
Christopher Snowdon is plainly an anti-vaxxer, however well he tries to hide it. “Existing Covid vaccines are simply not good enough at preventing transmission and infection,” he writes. Hasn’t he read the trial results, showing 95% efficacy against infection for the Pfizer vaccine and 74% for the AstraZeneca vaccine? Or the large population study from Israel showing Pfizer’s 92% efficacy? Or the study from Public Health England showing 67% and 88% vaccine efficacy against the Delta variant for AstraZeneca and Pfizer vaccines respectively?
On what does he base his bald assertion that they are “not good enough at preventing transmission and infection”? Clearly not the science. He doesn’t appear to feel it necessary to give a single scientific reference for a claim that flies in the face of all these respectable studies, leaving the baffled reader assuming he must have picked it up in some article he read on an obscure website somewhere, presumably by a pseudo-scientific sceptic in denial.
This, of course, is not the way to go about intelligently criticising someone’s viewpoint. Which is precisely my point. As it happens, I agree with Christopher that the current vaccines are not very good at preventing infection or transmission, particularly now the Delta variant is in town. But I’m also aware that that is not the current mainstream scientific position (though it is based on recent official data and reports). Rather, it is currently a claim being circulated among the very networks that Christopher pillories in his recent piece in Quillette, naming and shaming the “coronavirus cranks”.
It seems, then, that Christopher is not averse to a spot of ‘crankery’ himself. But how helpful really is all this name-calling, mudslinging and smear by association? Science does not advance by consensus, by everyone agreeing, or by closing down dissenters. Christopher himself is evidently sceptical of one of the key mainstream vaccine claims – that they are highly effective against infection and transmission – so inadvertently places himself within the ambit of his own polemic. Indeed, at one point he fires a shot at the ‘smileys’, as he calls sceptics, for being sceptical of the vaccines, arguing the jabs “have been tested in clinical trials and have demonstrated their safety and effectiveness beyond reasonable doubt in recent months”. Yet he himself goes on to doubt their effectiveness!
The science of Covid is far from settled. Snowdon takes aim at some of the more colourful and dubious characters in the sceptic camp (criticising some claims I have no wish to defend, though he is hardly kind or charitable as he does so). But he notably leaves out of his cranky panorama some of the world’s most eminent scientists who take a sceptical line on a number of the issues he raises.
Sunetra Gupta, for instance, Professor of Theoretical Epidemiology at Oxford University; Martin Kulldorff, Professor of Medicine at Harvard University; Jay Bhattacharya, Professor of Medicine at Stanford University. These three authored the Great Barrington Declaration in October 2020 and have been active in calling attention to the massive collateral damage from lockdowns, especially among the disadvantaged and in the developing world, and proposing alternatives to such extreme and unprecedented disease control measures. Yet they do not receive even a passing mention in Christopher’s very partial rogues’ gallery of sceptics.
Or where is Professor Carl Heneghan, Director of the University of Oxford’s Centre for Evidence-Based Medicine; or Sucharit Bhakdi, former Chair of Medical Microbiology at the University of Mainz; or John Ioannidis, Professor of Medicine, Health Research and Policy at Stanford University? Or many of the other scientists and medics across the world who have publicly spoken out and published research questioning some of the claims being put out from official sources about the pandemic. These are not charlatans, they are not cranks, and they are not obscure individuals who speak with no understanding or authority. They may not always be right, but neither do they deserve to be attacked and smeared by journalists for setting out alternative scientific ways of looking at the data.
The heart of the sceptical position on lockdowns, shared by all these scientists, is that they are not worth it. This claim has a number of aspects, and not all sceptics sign up to all of them, though all the claims have some evidence to back them up. They are:
- The virus is not deadly enough to warrant the measures taken against it;
- The measures are not very effective at controlling the spread, or at least, not enough to justify the harms and costs;
- More focused measures would be sufficient, or at least, more justifiable in terms of harms and costs.
Other claims connected to these include questions about how well official definitions of cases, hospital admissions and deaths match up with actual clinical cases of the disease, the real extent of prior immunity, and the mode of transmission of the virus.
The vaccines are a largely separate matter, and not all lockdown sceptics are vaccine sceptics and vice-versa. The issues around the vaccines concern their novel genetic technology, the extreme speed at which they have been developed and approved under emergency authorisation, their questionable safety profile (with very high numbers of adverse events including fatalities being reported and serious side-effects being intermittently added to the warning label), and their real-world effectiveness.
It really shouldn’t need pointing out to liberal-minded people that all these questions are legitimate areas of scientific research and debate, and we should not assume that we already know the correct answer on each of them that would justify ‘fact-checking’, attacking and silencing all the rest. Indeed, Christopher himself questions the official narrative on vaccine efficacy, despite condemning sceptics for the same crime.
Christopher makes a number of specific claims in his piece that he seems to think are scientifically incontestable but in fact stand on very wobbly ground when given closer attention.
For instance, he asserts that the second wave in the U.K “lasted longer and killed more people”.
