
The latest UKHSA Vaccine Surveillance report was released Thursday, and its authors are now bending over backwards to keep their critics happy. Following a telling-off this week from the U.K. Statistics Authority, the UKHSA’s Head of Immunisation, Mary Ramsay (pictured above), published a blog post explaining what they’ve done to appease their detractors, while the report now states no fewer than four times, twice in bold typeface, that “these raw data should not be used to estimate vaccine effectiveness”. Ramsay grovels:
To make our data less susceptible to misinterpretation, the U.K. Health Security Agency has worked with the UK Statistics Authority to update some of the data tables and descriptions in the report, specifically around rates of infection in vaccinated and unvaccinated groups. In our commitment to transparent and clear data, we regularly review our publications to ensure they reflect the current situation within the pandemic, and we will continue to work with our partners at the statistics bodies, to ensure our reporting is as scientifically robust as possible.
As I noted last week, the UKHSA does not accept the criticism of its population estimates levelled by, among others, David Spiegelhalter, who declared that using them was “deeply untrustworthy and completely unacceptable”.
The agency instead takes the view that the problem is systemic biases in the data which mean it “should not be used” to estimate vaccine effectiveness. But as I have noted repeatedly, those biases just mean that the estimate will be of unadjusted vaccine effectiveness, which is a perfectly legitimate quantity to estimate and has its uses, particularly when looking at trends or when there is reason to think the biases may be relatively small. (For instance, a recent vaccine effectiveness study in California adjusted its raw data for 22 different factors but in almost all cases the adjustments were tiny.)
The UKHSA report itself correctly gives the definition of vaccine effectiveness: “Vaccine effectiveness is estimated by comparing rates of disease in vaccinated individuals to rates in unvaccinated individuals.” The U.S. CDC, likewise, states the definition as “the proportionate reduction in disease among the vaccinated group”. The CDC distinguishes “vaccine efficacy”, estimated from controlled studies, from “vaccine effectiveness”, which is used “when a study is carried out under typical field (that is, less than perfectly controlled) conditions”. It is therefore not appropriate for the UKHSA, a Government agency, to insist that its data “should not be used” to estimate vaccine effectiveness, which is a false statement and amounts to attempted Government censorship of scientific enquiry.
The report explains that “vaccine effectiveness is measured in other ways as detailed in the ‘Vaccine Effectiveness’ Section.” However, that section is clear that each estimate “typically applies for at least the first three to four months after vaccination”, and “there may be waning of effectiveness beyond this point”. The report discusses this waning, but only for the Alpha variant: “Data (based primarily on the Alpha variant) suggest that in most clinical risk groups, immune response to vaccination is maintained and high levels of VE are seen with both the Pfizer and AstraZeneca vaccines.” What use is data based primarily on the Alpha variant, which went almost extinct around six months ago? There is no attempt to present adjusted estimates of vaccine effectiveness based on the most up-to-date data. Instead, we are just given repeated insistences that the data is not showing what it appears to be showing because it is subject to unquantified biases.
What are those biases? Last week the report claimed that vaccinated people “may engage in more social interactions because of their vaccination status”, which didn’t fit with the more usual idea of unvaccinated people as a less cautious sort. Neither did it fit with the other reason they gave, that the vaccinated “may be more health conscious and therefore more likely to get tested for COVID-19”. This week they kept the latter but changed the former to the entirely ambiguous: “People who are fully vaccinated and people who are unvaccinated may behave differently, particularly with regard to social interactions.”
The other two biases they suggest are that “many of those who were at the head of the queue for vaccination are those at higher risk from COVID-19” and “people who have never been vaccinated are more likely to have caught COVID-19” previously. (The latter they say gives a person “some natural immunity to the virus for a few months”, which seems a very pessimistic view of natural immunity, particularly seeing how optimistic they are about the effectiveness of the vaccines.)
The report asserts categorically that the unvaccinated have higher previous infection rates, but cites no evidence to support this. Why not? Why, almost a year into the vaccination campaign, are researchers still so often waving their hands when talking about the differences between vaccinated and unvaccinated groups? Where is the published data? Precisely how much more likely are the unvaccinated to have had a previous infection? This is a simple data comparison. Why hasn’t it been done? The study in California mentioned earlier found that 2% of the vaccinated had recovered from Covid against 2.3% of the unvaccinated, so not a large difference. Is England similar? Why don’t we know? Likewise, how much more likely are vaccinated people to be tested? This is just a comparison of the testing rates in vaccinated and unvaccinated populations. Why hasn’t it been done? This is not good enough. We want more data from UKHSA, not lectures on how not to use the meagre amounts of data they release.
