loss of taste and smell.
They masked inside rigorously, but it didn’t stop transmission of course.
OK so that’s what the model suggests. Meanwhile on a real campus:
Duke University: 98% full vaccinated, masks mandated indoors, weekly testing required. Yet, 364 people tested positive this week (all but 8, fully vax).
Response? Mask Harder! Masks are now required outdoors & classes are going online for two weeks.
https://www.newsobserver.com/news/local/education/article253851373.html
from @Humble_Analysis on Twitter
Fully vaccinated?
Surely, they’ve only had two doses ?
odd story
https://www.bbc.co.uk/news/uk-wales-58386905
17 year old has jab, contracts covid and has clot on lung. apparently CT scans show the clot was from covid and not the jab. not sure how a CT scan will show that. has it got a little flag on it?
Quote from the article:
That would be logical given the timing then ..
How reliable are pcr tests immediately or soon after jabbing? Surely they may pick up spike fragments?
Surely Gates/Wellcome has funded a study on this important point?
Oh, sorry – I forgot.
“Former member of the Welsh Youth Parliament,”
Is the most informational thing in the “article” for me, youth political types will tell any lie. Very untrustworthy IME.
How abour early treatment with antivirals? https://exoscientist.blogspot.com/2021/04/asian-countries-routinely-give-anti.html
Covid is a respiratory disease.
Peru has the highest average elevation of any country.
Air is thinner, contains less oxygen at altitude.
Could this be a partial explanation for Peru’s higher death rate?
Nasal irrigation? https://bestlifeonline.com/nasal-irrigation-covid-19/
‘Baxter also adds that the total deaths in Southeast Asian countries like Thailand, Laos, and Vietnam are particularly low. “Yes, they wear masks, and yes, they bow and don’t shake hands, but the biggest difference between them and places like South Korea or Japan is that nasal irrigation is practiced by 80 percent of people,” she says.’
Thailand 166 deaths/million
Vietnam 112
Laos 2
Japan 127
S. Korea 45
If anyone can find a ‘difference’ then they are delusional.
Another bloody irrelevant story.
This is nothing to do with a virus.
Ivor Cummins has covered this in
detail a long while back and sourced new studies to back up – and as commented by a few already – 1. Much higher T cell memory due to many more corona viruses over many years 2. Diet tends to be much more vitamin D rich especially in Japan 3. Different attitude to old people – not so many care homes but cared for at home – and therefore much healthier older population (diet) and yes not anywhere near as much obesity. Another point well missed here is that Australia and NZ are Oceania /Asia region and also experience many corona viruses – and are likely to have high T cell immunity – the crazy dickheads who run the place seem to have forgotten where they are in the world. Anyway all flus and many viruses hit sick and fat people for obvious reasons – the politics is the thing not a relatively benign virus
It’s almost as though all these numbers aren’t making sense. ‘Vaccine’, ‘Vaccinated’, ‘Vaccination’ NO. NO. NO. – anyone who tries to jab me, my family and my loved ones with that *monkey gunk* will learn the ultimate lesson. This is the hill I die on: FIGHT. BACK. BETTER. – Updated information, resources and useful links: https://www.LCAHub.org/
Obesity is a negative health condition.