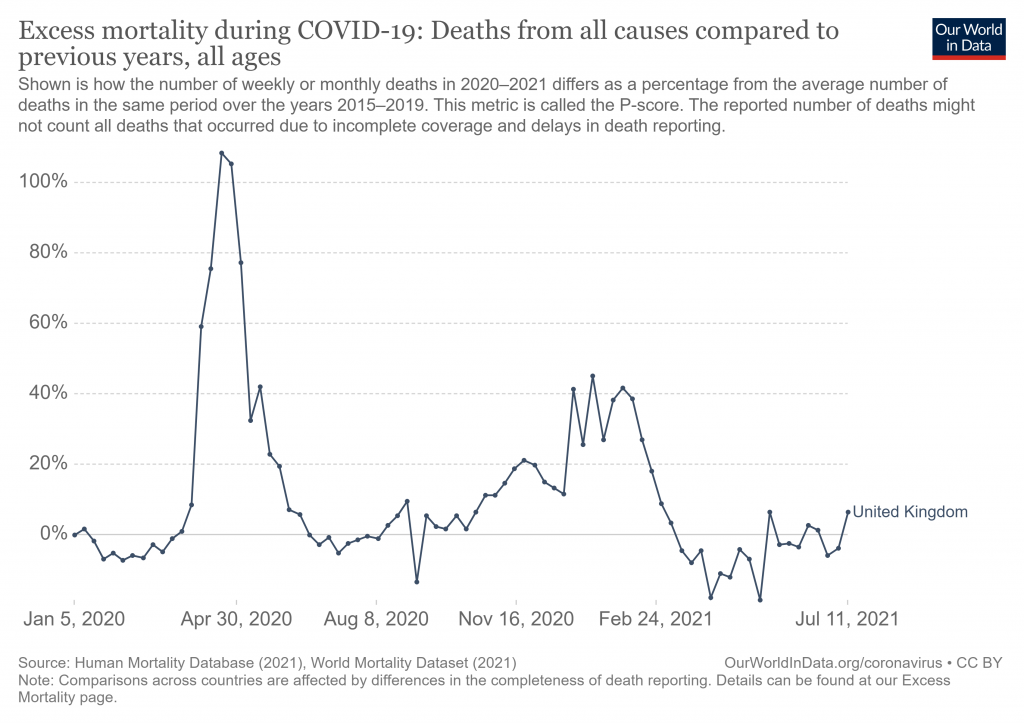
There were more Covid-related deaths between December 2020 and February 2021 than there had been in the first 11 months of the pandemic. At its peak, there were nearly twice as many people in hospital with the virus than there had been in March 2020. In Britain, as in most European countries, excess mortality went through the roof.
The data, however, tells a more complex story. Looking at the weekly total deaths, it’s clear that the second peak is much lower than the first (see below). The higher Covid mortality in winter compared to spring can be seen (blue bars) to be due to more of the non-excess deaths in winter being classed as Covid, whereas in spring there were many excess deaths beyond those defined as Covid (green bars). This discrepancy will likely have a number of factors behind it, but you have to think that how many people were being tested and treated as a Covid case has to play a large part, given that a Covid death is defined as a death from any cause within 28 days of a positive Covid test.
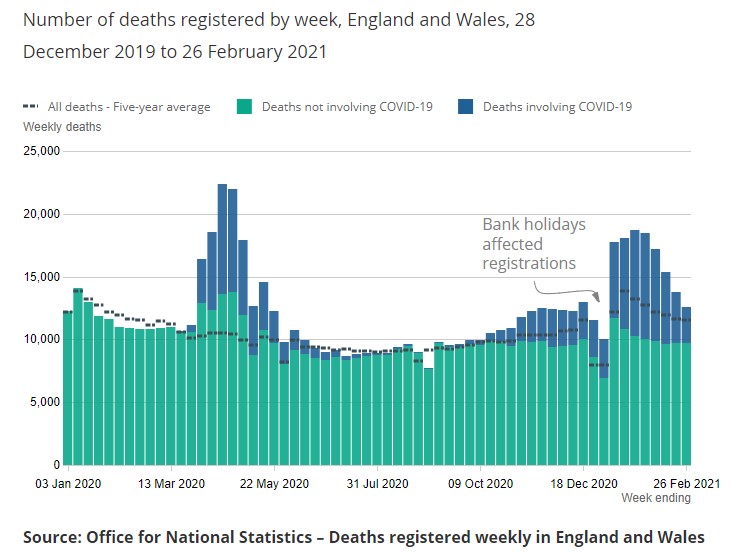
Note also that because it was winter the baseline was higher, meaning in percentage terms the excess peak was less than half the spring peak. This helps to put the winter epidemic into perspective.
The below average deaths since the end of winter have also meant that 2021 is now a below-average year for age-adjusted mortality (so far), the low mortality of the spring and summer having already cancelled out the high mortality of January and February.
Christopher is very critical of sceptics for questioning the reliability of the PCR test and the definitions of Covid case and death based on it. But this was a very live topic in autumn 2020, with a number of top scientists including Professor Carl Heneghan wading into the fray, as this correspondence in the BMJ records. The Lancet published a piece from NHS scientists in December stating that the operational false positive rate of PCR testing was estimated to be “somewhere between 0·8% and 4·0%”. Christopher argues: “The UK had a positivity rate of just 0.2% as recently as two months ago [May]. The false positive rate cannot possibly be higher than the positivity rate, but this simple logic continues to elude the Covid-sceptical community.” This simple logic is too simple, however, as it doesn’t grapple with the fact that the operational false positive rate can vary, including with the volume of tests.