In her blog post, Mary Ramsay points to studies PHE (UKHSA’s predecessor) has published in the past:
These factors are all accounted for in our published analyses of vaccine effectiveness which uses the test-negative case control approach. This is a recommended method of assessing vaccine effectiveness that compares the vaccination status of people who test positive for COVID-19, with those who test negative.
This method helps to control for different propensity to have a test and we are able to exclude those known to have been previously infected with COVID-19. We also control for important factors including geography, time period, ethnicity, clinical risk group, living in a care home and being a health or social care worker.
While PHE did publish such studies earlier in the year (I analyse them here and here), they have not published anything based on data more recent than May, over five months ago. This was just as Delta arrived, and before infections surged over the summer and the raw data started showing infections in the vaccinated eclipsing those in the unvaccinated.
So where is the update? It’s all very well writing pages at the behest of the U.K. Statistics Authority policing how people use your data, but where are the studies setting the picture straight? We’ve had studies from California, Sweden and Israel using data from over the summer, all showing sharp decline in vaccine effectiveness. Where is the U.K.’s contribution to this emerging understanding of the vaccines?
Yes, we had that dubious study in August from Oxford University based on the ONS Infection Survey. But there’s been no update from UKHSA to its studies based on Government testing data.
Here’s a suggestion. Why don’t Daily Sceptic readers write a (polite!) email to the UKHSA’s Mary Ramsay (address here, Twitter here) asking for an update on their very useful test-negative case control study with data from the summer and autumn. You might say you have been concerned about the data in their Vaccine Surveillance reports showing high infection rates in the vaccinated compared to the unvaccinated, but note they say vaccine effectiveness can only be properly estimated in a study, so would be grateful for an update on this.
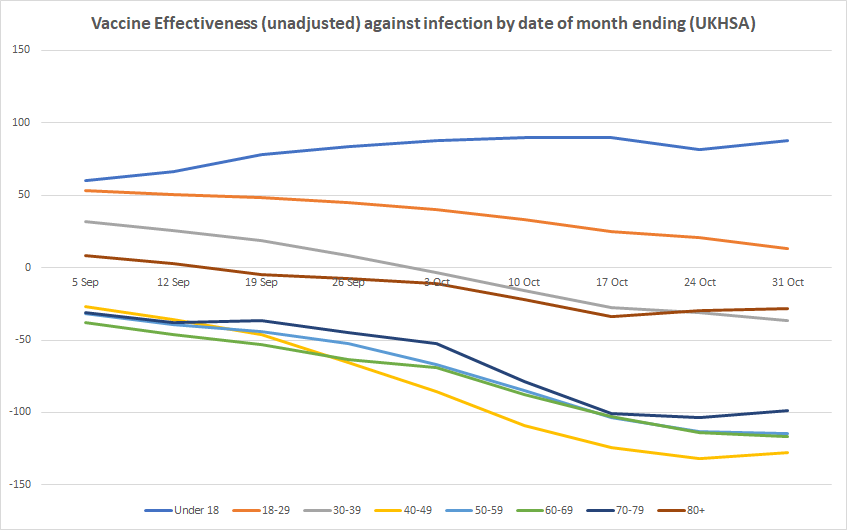
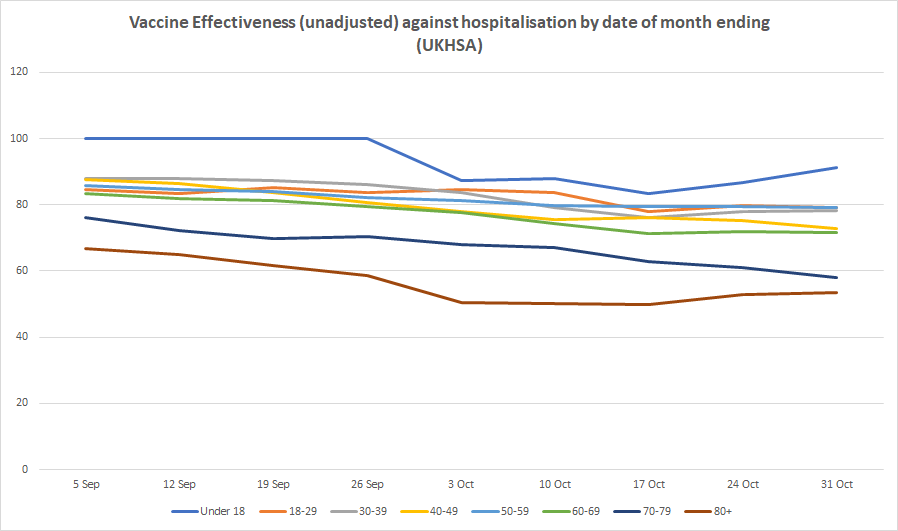
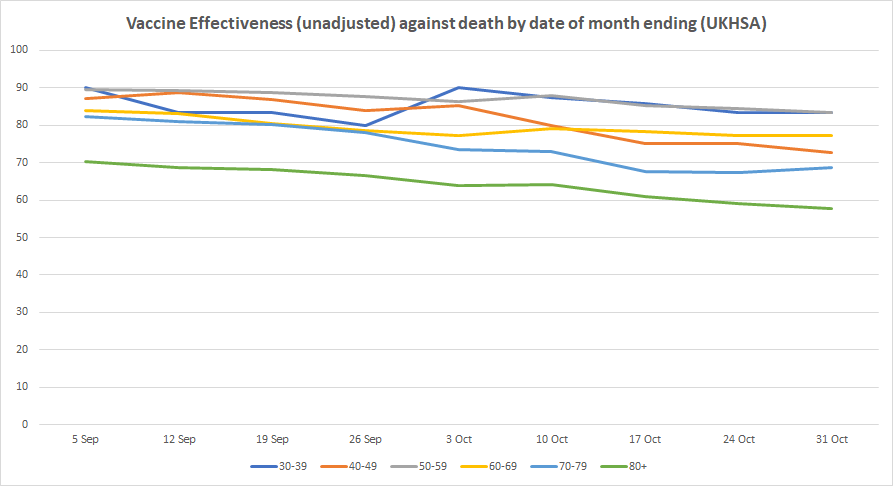
Here’s this week’s table of unadjusted vaccine effectiveness and the updated graphs showing how it is changing over time. It shows infection rates currently twice as high in the vaccinated compared to the unvaccinated for those aged 40-79, corresponding to an unadjusted vaccine effectiveness of minus-100% or more. Vaccine effectiveness is negative for all over-30s, and almost zero for those aged 18-29 (and still declining). It remains high for under-18s, and effectiveness against hospital admission and death is holding up. This week the decline appears to have stopped, or at least paused, in most age groups.













To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Serial liars and deceivers always tie themselves up in knots in the end. When UKHSA try to dismiss their own data and findings, you know they are up to two things, a) They are lying to you, and b) They have some rather inconvenient information that they would rather you did not know…
