Back in October, when the critics rounded on the UKHSA for publishing vaccine data that didn’t fit the narrative, front and centre of their complaints was the claim that they were using poor estimates of the size of the unvaccinated population, and thus underestimating the infection rate in the unvaccinated. Cambridge’s Professor David Speigelhalter didn’t hold back, writing on Twitter that it was “completely unacceptable” for the agency to “put out absurd statistics showing case-rates higher in vaxxed than non-vaxxed” when it is “just an artefact of using hopelessly biased NIMS population estimates”.
To the UKHSA’s credit, while it conceded other points, it never gave in on this one, sticking to its view that the National Immunisation Management System (NIMS) was the “gold standard” for these estimates. It pointed out that ONS population estimates have problems of their own, not least that for some age groups the ONS supposes there to be fewer people in the population than the Government counts as being vaccinated.
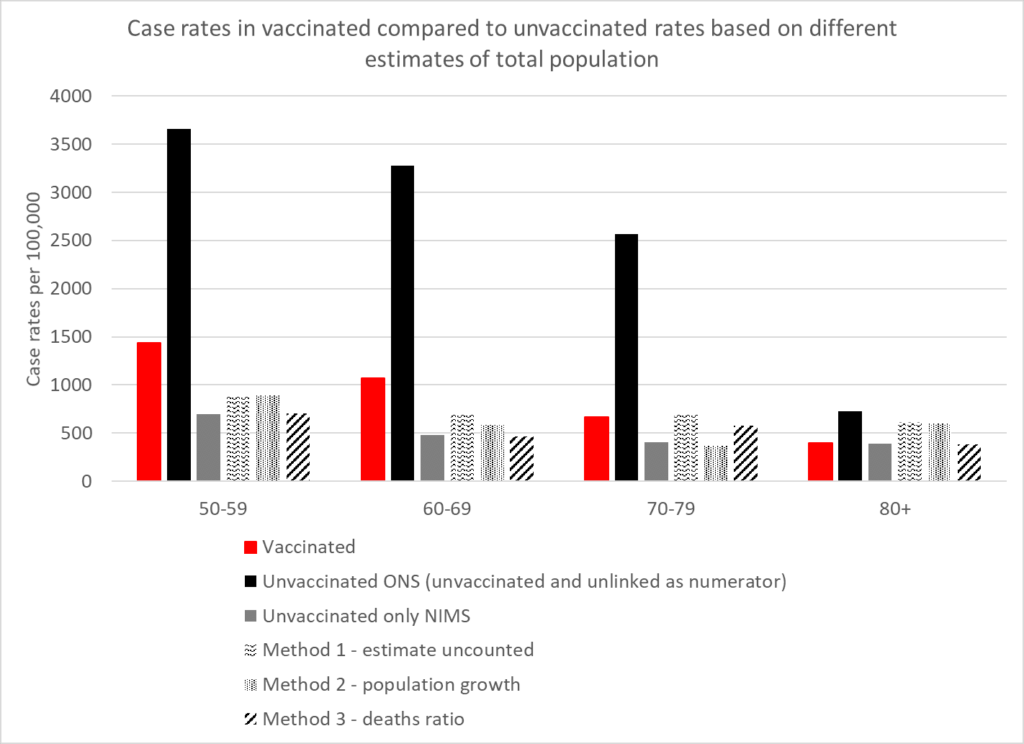
How can we know which estimates are more accurate? A group of experts has applied analytical techniques in order to estimate the size of the unvaccinated population independently of ONS and NIMS figures. Using three different methods, experts from HART found that estimates from all three methods were in broad agreement with the NIMS estimates, whereas the ONS estimate was a much lower outlier.
The first method involves recognising that people not within the NHS database system still catch Covid and still get tested. Assuming these people have the same infection rates per 100,000 people as the unvaccinated, you can calculate how many people there are outside of the database system and add these to the NIMS totals.
The second method involves looking at the rate of growth of people with an NHS number, which has been remarkably steady at around 2.9% per year. If you assume that people who are not yet registered in the NHS will sometimes become sick enough to seek healthcare, and thus a record will be created for them, applying this growth rate to the 2011 ONS population estimates give another figure for the total population.
The third method involves assuming that, in low-Covid weeks, deaths within an age bracket should occur at a similar rate in vaccinated and unvaccinated, allowing the size of the total population to be inferred from the percentage of deaths in the unvaccinated.
The results in terms of reported infection rates according to the five different estimates are depicted in the chart above. They show that the ONS is a clear outlier, its estimates sitting far too low, and NIMS is likely to be much more accurate. The ONS puts the unvaccinated population at around 4.59 million whereas NIMS puts it at 9.92 million, a difference of 5.33 million. That’s a lot of people not to be included in estimates, and suggests, among other things, that the ONS has not adequately estimated the magnitude of illegal immigration into the country.