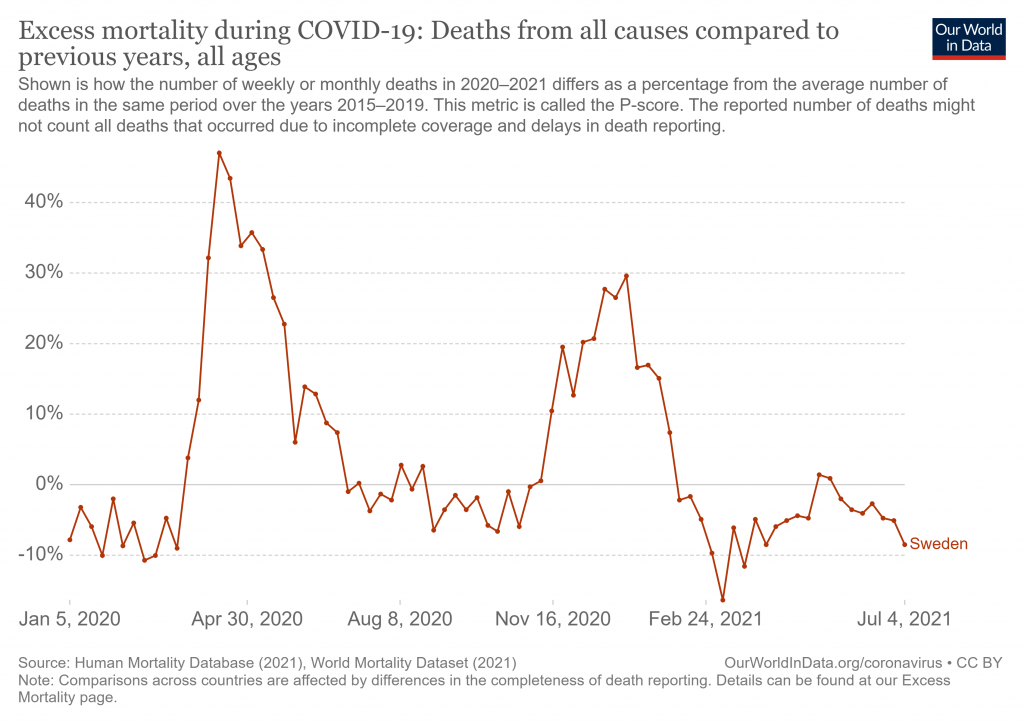
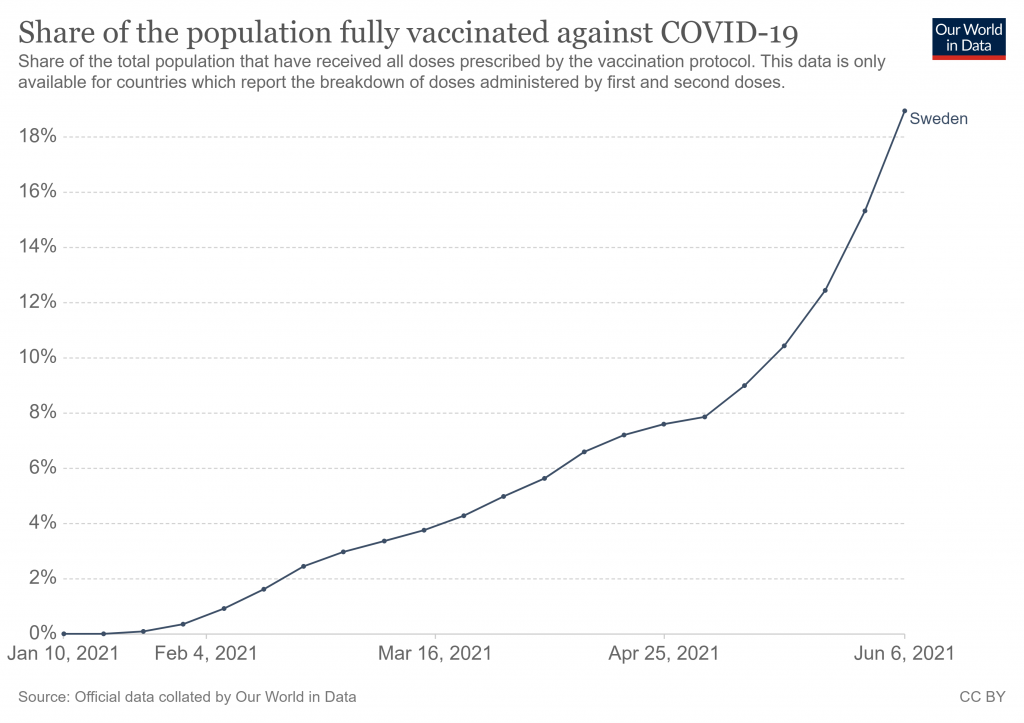
Christopher claims U.K. infections fell in January because of the lockdown, but fails to engage with the fact that Sweden’s fell as well without a lockdown. In an attempt to write-off the significance of Sweden’s example of light restrictions, he argues that it became Europe’s Covid “hotspot” in the early spring. In fact, while Sweden’s positive cases went high, its deaths stayed low, while its excess deaths went through the floor.