Or alternatively, they don’t know what they are doing. Either way it doesn’t exactly fill you with confidence, does it.
Bone marrow and the control of immunity (nih.gov)
“Research obtained by a group of scientists shows the COVID vaccine spike protein can travel from the injection site and accumulate in organs and tissues including the spleen, bone marrow, the liver, adrenal glands and in “quite high concentrations” in the ovaries.”
‘We Made a Big Mistake’ — COVID Vaccine Spike Protein Travels From Injection Site, Can Cause Organ Damage • Children’s Health Defense (childrenshealthdefense.org)
So the jab may be interfering with the immune system?
But they don’t dismiss their own data and findings. They just point out what it is useful for and what it is not useful for.
Data, according to government bodies:
Does that sum it up accurately?
Spot on. We need to stop making excuses for these inexcusable minions of a treacherous administration, suddenly and gratifyingly hoist with their own petard.
https://eugyppius.substack.com/p/ukhsa-efficacy-stats-death-watch
How do I know it is the weekend – because you trot our more specious bollox. “useful” to whom? Just as the Pfizer booster jab – using the S1 spike protein of the Alpha variant – that died out many many months ago – but ignores the impact of the Delta variant – is a meaningless exercise, the continued refusal to publish the incidence of infection between jabbed and unjabbed is indefensible. The availability of data from around the world that does show a distinct pattern of infection following “two jabs” makes Ramsey/UKHSA ex pHE a laughing stock.
It is a very serious demonstration of the abandonment of professional ethics for these alleged professionals to promote the narrative dictated by politicians where it demonstrably involves the use of partial data – something that has been shown to be the case time and time again since Downing Street “press briefings” started ; presumably you are happy with that level of bias? As you have a gullible and blinkered excuse for the swathe of wrong headed policies which characterise the UK’s government’s “official response” to SARS COV2/CV19, I think you should change your blog name to Captain Queeg.
Nope, it does not. But it also means that any person employed by the UKHSA who is a member of an accredited professional body, meaning they have signed up to a professional code of conduct/ethics, who conducts the direction of research OR, more meaningfully, suborns their professional ethics because of pressure applied from ANY external or internal source and then publicly presents incomplete data in the manner of Ms Ramsey above, to deny independent scrutiny, that person is potentially in a whole world of trouble.
Ramsey is a Doctor and Consultant Epidemiologist, meaning that she may well have agreed to the standards of professional conduct for non clinical Doctors, eg the Royal Society of Medicine; it would be great to see her reaction to a proper journalist putting this point to her, Whitty, Vallance, van Tamm, Harries the whole rotten cabal.