As well as vindicating the UKHSA in its decision to stick with NIMS over ONS, HART’s analysis also indicates that, contrary to the assertions of Prof Spiegelhalter, the UKHSA data showing infection rates higher in the vaccinated compared to the unvaccinated is not a mere artefact of using the wrong population estimates. There may be other biases in it, but this is not one of them.
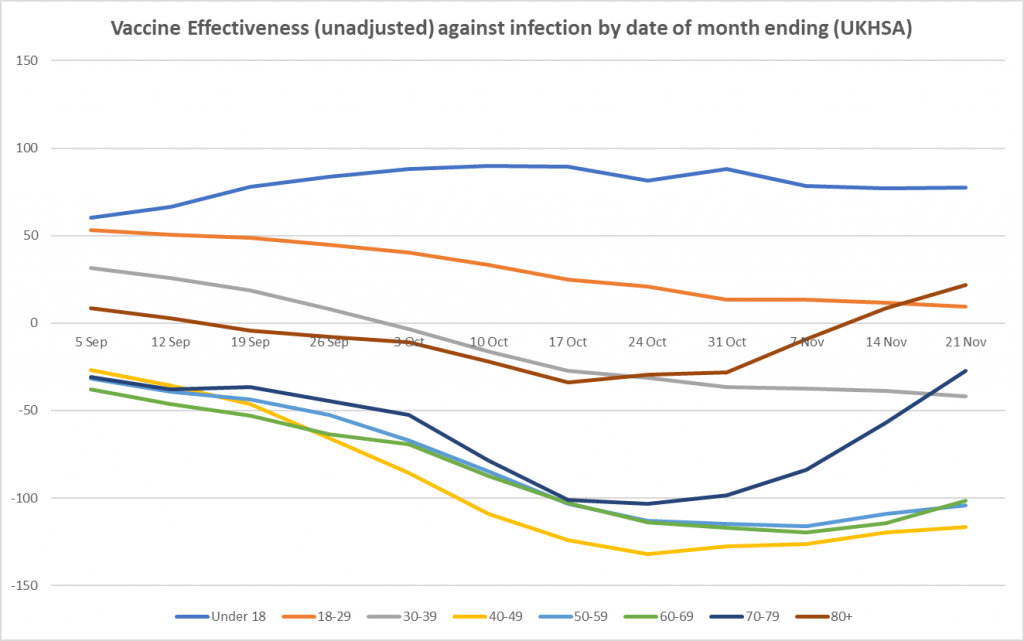
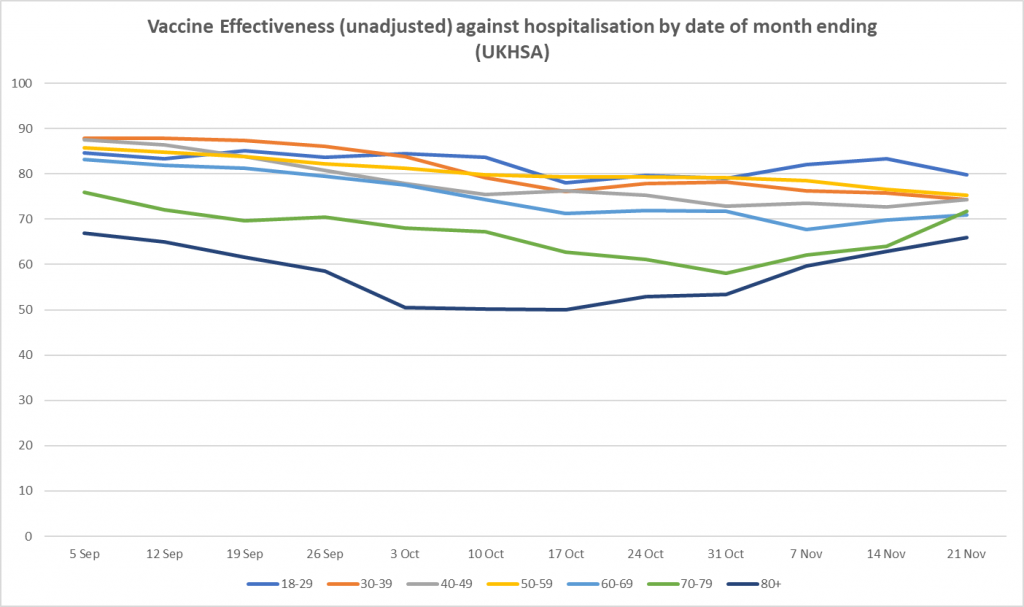
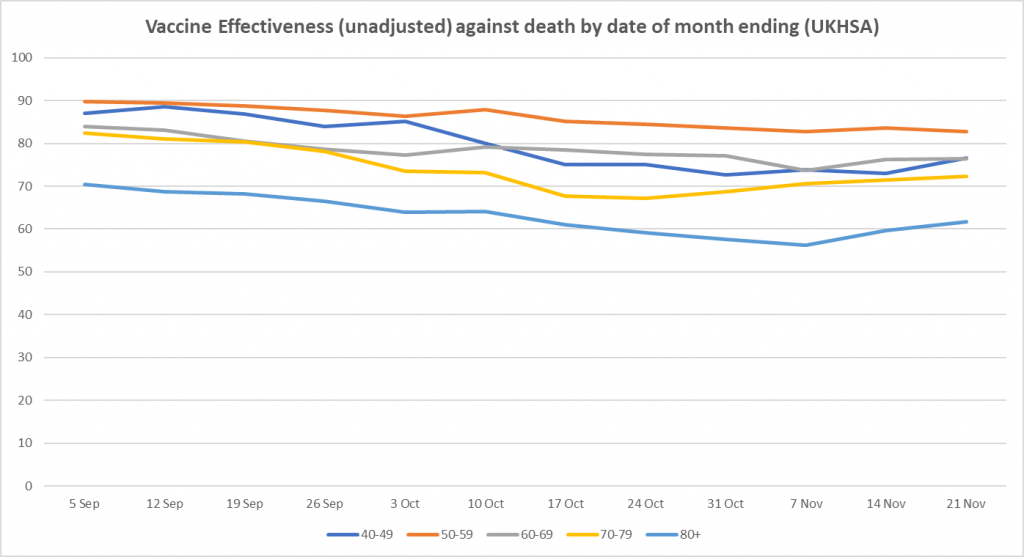
Here is the weekly update on unadjusted vaccine effectiveness based on the raw data in the UKHSA Vaccine Surveillance report. The unadjusted vaccine effectiveness estimates against infection have remained low in all adult age brackets this week, particularly in those aged 40-70, though there is little sign of further decline; in the older age groups (over 40), the recent vaccine effectiveness revival continues, possibly as a result of the third doses. There is also a sign of a rise in vaccine effectiveness against hospitalisation in the over-70s.














To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
“for some age groups the ONS supposes there to be fewer people in the population than the Government counts as being vaccinated.”
Hey, what do you bet that oldies are now 110% vaccinated – and counting?
Statistical manipulation that the Nudge unit wide boys now running the ONS insolently presume the rest of are too thick to notice.
Incidentally my Android keyboard capitalises the Nudge word as though it has some official standing or air of authority, does anyone elses?
nudge, fixed it.
Thank you for a clear presentation of the data. For the under 50 ages Covid remains a very low morbidity illness, vax or un-vaxed. For the 50+, especially 70+, it remains a net positive, which is of course where the whole vaccine program was supposed to be targeted. Now the key is to monitor 3rd dose impact on 50+ and see when it begins to decline.