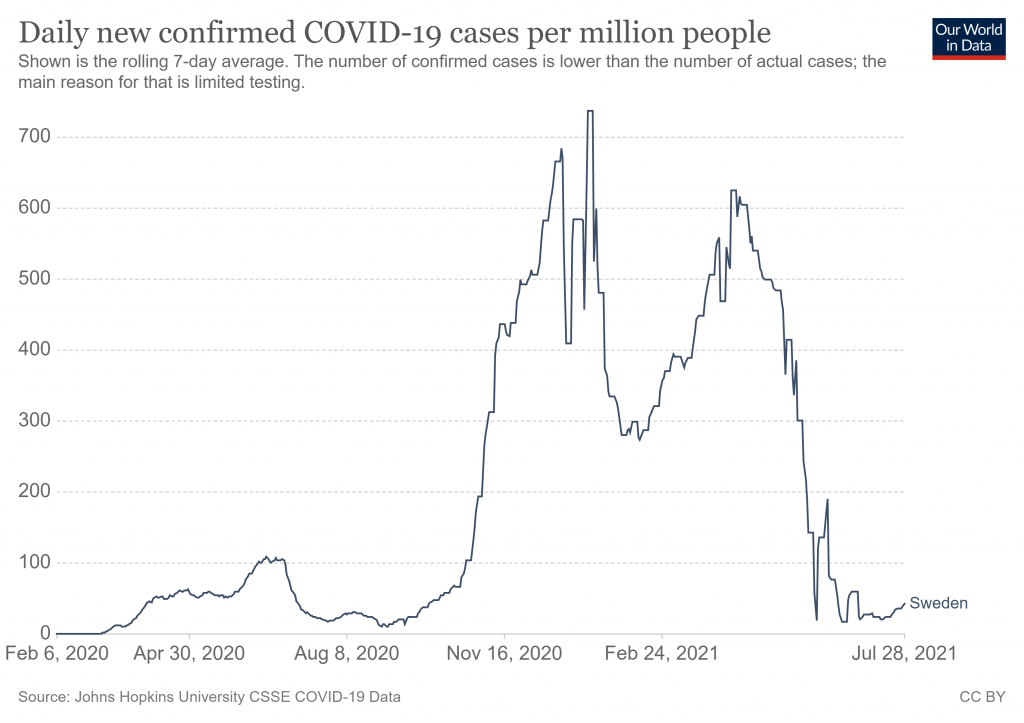
Apparently aware of this, Christopher argues that “in an encouraging sign of what was to come, vaccines began to have a clear impact on mortality in Sweden’s third wave”. Yet at the point that Sweden’s ‘third wave’ peaked in mid-April only 6.6% of the population was fully vaccinated, so it’s hard to credit that with having much impact on either infections or deaths. Infections in Sweden then entered sustained decline, again with no lockdown.
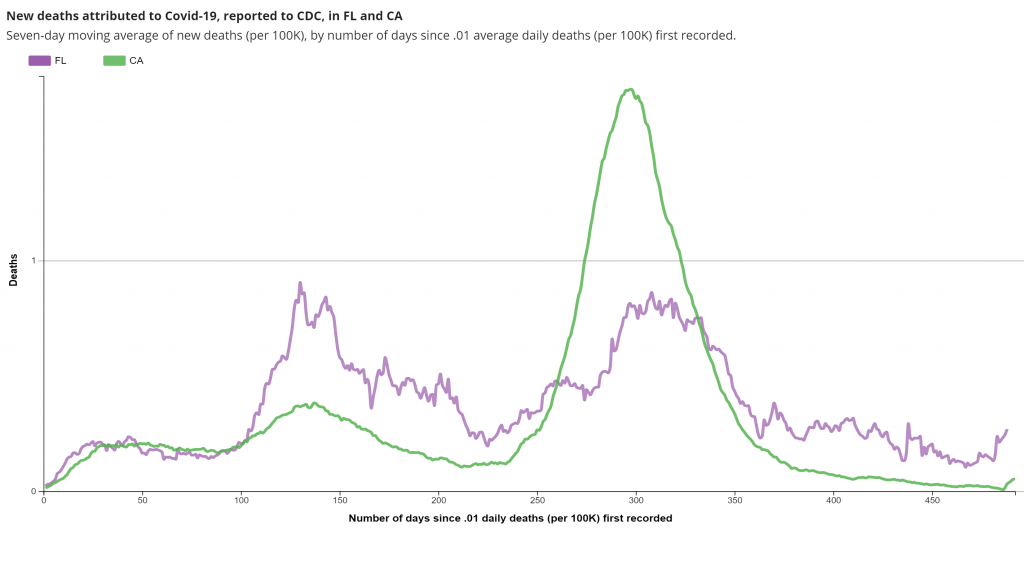
Florida is another place which defies the lockdown narrative, having lifted statewide restrictions in autumn 2020 and experienced a very similar winter to states which imposed harsh restrictions. Christopher, again, tries to dismiss its significance, saying it had a “large outbreak in the winter” and a “resurgence in early spring”. But the point is its winter outbreak was no worse than the outbreaks in lockdown states like California. And its spring ripple barely registered in additional recorded Covid deaths.