“People who are fully vaccinated and people who are unvaccinated may behave differently, particularly with regard to social interactions.”
Ah, see there’s the problem right there. What needs to be done is obvious. We need to control the behaviour of the vaccinated, that will fix it.
Do you know, I thought exactly the same thing. And I also thought that would be the easy thing to do because the jabbed are ripe for control.
They are starting to mandate testing them again in Germany…
In any case, the actual behaviour is likely to be the opposite of what they imply – bedwetting Covidians who are terrified of the deadly virus will almost certainly have been spiked each time they were “offered” it, and follow all the other rituals of the cult, plus hiding behind the sofa as much as possible.
In contrast, people who thing it’s all a ridiculous over-reaction (like most of us on here) are far more likely to be unspiked,to ignore all the cult rituals, and to try to carry on as normally as is possible.
“The agency instead takes the view that the problem is systemic biases in the data which mean it “should not be used””
But if the data was favourable you can bet your house they would be promoting it as gold standard and the fact-checkers would be onto anybody daring to question it. These pathetic, mealy-mouthed bastards disgust me.
How long before the UKHSA denounces the UKHSA as heretics, and demands its replacement with a more Correct body (run by the same people of course, on more pay and expenses)?
This starts to remind me of Stalin and Kondratieff.
Maybe they made the same observation?
So, Steiner isn’t coming to relieve the Fuhrerbunker after all.
ooooh someone needs to make the video with UKHSA….
Watched “Dark Waters’ last week with Mark Ruffalo, lawyer, digging in to the Due Pont poisoning the people of West Virginia with their production of Teflon.
It’s a classic example of the corruption of government bodies working for a big corporate company. Du Pont knew all along they were poisoning people, but carried on nonetheless. Government agencies assisted in trying to stifle the truth, and if it hadn’t been for that lawyer, they’d have succeeded.
This feels like the same plot, only on a much, much, larger scale. But we already have enough data to know the vaccine drive has been an unmitigated disaster, but like in Dark Waters it may be a generation before anything is done.
Issues are:
People watch films like Dark Waters and say “Isn’t it crazy they did that?” “Wow.” “I can’t believe they got away with it for so long.”
When will they wake up!
Excellent post. I had forgotten that film, it’s a good while since I saw it., but you are spot on. I wonder whether Robert Bilott would take this one on… We could do with some legal types with the cojones to really go for this lot. Though they appear to be stymied at every turn.
Someone like this fine fellow…
I watched Dark Waters last week too, and its emotional impact on me was far greater than the last time I viewed it, some years ago. I thought of Union Carbide, and Bhopal, and wondered that there was seemingly no one to fight for the victims of that disaster, the legacy of which remains today.
Scientists get away with an awful lot, their propensity for evil seems limitless. They will kill us all in the end, one way or another.
Surely they should be rebranded again as The Ministry of Truth?
“the UKHSA has worked with the UK Statistics Authority to. . .”
There is a phrase that describes the practice of Police Officers ensuring that their notebooks all say the same when giving evidence in Court but I can’t recall it offhand.
The upshot is the vaccines are pointless – jabber woke y
What does it matter if they lie? They have been getting away with it since March 2020 – that’s 20 months already.
If you go to Heathrow Airport’s departures & arrivals boards you’ll see planes coming and going with passengers who have more than likely been ‘fully vaccinated’ as no-one wants to arrive and have to be in quarantine for 10 days with Mitie marshalls (Serco) checking up on them, and also having to pre-pay for two expensive PCR tests for Day 2 and Day 8.
Much easier to get the ‘vaccines’ and only have to pre-purchase an LFT kit from one of the Government’s ‘approved’ companies that flog them at huge profit.
There are people who say they’re not going to take the ‘vaccines’ and don’t want to travel abroad. A lot of these people are old people who weren’t going to go abroad anyway. Which is OK, as there are lots of nice things to see and do in the UK.
But these old people will be replaced by younger generations used to wearing face masks and getting ‘booster shots’ regularly. A child of 20 months of age is already used to seeing face masks on everyone in the shops. And not a single MP or member of SAGE have had their feathers ruffled, they have been comfortably collecting their salaries whilst orchestrating this mass hysteria.
My prediction is that by October 2023 things will be pretty much the same as they are now, and endless churning of statistics and figures, with hope for new vaccines, and another variant-of-concern thrown in for good measure. All a bit gloomy, but look around you – what changes have there really been in all this?
I think you may be overly pessimistic, perhaps based on the situation in your local area? Around me there is maybe 10% at most mask wearing indoors and those are mostly either elderly or single women in their 30’s (not sure why they feel particularly vulnerable).
Mask wearing percentages vary from place to place – where I live it’s around 100% in shops and on public transport.