It will also be interesting to see when these new treatments begin to rollout (especially monoclonal antibodies) and see the impact on survival rates for vax and not. Equally, impact of repeated dosing (4th, 5th) must be monitored to see impact on overall immune response.
Repeated dosing (4th, 5th)?
That’s an awful lot of dodgy experimentation on the population, most likely not at all to their benefit.
Better imo to accept that covid is not an emergency disease, never was, and halt all “vaccination” until the proper assessments of the novel treatments have been carried out – no emergency use authorisation when there is no emergency.
Even once that hurdle has been overcome, the state should not be funding such treatment unless a clear clinical need can be demonstrated in each individual case, as well as cost effectiveness (NICE) in general.
Of course, none of that is probably practicable, in political terms. But that just emphasises how unfit for purpose our politics is, and is no reason not to advocate for it.
“For the under 50 ages Covid remains a very low morbidity illness, vax or un-vaxed.”
This is an error often made amongst sceptics. It is a ‘low morbidity illness’ across the board. There is a slight elevation amongst older people – but not enough to change that statement; older people die at a greater frequency. The simple, telling, fact of the higher average age of death amongst Covid sufferers seems to be constantly forgotten.
“Equally, impact of repeated dosing (4th, 5th) must be monitored to see impact on overall immune response.”
On current evidence, and the lack of a rigid test regime, we should not be getting anywhere near 4th and 5th doses!
Certainly not multiple across the board jabs merely to gather the data that they ‘need’.
When did they stop categorizing deadly more contagious new variants with Ancient Greek letters, the latest being B1.1.529?