Christopher’s next iffy claim is that the U.K had an exit wave in spring: “As the U.K. relaxed restrictions and took a more Floridian approach, infections began doubling every two weeks.” This is not the case. The U.K., like a number of U.S. states, lifted many restrictions during the spring without seeing a new surge. In the U.K., as in the U.S., the surge only came along when the Delta variant arrived, not when restrictions were lifted – and in the U.K. it declined in July despite the lifting of restrictions.
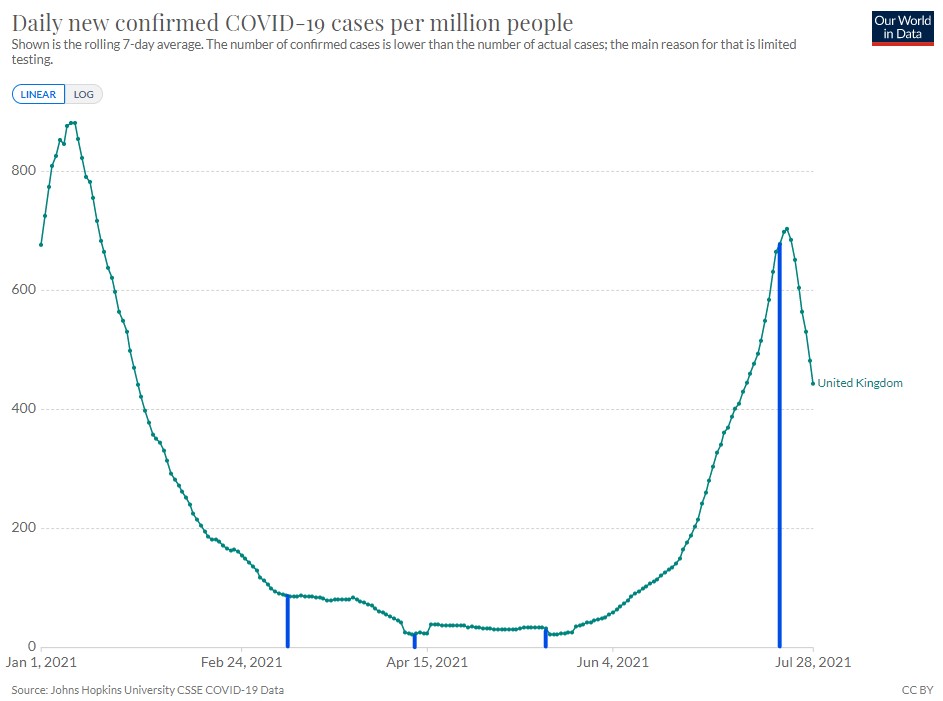
Christopher claims that it’s “the first time cases have dropped without heavy restrictions since the start of the pandemic”. If that was the case it is surely remarkable and demands explanation, particularly as Christopher believes that “herd immunity is unlikely to come from vaccination”, so he cannot join in the current trend of crediting the vaccines for the fall. But it’s also not true. Leaving aside that Sweden and numerous U.S. states saw infections drop without heavy restrictions, even in England infections have peaked and declined prior to lockdown on all three occasions – as Professor Simon Wood has shown in a peer-reviewed article, summarised in the Spectator.
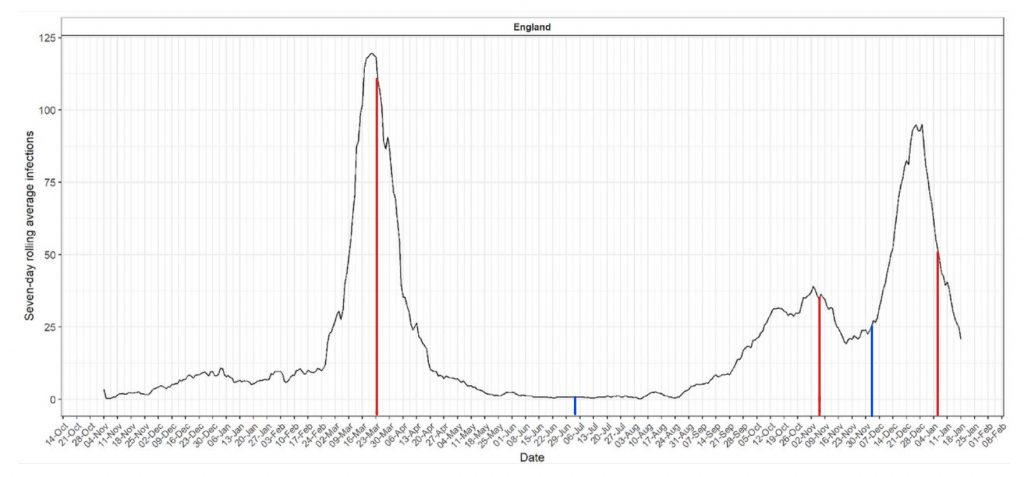
We can also see the same thing on the below graph from Imperial’s REACT-2 study, which reconstructs the infection curve from the (self-reported) symptom-onset date of those who tested positive for antibodies in their survey.
Christopher’s piece contains a number of other over-confident claims, delivered with uncharitable meanness and sneer, but it would become tedious to rebut every one. This will have to do for now. I’d like to think his next volley against sceptics (with whom I think he has more in common than he would like to admit) will acknowledge and engage with points like the ones set out here. But on past performance, somehow I doubt it.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
“sceptics (with whom I think he has more in common than he would like to admit)”
Well, it’s marginally less skin crawling that being lumped in with Piers Morgan, but please!
