
Public Health England (PHE) has released a new technical briefing on the variants of concern, number 21, and this allows us to update our estimate of (unadjusted) vaccine effectiveness against the Delta variant using the data it provides on confirmed Delta cases.
We subtract the figures in briefing 21 from those in briefing 17 to give the figures for the period June 22nd to August 15th. We also use figures for proportions of the population vaccinated by age derived from the PHE Covid surveillance reports.
Starting with the over-50s, for the period June 22nd to August 15th, PHE reports 29,282 Delta infections in the double vaccinated and 3,915 in the unvaccinated. PHE figures show that in this period the proportion of the over-50s double vaccinated was stable at 88% and the proportion unvaccinated was 10%. Calculating the vaccine effectiveness against Delta infection in the over-50s (1-(29,282/88%)/(3,915/10%)) gives a figure of just 15%, down from 17% using data from the briefing two weeks ago. This is very different to the estimate in the recent Oxford University study using ONS survey data, a study which I criticised for numerous implausible findings.
With regard to deaths with Covid (within 28 days of a positive test), PHE reports 602 in the double vaccinated and 280 in the unvaccinated in the over-50s in this period. This works out (1-(602/88%)/(280/10%)) at a vaccine effectiveness against death of 76%, down slightly from 77% using data from the previous briefing. This is a 76% reduction in mortality including any reduced risk of infection, not in addition to it. It’s an encouraging figure, albeit lower than earlier studies have suggested.
For the under-50s, for the period June 22nd to August 15th, PHE reports 36,855 Delta infections in the double vaccinated and 125,394 in the unvaccinated. PHE figures show that on June 20th 61% of under-50s were unvaccinated while 18% were double vaccinated. On August 15th those figures were 52% unvaccinated and 35% double vaccinated. Taking the average of these gives 56% unvaccinated and 26% double vaccinated for the period. Using this to calculate the vaccine effectiveness against Delta infection in the under-50s (1-(36,855/26%)/(125,394/56%)) gives a figure of 37%. This is higher than in the over-50s, but still very low and much lower than earlier studies (including the trial) indicated.
For deaths, PHE reports 27 in the double vaccinated and 66 in the unvaccinated in the under-50s in this period. This works out (1-(27/26%)/(66/56%)) at a vaccine effectiveness against death of just 12%. Why this would be so much lower than in the over-50s is unclear, but it’s worth bearing in mind that these are small numbers of deaths which may make the estimate unreliable.
These figures are much lower than those commonly quoted and used in modelling, and if they are closer to the truth then they mean the official, self-congratulatory estimates of “100,000 deaths” and “24.4 million infections” prevented by the vaccines are huge overestimates.
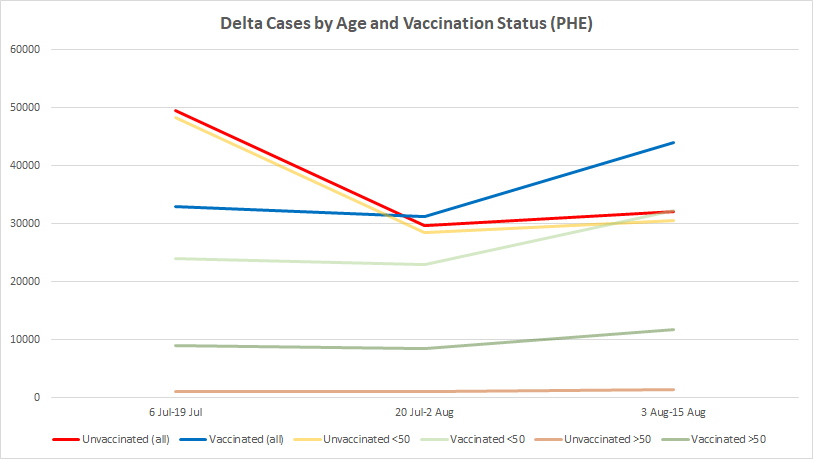
By plotting the differences between the reported total Delta cases in the last three briefings we can also get a picture of how they are changing over time in the different age and vaccine-status cohorts. The red and yellow lines in the chart below show that new Delta infections in the unvaccinated have stayed largely flat over the past fortnight, but those in the vaccinated (for this purpose, all who are at least 21 days after their first dose) have surged, so that a majority of new infections (44,038 out of 76,117, or 58%) are now in the vaccinated. This reveals that the recent modest increase in positive cases in England is being driven primarily by infections in the vaccinated. The fainter lines show the trends in the over- and under-50s, indicating that in both age cohorts new Delta infections in the vaccinated now outnumber those in the unvaccinated. This helps to explain the declining vaccine effectiveness estimates given above.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
I wish Lord Sumption and colleagues well in their endeavours but as I am not a National Trust member I cannot assist. Why am I not a member – for the very reasons Sumption is fighting against? And of course because I am not in favour of giving money to charities.
Donations to charities are just secondary taxation for the gullible.
Donation to Charity, yes.
True charity, true help your neighbour stuff? Rare. Rare indeed.
I agree, though in this case you do get to visit their buildings and grounds, so it’s not wholly a gift.
I’ve been thinking of joining because I like visiting those kinds of places, though have been put off by the wokeness. Perhaps I should join so I can vote. An expensive vote!
I have tons of respect for Sumption. To stand against his world, true strength.
But he needs to be educated about mRNA.
And also MRNA, the ticker symbol for MODERNA.
He has an uphill struggle. As I understand it they have amended voting to “make it easy for members” where they are recommending a committee (themselves) and to “make it easy for the members,” the voting system rigged so a single box with their committee recommendation can be ticked by all those members who haven’t been following things closely and don’t know the resumé’s and policies of the individual candidates. So that’s all the more reason for right minded members to take action and back Sumption.
Yep, already voted following an article I read in the Telegraph. It is _very_ easy to accidentally use the Quick Vote button and not vote for the candidates of your choice but as long as you are alert it is OK.
They have set it up so there is a single box to vote for the “recommended” candidates. Both myself and my wife have voted for Jonathan Sumption, Philip Gibbs, Andrew Gimson, Violet Manners and Philip Merricks. Best of luck to them all.
I am no longer a National Trust member …. because of the woke takeover – and I’m not inclined to pay £70 (or whatever it now is) in order to vote.
There are plenty of private gardens/houses in the west country to visit, if I’m so inclined. And I’d rather give them my money than an arrogant, woke Quango.
Is Lord Sumption awake to the Climate Change “Hoax” yet. Not a good reason not to support him here and I wish him all the best but, with all the literature and authoritative books around on the subject cannot find any excuse for him.
Have cast my vote for those members’ resolutions.
Yikes, save the National trust???? How about saving humanity? There will be no national trust without people Jonathan.
Saving the National Trust is one small step in the journey to saving humanity.
National Trust has long become Just a Property company
I spent a good hour last night going through all the candidates statements and, aside from those mentioned above and couple of others, I found myself repeatedly asking ‘Are you for real?’ I hope most are just saying what they think will get them elected, but fear that many may actually believe the woke / Net Zero / EDI mantras they’re spouting.