I don’t think people wearing face masks at 10% in some supermarket near you is a ‘victory’ – we all know they’ll slap them back on in a jiffy when told to do so. As they did before.
What I do wonder about is we never hear how many school children have been ‘Covid vaccinated’ – some say this, some say that, but what is the truth? Most of them, or just a few?
Face mask wearing is still 100% inside airports and on planes.
We’ll have to see what happens with the 3rd ‘booster’ – how many have had that already, and how many will take it? When will the jabbing of the 5-11 year olds take place, and will anybody be stopping that from happening? Nobody stopped the 12-18 year olds being ‘vaccinated for Covid’.
I think I am more realistic than pessimistic. Based on what I have seen happen.
‘Face mask wearing is still 100% inside airports and on planes’.
Sadly, that is here to stay unless the air industry suffers in a severely financial way and even then they will probably not buckle. I doubt I’ll ever board a plane again.
Not in Norway, Swedn & Denmark.
Outside of healthcare the few people around here still wearing facemasks, welders shields even, would in normal times be regarded as social misfits or weirdos for the other ways they behave.
From my observations on mask wearing round me:
I was out and about as a key worker during lockdown proper (last spring/early summer).
As lockdown was partly lifted at the cost of wearing masks indoors it was the manual working men, many of whom had been also been working throughout, that were least likely to be wearing masks in Tesco Metro or the Co-op even though it was supposed to be compulsory; dunno about Waitrose or Sainsbury’s.
Same goes for the cafe I used to frequent, once it reopened, even Police Officers would come in for a cuppa unmasked.
Yep. How can you spot a Remain voter? They’re wearing a mask.
Not a good look – broadcasting your stupidity on the net.
Time was we had many Remainer readers here, more of a left/right balance and some self identified BAME people too.
In the States, same applies to the Dems! The die-hards are masked alone in the cars. Total idiots.
Yes indeed. All following the climate change scam too, and pro-mass-immigration. All liberals.
When I drive past my local M&S it looks like a scene from Contagion. A lot of other places I’ve been lately.. hotels, bars, cinemas, I’d say were below 10% now.
My 5cts:
SW London Waitrose 20% from the start.
Chichester Waitrose up to 75% again.
Sainsbury’s 50/50.
I’ve only been in M&S and Tesco recently, but during the normal working day they seem to support your ranking above.
Interestingly, in both cases the number of face-nappies in evidence seems to go down in both cases later in the day (after about 5) – presumably those who are most terrified / compliant don’t go out as much in the evenings!
Very likely to be true, same was the case during lockdown lite (last summer/early autumn) far more mask rebels in the evening.
Yes, Nick, you seem to have nailed it. Returned from a few days in East Devon yesterday. Sidmouth Waitrose, possibly 90+% maskers. Taunton Masks & Spencer definitely 80%. What broke my heart though was driving through Colyton when schools were emptying out. Virtually every single secondary school child fully face knickered OUTSIDE on their way home, presumably to Karen and Gary.
Sidmouth is bit of a special case, Gods Wating Room along with nearby Budleigh Salterton.
Colyton School is a Grammar where wealthy parents fight tooth and nail to get their offspring enrolled, might have thought they had more sense.
Taunton though is very run of the mill, rundown even, it’s surprising they can support an M&S.
Just like the Soviet Union when Comrades were forever being cajoled into yet more sacrifices for the golden future that was always nearly within their grasp.
Btw – i have travelled and continue to travel without this passport – most countries accept lateral flow tests and i can take a day 5 so called early release back in UK – it’s not what i want but it does not stop me and btw my kid’s teenage friends are dead set (no pun…) against this jab and well up on toxicity etc – take up is almost zero with them. Exceptions can become the rule. Quit the cynicism… whining etc. Resist and Act.
You can only take a 5-day ‘early release’ if you are ‘unvaccinated’ and have agreed to a 10 days quarantine upon your arrival, and have pre-purchased the Day 2 and Day 8 PCR tests.
The Day 5 ‘early release’ is also a PCR test, not LFT.
The ‘passport’ for now is required and must show, proof of being ‘fully vaccinated’, proof of recovering from Covid, proof of a negative test. I don’t know how anyone can be travelling without such ‘proof’.
You don’t say to which countries you have travelled. Would you care to enlighten us?
I certainly wouldn’t turn up at an airport without the required documentation, in the hope there’s a chance they’ll just let me through! And then miss my plane and have to go through the process all over again, buying new plane tickets, pre-purchasing tests, etc. – and where would I be staying in the meantime, sleeping on the airport floor, hoping I can find an electric socket so I can charge my phone?