With his performance in the coronapanic, Snowdon goes in the authority-worshipping pseudo-libertarian bin.
Never heard of him.
Me neither.
He often writes for Spiked and The Telegraph. He’s anti nanny state and in fairness does not think people should be coerced into taking the vaccine. He’s right on most subjects but has been disappointing over Covid but personally I don’t cast people to outer darkness because we disagree on one thing.
A fair point, but the problem with the likes of Snowdon is that they cave when it’s most vital to stand firm.
He was far from the only resister to defect during the panickers’ winter offensive last year, that saw any chance of effective political resistance to lockdown finally destroyed, but his defection was particularly damaging because he has a position as a prominent “libertarian”. [I should say that my view of him as a defector is based on others saying that he was initially sceptical – I can’t say I noticed that myself, but I’ve no reason to doubt it.]
Didn’t he write some exposé about the American intelligence establishment?
That was Edward Snowdon.
That’s the good Snowden, with an e.
This Snowdon fills both the other roles, the Bad and the Ugly.
I know, brilliant book Permanent Record. I was being facetious.
I really don’t know what planet this one lives on, is he just trying to grab some attention? Was he a ‘spoilt child’ I wonder.
He craves respectability.
My previous experience of him was him sounding off about low-carb diets. I thought if anyone would benefit from a low carb diet it would be this fat moron. I ignored him ever since.
Medical Apartheid In Action – The New British Pub.
https://www.atangledweb.org/?p=91727
Stand in South Hill Park Bracknell every Sunday from 10am meet fellow anti lockdown freedom lovers, keep yourself sane, make new friends and have a laugh.
Join our Stand in the Park – Bracknell – Telegram Group
http://t.me/astandintheparkbracknell
A good putdown Will.
But you are omitting the Big One:
“The vaccines are a largely separate matter, and not all lockdown sceptics are vaccine sceptics and vice-versa.
The issues around the vaccines concern their novel genetic technology, the extreme speed at which they have been developed and approved under emergency authorisation, their questionable safety profile (with very high numbers of adverse events including fatalities being reported and serious side-effects being intermittently added to the warning label), and their real-world effectiveness.”
True, but the vaccines are, certainly now, just all about the vaccine passports.
And the vaccine passports are nothing but DISCRIMINATION and they open up a very nasty box of the Pandora.
They are not justifiable at all, neither medically nor morally.
Without the vaccine passports, the different test and quarantine requirements for and the coercion and discrimination of the unvaxxed, us lockdown sceptics wouldn’t care that much about the vaccines, only about the lies made in conjunction with them if and as they impacted us.
Yes – agree – but not mutually exclusive to the vaccines themselves still being a major ongoing concern. I actually agree with CS in that I do not believe vaccines are responsible for herd immunity based on the most vulnerable being killed last year via care homes etc., the increasing evidence this virus has been around well into 2019, the mildness of the virus for most who would hardly know they’d had it, T cell immunity, the ARR of the vaccines is very low, and the increasing evidence for gain of function hence the variants and increasing numbers of vaccinated people getting infected. The rollout needs to stop now and the entire cabal needs to be exposed for profiteering on fear and death.
I see no issue with being a vaccine sceptic.
In a free world I have the right to eschew any medical treatment. Likewise I don’t have to believe I am a racist because I am white or accept that men can be women. When you have your own brain and you are free of brainwashing you can calmly and happily say you are anti-vax and not worry what jabbed and masked fuckwits think. I am anti-vax. Fuck vaccines. I don’t care if some save lives because I now suspect there is pharma shenanigans involved with them all. Fuck the drug companies and fuck vaccines.
I hate this term ‘anti Vaxxer’.
What is it supposed to mean?
My kids were vaccinated for diptheria, rubella, measles, TB, whooping cough and mumps.
These vaccines were subject to long term trials, fully underwritten by FDA etc.
The Covid ‘vaccine’ isnt the same. Drug companies are exempted from liability. No long term trials. More deaths and side effects in the 4 months theyve been employed than EVERY OTHER vaccine combined fir the last 15 years.
I’m not ‘anti Vax’. I am absolutely against the injection of an experimental gene therapy which is being forced upon us.
Note to the LS editorial team: please stop using the terminology of our enemies.
It’s a weaponised word that has nothing to do with it original meaning and is now deployed to shut down debate and critical thinking. cf: racism.
Yep well put my sentiments exactly.
https://www.bournbrookmag.com/home/youd-have-to-be-nuts-to-call-me-anti-vax This one delves into the factual idiocy of the deliberate smearing go on.
The gene therapies are indeed deliberately mislabeled and sold as vaccines.
Berenson had a good thread on that issue recently.
And that lady actually thinks and makes a good case that they are bioweapons, which would explain most other things as well…
https://www.lewrockwell.com/political-theatre/deadly-shots-former-pfizer-employee-confirms-poison-in-covid-vaccine/
I hate this term ‘anti Vaxxer’.
