
In the US, Southern states have the lowest vaccination rates, while North Eastern states have the highest vaccination rates. This pattern appears to be largely down to partisanship: Republicans are less likely to be vaccinated than Democrats.
At the end of August, when the Delta variant was dominant, case rates were highest in Southern states like Alabama, Georgia and Florida. Meanwhile, they remained low in North Eastern states like New York, Massachusetts and New Jersey. This is shown in the map below, which gives the official case curve for each state up to 26 December:
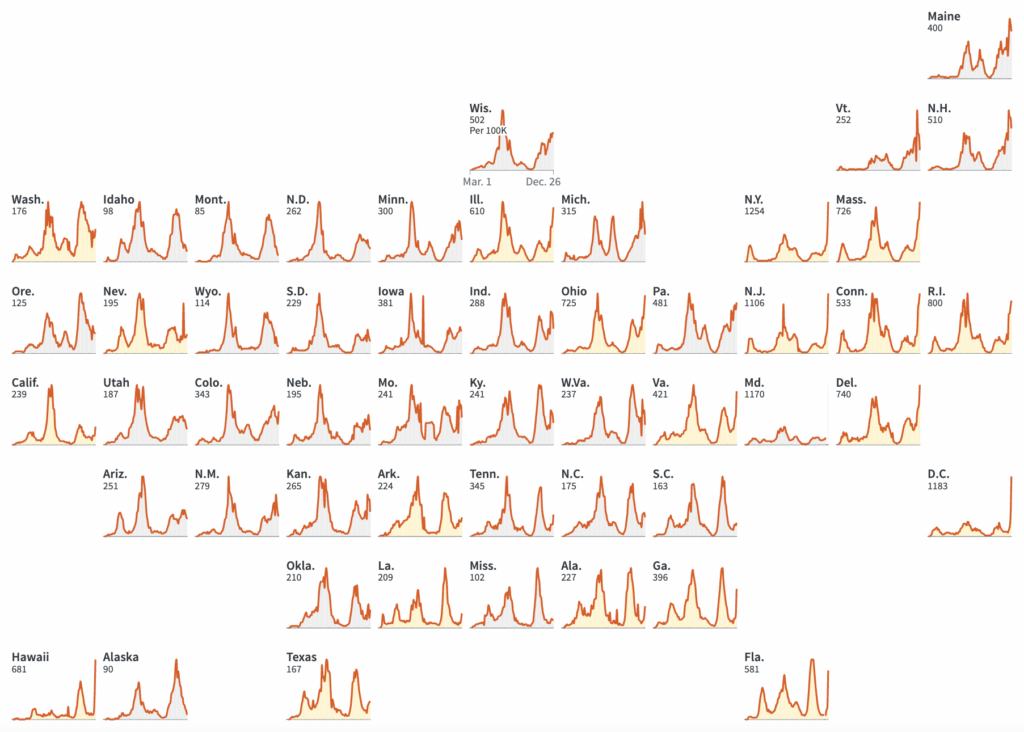
The much higher case rates in the South seemed to provide evidence that the vaccines stop infection (in addition to protecting against serious illness and death). Hence, it was believed, vaccine passports will help to curb transmission.
Fast forward three months, and the situation is rather different. Infections are now surging in the North East. This has led to the somewhat peculiar situation whereby case rates are highest in some of the most vaccinated states. See the chart below, based on data from the CDC:
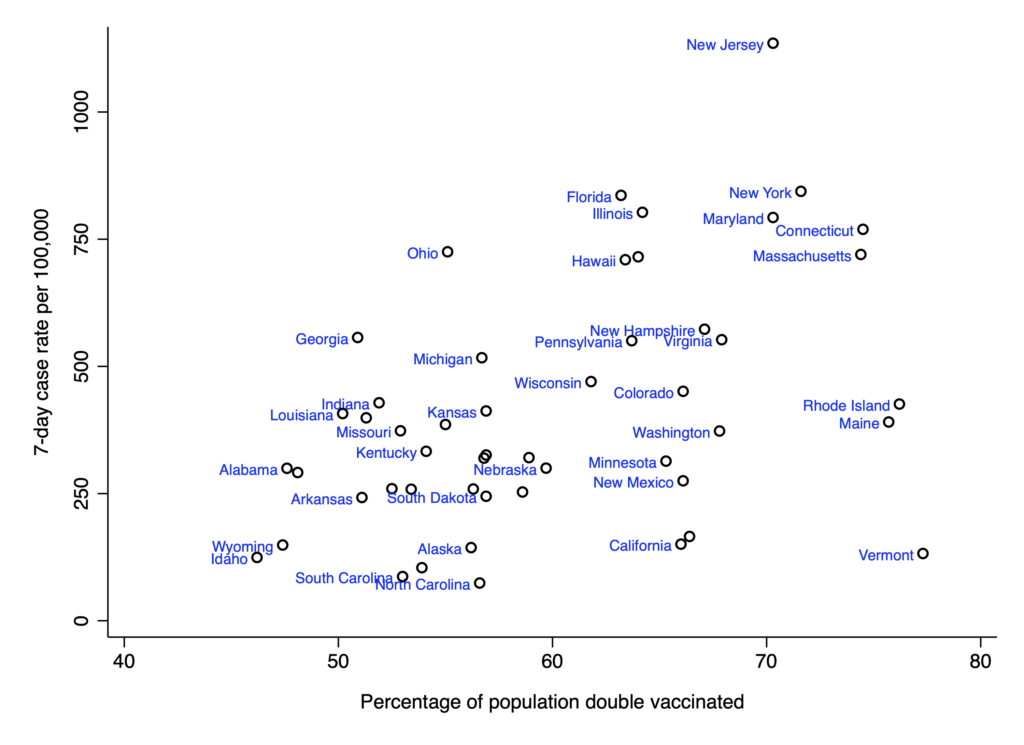
What explains this? One factor is waning effectiveness against infection. A few months after vaccination, you’re not that much less likely to become infected than someone who’s never been vaccinated.