The passport isn’t required o travel to Spain and back – I just show my test results and passenger locator form
Your ‘test results’ and the ‘passenger locator form’ are ‘the pass’. Anyway, that’s all rather vague. What test(s)? Where? How much time before the flights?
I’d suggest people do their own research rather than just turn up at an airport. For example:
https://www.spth.gob.es/more
https://www.gov.uk/guidance/travel-to-england-from-another-country-during-coronavirus-covid-19
Three minus ticks? Tell me what I have said that is not true! Still waiting for Ruth’s reply as to which countries she’s travelled to without any kind of Covid documentation…
I know for sure my paperwork was looked at when I flew from Helsinki, Heathrow and Amsterdam, and that I wouldn’t have even been allowed through security at those airports if my documents hadn’t been in order. I don’t like this, that you have to have ‘proof’ of Covid/vaccination status, but if you want to fly that’s how it is now.
My son has been travelling extensively this year (Turkey, Russia, Ukraine, Maldives) and has consistently refused vaccination; he did contract Covid last year (incidentally on a plane whilst fully masked) along with his friend who was sat next to him.
From the UK? And what happens upon his return to the UK? You haven’t said. Presumably he is required to pre-pay for PCR tests for Days 2 and 8, and be in quarantine for 10 days when he gets back to the UK.
Here’s the UK Gov site about ‘the rules’:
https://www.gov.uk/guidance/travel-to-england-from-another-country-during-coronavirus-covid-19
I agree almost entirely with you.
Air travel isn’t going back to what it was. Ever.
Measures and regulations are hard to turn back as it is. But to make matters worse, they’ve got themselves a climate change win by reducing the amount of air travel so the pressure to keep air travel volume low will remain.
Bureaucracies, airlines and the kind of people that travel a lot are generally the crowd that have swallowed all the covid bullshit whole – masks, jabs, lockdowns, social distancing, the lot. They are like the cool guys making and imposing the rules and will make everyone else jump through their miserable hoops.
Only that we are the kind of people who have been travelling a lot – four or five times/year to the UK – and we certainly didn’t want any of this ‘Covid nonsense’. However, we now have the choice – unvaccinated and 10 days quarantine plus two PCR tests pre-purchased from some cowboy company, or ‘fully vaccinated’ and only an LFT test required at a rip-off price.
My partner is ‘double-jabbed’. No noticeable side effects, still alive (I expect that if she were to die at the age of 95 some here would claim it was the ADE!). I remain unjabbed but it is becoming obvious that if I wish to travel to the UK without quarantine then I shall have to get the jabs – remember, they are 8 weeks apart minimum, so if I got the first on, say February 1st, I wouldn’t be able to travel until mid-April (8 weeks plus 2 weeks required for the ‘pass’ to become valid).
Even for the ‘fully vaxxed’ the EU certificate lasts only 12 months from the second dose… so it’s clear something must happen. My guess is the 3rd ‘booster’ will be required to keep the ‘pass’ valid.
Of course, I could remain ‘unjabbed’ for ‘The Cause’. I could also give all my money away to charities so they could help feed the starving children in Africa.
Difficult decisions!
I don’t know where you are but the Valneva (dead virus) vaccine, which is a French company, so bound to be available in France (though the UK have cancelled our order for deeply dubious reasons even though it’s going to be manufactured in Scotland; is that still the UK?). I suspect a lot of vaccine-hesitant people would accept this one, even though it still won’t have been through the full testing regime. I suspect, like many, I couldn’t give a toss how effective/ineffective it is, as someone who is ‘recovered’ I don’t feel under any risk & as someone who is in fine health I don’t feel at any risk anyway & totally in no need of any assistance from a vaccine of any sort.
Caution … one of the non-GM jabs causes pre-diabetes, according to recent findings.
So a choice … semi-permanent blood clotting or diabetes. Aaargh.
Well, semi-permanent if it depresses the immune system and you end up needing boosters for life.
I wouldn’t normally touch these ‘Covid vaccines’ with a barge pole either, but the fact is that for those who are deemed ‘fully vaxxed’ there’s no quarantine for them when they arrive in the UK, for the ‘unvaccinated’ 10 days quarantine awaits, plus obligatory pre-purchase of the Day 2 and Day 8 PCR tests.
Downtick all you like, but those aren’t the rules I made.
I don’t know how many arrivals take the chance of receiving a fine and break their quarantine. How do you answer when Serco phones up and says our man called round but you weren’t where you were supposed to be?
It’s no good when you get to the UK Border and they want to see your paperwork and you say “I read on the Daily Sceptics site that you don’t need any of that…” – and there’s a line of 200 people behind you tutting because you haven’t done as you should.
Finland I believe.