Its suggested ability to ‘evade immunity’
(Will create) “a potentially significant theat to the Vaccine Programme that we will have to protect at all cost” (Source ‘Whitehall Sources’)
So it’s not about saving the NHS anymore (at the cost if national ruination and the wrecking if countless lives) but just about saving the Just Vaccination Programme itself?
(Source BBC News online)That must be why they got Kerry Hurt and her husband Pat to urge others to take the vaccine after their own lives were ruined, crucified, destroyed weeks after getting the vaccine so that they could go on holiday to Turkey instead of which she had to learn to eat and talk again while she remains wheelchair bound and unable to go to the toilet by herself without yet starting proving that she qualifies under an old vaccine compensation scheme.
How much did they get paid to ‘Save the Vaccine Programme at all costs.’
“Urge others to take the vaccine” after what happened to her. Really BBC?
They should just cut to the chase and call it the “save the ass of those in charge programme”
Yup, that about sums it up although the description of Kerry’s vax ralated disablements coming from the BBC was something of a surprise.
Did you not get the memo? (When did they stop using letters of the Classical Greek alphabet to name variants?) The Ancient Greeks were racists! kept slaves! colonized foreign lands! admired beauty, and loved truth! The guilty parties who rushed to name the variants alpha, beta, etc. have been dealt with.
But now they use so-called ‘Arabic’ numerals, which originated in India. Isn’t that cultural appropriation?
Stats aside – the jab is a means to an end unrelated to health, has horrible side effects including death and has the sole purpose of bringing in passports and removing all your rights and autonomy- stitched up by corporate govt and its bought dogs… this is war. Insidious and deadly. Act, resist, connect.
Bringing in ‘vax passports’, aka movement licenses, followed by digital ID, digital currency and then the social credit system is but one objective of conditioning people into accepting experimental medical procedures when commanded – but there are many other motives for doing this. Schwab has told us many times that his, Prince Charles endorsed, Great Reset will forever change what it means to be human – and nanotech hardware is the means by which transhumanism will be achieved. How do you think they will get this experimental technology, including nanobots, gel chips, graphene oxide, neural lace and subdermal RFID systems, into every human on the planet? Once they have people accepting medical procedures ‘for the common good’ what is to stop them ordering mass sterilisation, organ donation or euthanasia? If they just wanted to bring in a ‘vax passport’, they could have injected everyone with a placebo and none of their present problems would have arisen. So no, its not just about the ‘vax pass’. Its about getting experimental, humanity changing, components into our bodies.
So no, its not just about the ‘vax pass’. Its about getting experimental, humanity changing, components into our bodies.
If it was just about vax pass then they would let those that have recovered get their immunity digitally certified too… but that clearly is not the case, so unfortunately it looks like you are right and they want everyone to have whatever is in these jabs.
Just learned that the origin of great reset is from 2019. G7 central banks agreed on ‘going direct reset’ in 2019 in Jackson Hole. Very little information circulates about this…
A fourth approach to analysis of the data applies common sense and experience: the people who from the beginning have lied about the virus and vaccines, are once more not to be believed.
Top ICU Doctor Suspended After Suing Hospital for Banning Life-Saving COVID TreatmentsIn an exclusive interview with The Defender, Dr. Paul Marik said patients are dying “unnecessarily and unlawfully” because the hospital where he is director of the ICU prioritizes expensive drugs like Remdesivir while banning more effective and less costly treatments.
https://childrenshealthdefense.org/defender/paul-marik-lawsuit-hospital-remdesivir-ban-life-saving-drugs/?utm_source=salsa&eType=EmailBlastContent&eId=b2e8747f-cbbc-42db-922f-1b6f7c9d1765
Marik filed his lawsuit against Sentara Healthcare on Nov. 9, arguing the organization is endangering the lives of its COVID patients by preventing him from using his treatment protocol, which he says has reduced mortality rates in the ICU from approximately between 40% and 60% to less than 20%.
The lawsuit alleges Sentara’s ban on the use of certain therapies against COVID violates U.S. and Virginia medical laws and the concept of informed consent — whereby “patients have the right to receive information and ask questions about recommended treatments so that they can make well-considered decisions about care.”
Pfizer, Moderna Vaccines ‘Dramatically Increase’ Heart Attack Risk, Renowned Cardiologist WarnsIn an analysis presented during a meeting of the American Heart Association, Dr. Steven Gundry, a pioneer in infant heart transplant surgery, said mRNA COVID vaccines put many patients at higher risk of a new acute coronary syndrome, such as a heart attack.
https://childrenshealthdefense.org/defender/sharyl-attkisson-steven-gundry-pfizer-moderna-vaccines-heart-attack-risk/?utm_source=salsa&eType=EmailBlastContent&eId=b2e8747f-cbbc-42db-922f-1b6f7c9d1765
In part, the analysis states:
“We conclude that the mRNA vacs dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy, and other vascular events following vaccination.”