I was about to say the same thing – I’ve had polio and TB vaccinations, I’ve had Tetanus jabs, I’ve had all kinds of jabs when travelling to parts of the world where there were viruses and bugs with a much higher fatality rates than Covid19 and on balance the risk of an adverse reaction to a properly tested vaccine shot (virtually zero) and catching a deadly virus or bug when overseas was not even questionable – a vaccine shot made perfect sense to me and I would have them again if travel restrictions were lifted … so I am by far not an ‘anti-vaxxer’ in the least … its a made-up word deliberately invented to shame and pressure people into having a jab where the mid-long term effects are unknown for a virus with a 99+% survival rate for the vast majority of people – many of whom have probably had the virus and didn’t even know it.
Agreed. By the way, I’m Spartacus too.
The general acceptance of case numbers and the drawing of conclusions from them is infuriating.
Surely any statistics based on PCR tests are going to be highly questionable? Since the test, properly used, requires a medical diagnosis of symptoms followed by a PCR test of 20, maximum 23 cycles, aren’t all claims based on PCR testing suspect?
We know, anecdotally, that numbers have been inflated by medical staff diagnosing covid on the most spurious evidence and that test cycles of 35 to 45 (currently in the NHS, I believe) have been used.
This unscientific inflation of cases is not new, by the way. The medical and pharmaceutical industries have form on this in their attempts to sell ‘flu vaccines. They fell flat on their faces with the swine ‘flu scandal some 12 years ago when they convinced Merkel to spend hundreds of millions on a vaccine which had to be destroyed after there were hundreds of cases of paralysis post vaccination.
The acceptance of PCR testing as the “gold standard” is laughable and makes all of the graphs shown above meaningless.
A little bit of clarity might enter the field if every “testee” were to demand how many cycles were to be used and were to refuse the test if they are symptomless.
Stop the testing, stop the “pandemic”!
But I agree with JayBee – it’s a good putdown! Good work.
The tests are illegal when required or mandated, as they are invasive and thereby impeding upon one’s right of body autonomy.
The self-exemption under common law that applied to masks should and does also apply with them and the vaccines, in the UK at least, too- this should now be established most urgently by lawyers here!
Their results aren’t useful medically as long as they aren’t standardized with regard to CT, kind and number of gene snippets searched for, confirmation cycle, swab procedure etc..
They are now even abused, to openly introduce double standards in order to manipulate case numbers (CDC max 28ct for unvaxxed only).
We don’t need to discuss the CT fraud much further, especially not Drosten’s ridiculous 45.
Most tellingly is that the CDC will suspend this and all other tests which can’t distinguish between Sars-Cov-2 and the flu soon.
This means, that the eradication of the flu last year was solely due to it being mislabeled as Covid!
Tellingly, health care workers here must now be jabbed mandatorily against the flu as well, not just against Covid!
Observers have already commented that this is the real reason for the CDC’s changed focus:
Cashing x2!
The tests are also given in breach of ‘informed consent’ ethics. When a test has been demanded on hospital admission, I have asked for information about the Ct threshold used (which, I think, informed people would agree is ‘essential information’). I have never had a response.
There is a kind of sleight of hand going on when people talk of false positives in relation to the PCR test. It may not be deliberate because there is a source of confusion with the terms used.
Suppose a manufacturer produced two tests.
Test A is a box that claims to test for exposure to the virus
Test B is a box that claims to test for infection with the virus
But inside boxes A and B is exactly the same test – they are identical, but marketed differently.
Test A could have a very low false positive rate in relation to its intended meaning. However, test B will have a higher false positive rate (in relation to its intended meaning) because it is, for example, picking up positive results from people who have had the virus, but are no longer infected.
The false positive rate for test A is the probability that you get a positive result for exposure when you have not been exposed to the virus.
The false positive rate for test B is the probability that you get a positive result for infection when you do not have the virus.
These 2 probabilities are not the same.
In fact we would have that
FP(test B) > FP(test A)
In maths terms we might write these false positives symbolically as
Test A : FP(test A) = Prob(e+ | no exposure)
Test B : FP(test B) = Prob(i+ | no infection)
What’s happening is that the 2 get confused and the false positive for test A is getting applied to test B, incorrectly.
It might be even worse than this because in practice we’re using the test to “determine” not just infection but infectiousness. So a better false positive rate for test B might be to work out the probability that one is told to self-isolate when there is no need to do so.
The false positive rate is not enough on its own anyway. The probability we really need is the probability I am not infected when I have received a positive result:
Prob(no infection | i+)
[see how the labels are flipped here from the probability that determines the false positive rate].
This more pertinent probability depends on the prevalence.
In times of low prevalence, with mass asymptomatic testing, you’re going to see a high fraction of positive results being due to individual test false positives.
As for the false positive rate itself (in either test) one potential source for time variation is, again, the prevalence. If some false positives come from sloppy lab technique and are as a result of cross-contamination, then when prevalence is high you have more potential sources of cross-contamination. I don’t know whether this is true, but it’s a plausible speculation.
… only part of the conundrums inherent in this.
The basic one is even simpler. What is the probability that what is being detected is actually a virus?
I was looking at the BBC death graphs last night for my own county, Northumberland. The graphs helpfully show the average deaths at particular times of the year as well as the ‘Covid’ ones. Being made up of rural and former coalfield communities, Northumberland has a high age demographic but it is starkly obvious that, whilst deaths in Spring 2020 were way over the average, deaths in Winter 2020/21 barely exceeded it. With a few outliers; mainly unhealthy, overweight middle aged men whose wives worked in hospitals (there are so few people here that we know who ‘out in the community’ has died), deaths were of old people in hospitals and care homes who would almost certainly have died of a respiratory virus this last winter anyway. They happened to die of this one. Cities may be slightly different but I suspect that this is replicated across the UK and was what Carl Heneghan said would happen.