Yes. Which is why I’ve been keeping my eye on the international travel situation, especially in regard to the UK. I certainly wouldn’t just turn up at Helsinki airport without the documentation the UK Government demands, as I bet I would get no further than the Finnair check-in desk, or the check-in machine would ask for documentation codes.
I simply find it hard to believe people who come out with things like “I travel to Spain and back a lot and only have to show a negative test” – I mean, what does that mean? What test?
Then there are those who claim a fake screenshot of being ‘fully vaccinated’ will get you through – maybe it will, but who is going to risk all to see if it really works?
Millions of people all over the world unwittingly “risk all to see if it really works.”(The shot, that is.)
Catch covid and recover?
That certificate is good for 6 months. It’s a bit chancy booking a plane ticket and hoping you’re going to catch Covid and be on the path to recovery before the plane departs.
very iffy when recovering from actual COVID is vastly more protective than the clot shots
You have to catch ‘Covid’ first and I don’t seem to be able to find it anywhere!
As for ‘the vaccinated’ shedding ‘spike proteins’, my partner has been doubly-jabbed and I haven’t caught ‘Covid’ from her. Or… maybe I have and just didn’t know it? Asymptomatic like….!
The thing is, for those who want to travel to the UK and don’t want the hassle of 10 days quarantine plus having to pay for two PCR tests sold by shady characters, getting the ‘vaccines’ is the way to go. I’m not recommending this course of action, just saying that this is what people have been doing.
Take your chances and get the injections. I doubt anybody on here could really care less what you do.
Isn’t freedom of choice what we are all concerned and fighting for in our own small ways?
Absolutely, whether someone chooses to get vaccinated or not is entirely up to them, as is the reason they choose to do so.
My reason is not some anti-vaxx principle (although I’m starting to lean towards anti-vaxxing, as profit is clearly becoming more important than health). It never occurred to me I would need the vaxx, it was first supposed to be offered to the elderly and vulnerable and was not going to do much more than the flu shot. I am loathe to take any kind of medication without a genuine need.
Knowing more about the vaxxes now, I definitely do not want one as not only do I not believe there will be any benefit for my health, but worse there may well be some detriment to my health.
But should someone else decide otherwise, they should do what they think right. I have a somewhat more strident view of cooperating with the nassi pass, however.
“some anti-vaxx principle “
It’s a nonsense term, applicable to a small minority who are as religiously blind as any Covid fanatic – and a few who are looking to imitate Big Pharma and make a killing with other snake oil.
Jabbing is essentially the same as anything you ingest for your health – some interventions work, and others are a waste of time or even positively dangerous.
Whichever – it is an accepted ethical principle in medicine that it is your choice, after being full informed, whether you take the prescription. No ifs, no buts, and certainly not on the basis that the majority of the population are suffering from induced psychosis.
In the case of vaccines (in general), a few have undoubtedly had overall beneficial effects. But even those have had beneficial impacts that are historically a minor part of health improvement. What is also true is that ‘vaccines’ as a general category of pharmaceutical intervention have been massively oversold – for reasons thatare not hard to divine for someone with a functioning brain.
I tend to stick to the basics re. the snake-oil : simply that a novel experimental jab with little testing provenance is a very stupid thing to accept – especially with so many observational contra-indications that are consonant with theoretical predictions.
I was speaking hypothetically – we’ll have to see how this plays out, but I tend to believe that most people flying now have been ‘fully vaxxed’. There may be some who get a PCR test within 72 hours of the plane departure time, but that is tricky to arrange.
And very few travelling on the ‘recovering from ‘Covid’ certificate.
Not just planes, but ferries across the Channel too, and Eurostar.
9 minus ticks! Bizarre! I must have stepped on some tender toes…
You cannot lawfully be quarantined in then UK. This video may be of interest to you.
https://www.youtube.com/watch?app=desktop&v=hEgezGOeALk&feature=youtu.be
Yes – have bookmarked it and will look at it later, thanks.
Except for those with private jets, for whom it’s business as usual!
“My prediction is that by October 2023 things will be pretty much the same as they are now”
I think you could add 5 or 10 years to that date and still have a good chance of being right, sadly. There are only two things that will save us in the short to medium term. (1) Regime overreach causing a revolt. No sign of that in the UK. (2) People gradually tire of it all and it just fades into the background, and politically governments feel the need to move on because the public are no longer interested. The chances of this are slim I think, but it could happen.
if it turns shooty in the US, as it may well do, the impact will run globally
Alec Baldwin tried that but it didn’t catch on!
Globocap target date is 2030 so one way or the other the shitshow will continue for the next decade. As the C1984 nonsense wanes the planet toasting crap will be revved up. Either way my final year(s) are not going to be pleasant but the real horrors await the generations following.
God help them.