Gundry explained:
“Recently, with the advent of the mRNA COVID-19 vaccines (vac) by Moderna and Pfizer, dramatic changes in the PULS score became apparent in most patients.”
Thousands of heart-related injuries have been reported following COVID mRNA vaccines. These injuries lead to the formation and progression of cardiac lesions which may become unstable and rupture, leading to cardiac events.
Jesus wept, they needed a study to tell them this!
Ambulances forced to queue daily outside A&Es, study suggests – BBC News
It’s funny how they deliberately don’t spell it out that the reason is staff shortages in A&E and you need to read the whole article to realise that that is the problem.
The way it is written it makes it easy for people to jump to the conclusion that it’s because the hospitals are out of space.
Hospitals are only ‘reaching capacity’ because their idiotic COVID protocols have reduced bed numbers by 40%. So in the midst of a ‘plandemic’ they’ve dramatically reduced the number of beds the country needs, just when folk need them? The gullible just keep taking the bait, better news – not a soul queueing outside the jabbatoir yesterday. At least the 4 members of staff stood outside are making a living out of this, better than paying them benefits.
And let’s not forget that the Covid fetish-rituals which lead to reductions in capacity don’t actually appear to make the slightest difference to the ability of the virus to spread – which it continues to do very effectively in hospitals.
Plus there is the inability to discharge medically fit but frail oldies due to having sacked all the sane carers…. So we’re back to the bed blockers…
A cynic would think that they’d done this to enable Plan B & vaxx passports to be introduced….
This has been happening for years ! In 2013 my husband died waiting for an ambulance. They were all queued outside hospitals waiting to offload patients. Oh, I forgot, there was one available but the crew ‘politely declined to attend because they were due a break’…….
What an awful thing to go through, I’m so sorry.
Covid19 vaccines have been authorised for tiny children aged 5 years old & up.
It’s public knowledge that there are ongoing trials in babies 6 months and up & it’s inevitable that they’ll be mandated also.
There’s no possible benign interpretation of any of this. The vaccines are horribly dangerous. They don’t work. Repeated injections are a reality with some countries planning 4th already.
I can’t see any reasonable person concluding other than this ends with substantial, deliberate loss of life.
For survivors, however many that might be, VaxPassWorld will be here to stay, with a database & algorithms deciding what you may or may not do.
It seems likely that with these preconditions established, it’s merely a complex technical issue to withdraw all sovereign currencies as well as cash & introduce central bank digital currencies (CBDCs). Many central banks have been openly exploring these, including programmable CBDCs. For example these can be set to expire periodically do you cannot save. High resolution geolocation may be used, for example, to disable your spending apps at 5miles from your home. This is the Great Reset & the end of the long era of Free Humans. Once established I regard reversing it as impossible.
Please think carefully about what you’re going to do.
Best wishes,
Mike
Dr Mike Yeadon
The USA borders close to non residents & citizens on Jan 22, 2022, who are not vaccinated. I’m talking about land borders from Mexico & Canada (I guess roads, railways & sea ports).
Since early November 2021, the unvaccinated are prohibited from flying into the USA.
Anyone considering visiting the USA should make sure you understand the constantly changing rules.
Anyone with a U.K. passport but no visa should be admitted to the US provided they have completed an online ESTA form (a visa waiver system). You can visit as a tourist for up to 90 days. You cannot work but otherwise there aren’t any restrictions once you’re in & you can move freely between states of the USA.
Some may rover to arrange a vacation of a few weeks, then find a reason not to board your return flight (you’ll need to show that return flight on border entry).
At that point, you’re an illegal, and if apprehended, I expect you’d be subject to deportation. How likely you are to be apprehended, I’ve absolutely no idea. Worth knowing that there have always been large numbers of illegal WORKERS, mostly in low paid agricultural jobs. The nation couldn’t operate without them. An illegal who isn’t working & is able to support themselves financially seem to me to be unlikely to be a high priority for removal. Then again, when did sense & logic apply these days?
Hope helpful. For avoidance of doubt, I am not advocating you go about breaking the law. But it’s becoming a matter of life & death in several European countries, where COMPULSORY vaccination has been announced. No longer will you be able to tough it out & accept restrictions.
Covid19 vaccines have been authorised for tiny children aged 5 years old & up.
It’s public knowledge that there are ongoing trials in babies 6 months and up & it’s inevitable that they’ll be mandated also.
There’s no possible benign interpretation of any of this. The vaccines are horribly dangerous. They don’t work. Repeated injections are a reality with some countries planning 4th already.
I can’t see any reasonable person concluding other than this ends with substantial, deliberate loss of life.
For survivors, however many that might be, VaxPassWorld will be here to stay, with a database & algorithms deciding what you may or may not do.