That is, essentially, the national pattern. The number of deaths in nosocomial settings are a very high percentage and the normal pattern of mortality as it relates to age was not really affected.
Who the hell is he?
Exactly my thinking and why are we giving him so much importance in which to rebut his seemingly vacuous ‘arguments’? If he’s just a rude commentator who seems to be anti-vax and pro-vax at the same time and not even a scientist or doctor why give him so much space on DS? Perhaps Will Jones has some old feud going. Honestly, surely we have better things to discuss than have some sort of pub debate on here!
Overconfident, uncharitable, mean and sneering describes the arrogant Snowdon to a T.
It’s his default position.
The reason eminent Scientists and sceptics have been ignored and in many cases effectively silenced is because the pro-lockdown extremists CAN’T rebut their arguments.
I had a spat with him recently on Twatter over PHE data. He didnt like the fact that I pointed out in the under 50s deaths per case were basically the same in both the vax and unvax groups…and in either case came out at like 0.03%. He then insulted me as initially I said I had only looked at the under 50s and sarcastically called me a “busy guy” and told me I was more than welcome to “roll the dice” by not getting vaxxed. Idiot
Who is this guy? Why give him so much importance? He’s seems like just another pundit who has an opinion. So what. We’ve all got opinions here. Let’s focus on facts please and stop getting distracted by another bloke’s views. We may as well all be down the pub, arguing over our pints about percentages and statistics.
The Absolute Risk Reduction for the AstraZenica vaccine is ~ 1.3% and ~.098% for Pfrizer. The ARR figure is rarely broadcast. I wonder why. The Relative Risk Reduction figure is used to sell the efficacy of the vaccines. Let’s use a little analogy. If I buy a lottery ticket, I’ve realistically got no chance of winning. If I then buy another lottery ticket, relatively speaking I’ve increased my chances of winning by 50%. In absolute terms, I’ve still got no bloody chance!
0.98% for Pfizer – Typo
“The ARR figure is rarely broadcast. I wonder why.”
Because it’s not a relevant statistic. You want to know how much the vaccine will help *when* you catch the virus. It’s not a matter of if, but when.
This only ends at herd immunity remember.
I disagree.
It’s a very relevant statistic, since it reflects the overall real world risk, including the probability of actually getting the virus.
Has anyone tested what is really in a batch?
That would be interesting. I suspect some are weaponised. And some are saline. A mad experiment.. toward eventual depopulation. Of course for depopulation to be effective you would have to focus more on Africa, India, and China…
Fun fact: Stanley Johnson’s work at The Rockerfeller Foundation, where he was tasked to look at depopulation, formed the basis of what became Agenda 21 – a fact for which he is apparently very proud. [source Tom Bowers – The Gambler]
Check this report out.
https://naturalnews.com/2021-07-29-cdc-confesses-vaccines-are-failing-the-vaxxed-can-be-super-spreaders.html
Boosters anyone (in perpetuity)
Who is he? A virologist, an epidemiologist perhaps?
Re. the graph of Covid cases annotated with step 1-4 lockdown opening dates, it seems implausible to blame the June spike on the Delta variant as the covariants.org website shows that it had reached about 90% penetration by mid-June when the rise in cases (not delayed deaths) really took off.
It’s difficult to blame vaccine adverse reactions either as the build-up of vaccinations over this period has been smooth and steady.
I suspect the June spike in cases is an artefact. I wouldn’t put it past the corrupt establishment to have ratcheted-up the CT cycles on their PCR testing in order to find more “cases”.
Do I give a shit about who Christopher Snowdon is and what he thinks? (I had to search to find that he is connected to that dodgy lobby group – the IEA).
As with small children – don’t give significance-seeking wankers the attention they crave.
Surely everyone knows by now the vaxxines are pointless. They don’t work. Those who suggested they did and took them must be very disappointed. The thing I don’t understand is why is Joe Biden and Boris are still insisting people take them. I guess they can’t admit they were wrong.
Why do you even mention the guy? Never heard of him.
All Pandemics come to an end.
Only when politics sticks on a lab coat do they carry on for ever.
Just another petty tyrant jostling for position in the new regime.
This man is repugnant.
I wanted to capture Snowdon’s main assertions from his Quillette piece to see if they pass the test of time. 1) lockdowns (rather than shielding the vulnerable plus voluntary guidance) were the right and proportionate response to the pandemic; 2) vaccinating pretty much the whole of the population (rather than just the vulnerable) was the right policy; 3) PCR tests are a good diagnostic basis for finding covid-infective people; 4) vaccines have demonstrated their safety and effectiveness beyond reasonable doubt; 5) use of repurposed existing drugs (such as ivermectin) were correctly excluded as treatment options; 6) around 80-90% of deaths attributed to covid had covid as their principal cause of death; 7) seasonality is not a feature of covid.
https://blogs.bmj.com/bmj/2021/01/04/peter-doshi-pfizer-and-modernas-95-effective-vaccines-we-need-more-details-and-the-raw-data/