Another factor is regional clustering. Case curves seem to be strongly correlated within regions of the US. This is probably due in part to seasonality. But it could also be due to the simple fact that transmission is more likely to occur between neighbouring states than between ones that are far apart.
A third factor is the spread of Omicron. This mysterious variant has immune escape properties, rendering both the vaccines and natural immunity less protective. And there’s even evidence of negative vaccine effectiveness – i.e., that double-vaccinated people are more likely to catch Omicron than the unvaccinated.
While offering vaccines to the elderly and vulnerable makes sense as a way to achieve focused protection, it’s clear that high vaccination rates in the North East have not curbed transmission. Vaccine passports don’t work in Europe, and they don’t work in America either.














To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Further proof that this is all about controlling us so that the rich can go wherever they want without bumping into plebs all over the place.
He is Elite don’t you realise that? he is so much more impotant than us plebs, Know your place just pay your taxes so they can live off you like the parasites they are.
“Impotent”.
Small but significant typo I presume.
If only that were the case, but these bu**ers want to pass their riches on to their offspring.
Nuff said!!
“All animals are equal, but some animals are more equal than others.”
I’m left wondering what work was so vital that he had to fly in to do it in person, but only took one day.
Aside, does anyone know the cargo capacity of a Gulfstream G650, expressed in sacks of gold?
yes, or telling someone something (or hearing from someone) that there couldn’t be an electronic or paper trail for
ie backhanders/corruption/you scratch my back etc
anything else can be done on zoom
About £130 Million at todays price. Only about 33 gallons of gold though.
Well that’s my ready made excuse for not ever quarantining. Don’t you know I run a massive bank? Get out of the way peasant.
Well, I can tell you, I really DO have a large bank (at the far end of my garden)!
And yet even Santa had to prove his Covid status to get into the Tesco ad.
The only miracle there is that he wasn’t black like everyone else on TV ads is now.
i am running a competition with my friends to see who spots the first one, but maybe that is one step too far for even wokey-blokeys.
I think Kwanzaa involves the veneration of Saint George.
Zwarte Piet on ads?
banking is simple
you borrow money at one timescale and lend at another
make money off the interest rate difference
what these people do is investment banking. convince you they are clever then invest your money. take a cut whether you win or lose. shysters
Don’t forget also packaging debts up into incomprehensible financial instruments to hide the risk!
“Money talks, virus walks”
Rules for thee but not for me.
Hong Kong was the birthplace of HSBC, a competitor to JP Morgan. It would have been fun to watch Hong Kong quarantine the head of a competitor “for health and safety reasons” for, say, several weeks. 😉 A missed opportunity!
Rich person avoids rules, as old as history
There is an ivermectin panic on the big tech and MSM right now. Massive articles from MSM on Ivermectin trying to push a danger narrative and also negative press on Americans Frontline Dr’s, again, to keep the Covid narrative alive. Just go to the Goog and type ivermectin then look at all the panic news articles. We are over the target. Big-Pharma is panicking. This medicine has been widely used by humans without any problems for 40 years. It’s inventor won a Nobel Prize after 20 years of successful use and after 100 million people were cured of a broad spectrum of problems without any side effects. Get your Ivermectin while you still can! https://ivmpharmacy.com
Our PM would be OK then, he’s always been a great big banker
Nice. One rule for me, one rule for thee.
In other words the NWO working with China is breaking down HK. the thousands of entrepreneurs who live and work there will gradually go bankrupt and only the big China affiliated banks will be allowed to survive. Taiwan will also be totally controlled by CCP within the next couple of years and Tibet will be completely broken. This is Communism taking over and many of our own Globalists want this system in the West.
Amazing, isn’t it, that this virus has the intelligence to avoid infecting Very Important Persons (or very rich ones)?