It seems likely that with these preconditions established, it’s merely a complex technical issue to withdraw all sovereign currencies as well as cash & introduce central bank digital currencies (CBDCs). Many central banks have been openly exploring these, including programmable CBDCs. For example these can be set to expire periodically do you cannot save. High resolution geolocation may be used, for example, to disable your spending apps at 5miles from your home. This is the Great Reset & the end of the long era of Free Humans. Once established I regard reversing it as impossible.
Please think carefully about what you’re going to do.
Best wishes,
Mike
Dr Mike Yeadon
https://www.lifesitenews.com/news/biden-to-require-covid-vax-for-non-american-essential-travelers-crossing-border/
I like modelling with accuracy population size, but we also have ageing rock-stars who can help us understand this complicated virus.
according to recent news here in Italy, doubly-vaxxed Canadian balladeer Bryan Adams has just landed in Northern Italy. At Malpensa airport he was tested, due feeling a bit unwell, and he was declared positive. Off to hospital!
it was mentioned that he’s probably been a “long shedder” as theoretically he caught covid a month or so ago, but ‘recovered’
more at https://www.ilgiorno.it/cronaca/bryan-adams-malpensa-covid-1.7077311
(ad-blocker might help to actually see the text, or just check instawhatsit)
https://www.instagram.com/bryanadams/?utm_source=ig_embed&ig_mid=A122EAA0-E9EB-48F2-9BC7-6AA9BF06A925
get well soon…..!
I thought covid didn’t infect vegans because they are too virtuous.
Professor Chris Whitty, UK government advisor, delivers a lecture at the Museum of London for Gresham College and is ridiculed on his comparison of past draconian measures exceeding those utilised in the Britain today.
https://www.youtube.com/watch?v=dUyAI6u0NDs&ab_channel=ResistanceGB
24th November 2021, London.
This is a letter I wrote three years ago about an ONS news release to boost flu vaccine uptake which overestimated flu mortality by 150 times. There was a controversy in 2018 when researches Hiam and Dorling established that excess deaths in the early months of the year had nothing to do with flu. Then suddenly the ONS pops up at the end of the year to pretend the 50k excess deaths were flu when this was known not to be the case.
https://www.bmj.com/content/361/bmj.k2795/rr-6
Government exaggerates flu mortality again: why cannot the public be trusted with the truth?I was perturbed and slighty astonished last week to see last winter’s excess mortality being largely attributed to the bad flu season, though it is well-established that this was not the case – the main culprit being on this occasion apparently the Office for National Statistics [ONS].
The BBC reported [1]:
“There were around 50,100 excess winter deaths in England and Wales in 2017-18 – the highest since the winter of 1975-76, figures from the Office for National Statistics show.
“The increase is thought to be down to the flu, the ineffectiveness of the flu vaccine in older people and spells of very cold weather last winter.”
The Daily Mail reported [2]:
“More than 50,000 excess deaths were recorded across England and Wales last winter, official figures show.
“Excess deaths refer to the amount of patients that died unexpectedly, calculated by comparing the mortality rate from winter months to the rest of the year.
“The shocking figures have been partially blamed on the deadly strains of flu that swept the nations over the colder months of December to March. ”
So the government are now apparent not only blaming fluctuations in winter mortality on flu but all excess winter mortality on flu, to the the tune of more than 50,000 deaths. The reality is that Public Health England had already published the flu mortality figures for the season in May [4]:
“Through the USISS mandatory scheme, a total of 3,454 ICU/HDU admissions of
confirmed influenza were reported across the UK from week 40 2017 to week 15 2018,
including 372 deaths, based on combined data from England, Scotland and Northern
Ireland. In England, the total number of influenza confirmed admissions to ICU/HDU
was 3,175 (rate of 0.22 per 100, 000 population) and 320 deaths during the same
period…
“The cumulative number of cases and deaths were higher compared to the 2016 to 2017
season (992 cases (rate of 0.06) and 112 deaths) and to the 2015 to 2016 season
(2,173 cases (rate of 0.14 per 100, 000) and 166 deaths) in England. This season
represents the highest number and rate observed since the beginning of the scheme
…”
On this basis, the number of deaths in England and Wales in an admittedly exceptionally bad year would have been only in the region of 335-340 deaths, and the ONS seem to have exaggerated the risk to the public by in the region of 150 times.
The House of Commons Science and Technology Committee have been complaining about low flu vaccine uptake again [5] but we do not even have any information about the vaccination status of the people who died. There are serious ethical issues both for medicine and government here which have yet to be addressed.
[1] ‘Excess winter deaths highest since 1970s, says ONS’ BBC Health 30 November 2018, https://www.bbc.co.uk/news/health-46399090
[2] Vanessa Chalmers, ‘Winter death toll highest since 1975: Failure of flu jab to combat severe outbreak resulted in more than 50,000 extra people dying in England and Wales last year’, Daily Mail 30 November 2018,https://www.dailymail.co.uk/health/article-6446399/More-50-000-people-di…
[3] John Stone, ‘Discrepancies in published data’, BMJ 2010; 340 doi: https://doi.org/10.1136/bmj.c613 (Published 02 February 2010)
[4] ‘Surveillance of influenza and other respiratory viruses in the UK: Winter 2017 to 2018’ , Public Health England May 2018, p 21, https://assets.publishing.service.gov.uk/government/uploads/system/uploa…
[5] Commons Select Committee: “Committee shocked by low uptake of flu vaccine”, https://www.parliament.uk/business/committees/committees-a-z/commons-sel…
“Imagine a new birth control pill, that allowed you to get pregnant, and required you to wear a condom, and be given to your kids who weren’t sexually active nor anatomically mature – for the sake of ensuring your neighbour didn’t get pregnant. REMIND YOU OF ANYTHING?”
Dr Anthony Hinton
On the French island of Guadeloupe the situation is escalating.
To control the situation, Paris has ordered special forces from the RAID and the GIGN to deploy on the Island.
Gun fights are now opposing anti green pass protesters to the Gendarmerie (military police), who is also deploying armoured vehicles to destroy burning barricades.
https://t.me/s/robinmg
Over the course of the so-called pandemic, I’ve been through a range of emotions, mainly clustered around the outraged/angry end of the spectrum. But now I just think it’s funny. Really hilarious. People like Prof Speigelhalter crack me up, with his cute cognitive dissonance, and his brainy strutting around getting all bent out of shape because the data doesn’t reflect his prejudices, and all the normal people going berserk about locking down the unvaccinated. Now, I just laugh, and enjoy the spectacle.
So, if you oppose a vaccine requirement, you are an anti-vaxxer. Well, an official NBC News Survey by Hart Research found that 50% of American adults opposed “requiring that everyone who is now eligible must get a COVID-19 vaccine.” It appears half of Americans are now officially anti-vaxxers.
https://aaronsiri.substack.com/p/a-majority-of-americans-are-anti
In reality, based on the more common, colloquial use of this term, even more Americans are anti-vaxxers. According to mainstream media, if you raise questions about the safety of COVID-19 vaccines – anti-vaxxer! If you raise questions about the efficacy of this vaccine – anti-vaxxer! If you question the FDA, CDC, or White House guidance on this vaccine – anti-vaxxer! If you want pharma companies to be liable for vaccine injuries – anti-vaxxer! If you want long term placebo-controlled trials prior to licensure – anti-vaxxer! If you raise concerns about breakthrough cases – anti-vaxxer! If you think natural immunity has anything to offer without a vaccine – anti-vaxxer!!
One problem is that pissing about with the elastic of ‘case’/’infection’ rates is never going to resolve any issues – it’s just another duff-data area. Even ‘hospitalization’ is a dodgy number. Too many confounders.
In the end, all we have, almost two years on, is still observations of all-cause mortality variations and – sticking to the coldly scientific question – “Is there any convincing evidence of ‘vaccine’ efficacy?”
To which the answer is a resounding ‘NO’. Everything else comes from that. Given the previously accepted high bar required for the judgment of new medications, this is sufficient to dismiss this experiment.
I’ve never understood the difficulty in providing a reliable estimate of relative vaccination rates. The authorities might not know precisely how many people are “in” the country due to illegal immigration as well as others dropping into homelessness and other marginal lifestyles – all very regrettable but inevitable and an argument for another day.
But surely the public health authorities know who they sent blue envelopes to? So if someones pitches up in A&E with a cytokine storm in their lungs and testing positive for SARS-Cov-2, but no record of an invitation for vaccination sent or pending, you just exclude them from your analysis.
That way you get to compare infection rates between the vaccinated on the one hand and refuseniks/yet-to-be vaccinated on the other. And unless there’s a plan afoot to lace the country’s heroin supply with Pfizer booster and getting addicts to innoculate themselves, I fail to see how they’ll reach marginal social groups anyway….
All the people who have never received a blue envelope are almost by definition unvaccinated. I suppose they could have turned up at one of those pop-up injection sites under a false name, but even then they’d end up in the system under that false name.
So, even with just a million people living under the radar, that’s one million to be added the “unvaccinated” column. Makes a huge difference when the official “unvaccinated” numbers are now so small.
I believe now the UKHSA, under guidance from Penn and Teller, are going to reclassify double-vax as unvax if their injections were a certain time period ago. This moves a pile of double-jab deaths into the unvax column. Et voila, vaccine effectiveness will go back up!
I think that is more likely to be the ONS game. The UKHSA is actually maintaining a semblance of scientific objectivity.
https://jermwarfare.com/blog/piers-robinson
When a government proudly boasts about perpetuating propaganda, it’s probably a good idea to sit upright, as Piers Robinson explained to me. Piers heads up the Organisation For Propaganda Studies and the Working Group On Syria, Propaganda, And Media, which means that he knows a lot about how governments and corporate media deceive.
WORLD’S FIRST VACCINE MURDER CASE AGAINST BILL GATES, ADAR POONAWALLA FILED IN INDIA’S HIGH COURT
“Petitioner has sought prosecution of AstraZeneca’s (Covishield) manufacturer Bill Gates, his partner Adar Poonawalla and other Government officials and leaders involved in the murder of a 23 year old man, who lost his life because of vaccination. The deceased took the Covishield vaccine by believing in the false narrative that the vaccine is completely safe and also owing to the compliance requirement set by the Railways that only double vaccinated people would be allowed to travel.”
https://indianbarassociation.in/worlds-first-vaccine-murder-case-against-bill-gates-adar-poonawalla-filed-in-indias-high-court/
This is the chart you get from this 1st November ONS publication for the over 80 group.
If you switch to NIMS for all the data (the numerator and denominator) then suddenly (not shown here) the apparent differential in all cause mortality disappears.
The differential disappears in all the 4 age bands for which ONS provided data, over 80, 70-79, 60-69 and 10-59.
Note you have to do some adjustments to remove the age confounding with the 10-59 age group, but when you do again there is a differential that disappears when you move to NIMS for denominator and numerator.
There can only be two realistic explanations
a) NIMS for denominator and numerator (as per the UKHSA vaccine surveillance reports) is much nearer the reality than using ONS for the denominator
b) there is some element of selection still going on where unhealthy people have had a greater tendency to not get vaccinated, and this selection effect is not just initial selection but long term selection.
Because the apparent difference in mortality between vaccinated and unvaccinated occurs in all these 4 age groups of the ONS data, but the initial selection (the non vaccinated hump in mortality shown here) reduces in relative size as we go down the age groups, then it suggests to me that a) is by far the more important of these two affects.
And here’s the same chart but with the different vaccination statuses separated out (I’ve not shown the second jab group separately but the vaccinated group is a combination of all categories of jabbed)
There is the initial selection of the most ill not being able to get vaccinated. This is the green hump as unvaccinated numbers reduce and a disproportionate number of the very sick remain in the unvaccinated group as the more healthy leave to the single jab group. This has been discussed before
And then there’s the selection of those who are unable to get the second jab because they are too ill. This is the red dotted hump after second vaccinations happen, of the single jabbed who are left behind as the healthy exit the single jab group to the second jab group. Again that has been previously discussed.
But notice also the red dashed hump around 5th March (the within 21 days of first jab group). This is likely to be people who were too ill to get their first vaccinations in January, perhaps because they were ill in hospital at the time, but had perhaps been discharged from hospital, were still quite ill but well enough to get their first jab. The late first jabbers show up as the red dashed hump.
What this all suggests to me is that there was an initial selection effect where the most ill couldn’t initially get jabbed, but most/many of these people (at least those who survived) have now been jabbed if they’ve chosen to.
So this is why I think the selection affect is mostly an initial selection affect and not a significant long lasting selection affect. And hence why the unvaccinated proportion must be understated in this ONS analysis. And why the unvaccinated proportions used by UKHSA for their vaccine surveillance reports is more realistic than the ONS figures.
Note some ethnic groups who have typically experienced higher mortality than the white ethnicity group are disproportionately within the unvaccinated group. So we can’t rule out b) above having some affect.
https://eugyppius.substack.com/p/ukhsa-efficacy-stats-death-watch-ea9
His take on these numbers.
Latest from eugyppius:
https://eugyppius.substack.com/p/ukhsa-efficacy-stats-death-watch-ea9
What are the black bars? I don’t understand what “unvaccinated and unlinked as a numerator” means.
I get confused by same but the original article explains better. https://www.hartgroup.org/what-is-real-world-vaccine-effectiveness/
Joe Rogan said his doctor, Pierre Kory, is part of a group that has used Ivermectin to quietly treat 200 Members of U.S. Congress for COVID19. Dr Simone Gold, from America’s Frontline Doctors, told that she has prescribed treatments for Congress. She still believes in her oath, but she is vocal saying she has been contacted by many in DC. Can you believe these demons? Healing for them are OK but not for us. Get your Ivermectin while you still can! https://ivmpharmacy.com
Am I right in assuming that better vaccine effectiveness in the younger is because they are less likely to be Ill or die anyway, wether vaxxed or not?