Yet they are going to make me chose between getting the jab or finding a new career which I suspect will involve me having to get a jab anyway, besides I’m not sure I can face another career change yet again. I guess it’s better to comply with these douchebags? I honestly don’t know what to do anymore. I just don’t understand why all my colleagues in the NHS are so compliant. Why do they accept to take orders from some wanker that worked at Goldman and Sacks before he got into politics. It’s not safe and it’s not effective.
Say no. If you say no, if we all say no, it ends.
Nothing is going to change. The New Normal. The New Nonsense. The New Nonscience. Build What Back Better you may ask?… consolidation of control. Why? Because they know the time is short. A controlled demolition is better for them than waiting for it to all fall apart.
This Government has systematically destroyed any belief or faith in politicians, the NHS, Doctors, journalism along with the Pharma Industry has destroyed faith in vaccines and medicines with their system of lies, cover ups, misrepresentation and bullying tactics.
May they reap what they sew
In the end, and for the historical record, the corporate scientists and their media lackeys will simply ‘revise away’ any evidence showing that there was no pandemic, the PCR results were not ‘cases’, the injections didnt work and caused millions of injuries and deaths just like their kindred spirits in the climate hoax are already doing with past temperature records. What we have witnessed over this last 18 months in terms of wholesale lying and blatant data manipulation are the formulative steps of that vast deception taking root.
Vaccine failures – now called breakthrough infections.
Vaccine failing – now called waning effectiveness.
It’s not just the figures/interpretations they massage. “Failures” and “failing” might wake up a few sheep you see.
It would indeed be very interesting to have some reliable data re the “breakthrough infection rate” experienced by never vaccinated people who have had covid, – ie pcr + clinical signs. In all probability though this has been done.
If I were a conspiracy theorist no doubt I’d be thinking there’s some sinister explanation for the figures not being released, like evidence based confirmation of the superiority of natural recovery from infection for example – which would upset the agenda.
Pushed into a corner they will say that even to contemplate such studies would lead to a lack of confidence in their product/vaccine/ultimate objective of digital control, and, that would never do.
There needs to be a study of people who think they had COVID before it was even named or identified. How many of these people (sick pre March 2020) later tested positive for COVID via a PCR test (once they were available)? If a smaller percentage than the population at large, this would be strong evidence of early spread. The evidence? These people apparently had natural immunity. (No such study will ever be done, which is kind of revealing imo).
Apologies for repeating my experience, but it remains relevant:
I’m certain I had covid in mid-October 2019 (Chinese students studying here were returning after the summer, and I was told about a mysterious respiratory ‘student virus’ at universities). I was really ill – anti-biotics and steroids didn’t touch it, and in December a scan showed ‘ground glass’ lesions on my right lung, and further examinations showed some damage to my heart. I still have these problems today, though not nearly as severe. Many times in early 2020 I told them at the hospital that I’m sure I’ve had covid and always they were dismissive, saying “oh, everybody thinks that” and ignored me.
By August 2020, fed up with these responses, I paid for a blood test at a local pharmacy, where I was found to have a full covid antibody count. I remain undiagnosed, however. My husband and son, who had both been ill at the same time (though not severely, and both recovered in a week or so) decided to get tested too, only to be told that the antibody tests had now been banned, going so far as to threaten pharmacies with closure if they didn’t comply.
At that point that I knew that ‘something was going on’; my family and I refuse vaccination, having done much research on-line, and know that we have naturally-acquired immunity from what is generally not a serious disease, though for a few, like me, it is more so. As it is, I consider myself lucky that covid didn’t become a ‘pandemic’ until I’d largely recovered, otherwise I’d probably have ended up in hospital, from where I believe I may have left in a box thanks to their early administrations.
Had there been a true, measured, unhysterical response to this virus, an honest government would have made antibody tests the norm; we would have seen how the disease progressed, who was vulnerable and who was not, the percentage of natural immunity in the population. Billions saved on PCR/lateral flow tests etc., (and fewer billionaires following Gates’ previous, oddly timely, advice to ‘invest in vaccines’, and making a killing). There was never a need for lockdown, etc., and the wholesale wrecking of peoples’ lives and livelihoods. Protecting the vulnerable would have been the priority while normal life went on as usual. Pretty much as was said in the Great Barrington Declaration, in fact.
As Hancock displayed, government was astonished and overjoyed at the ease with which the people capitulated to the monstrous new rules; within weeks we’d lost most of our civil rights and been controlled like never before in our entire history. They grabbed this unexpected opportunity with both hands, and a gullible people eagerly gave it to them.
Whatever happened to the people who were willing to fight, literally, to the death for freedom during WWII? The’ve been replaced by woolly-minded liberals.
They do have an out here and it’s to take the pharma companies to task for a product that doesn’t work and causes huge harms.
Oh, they’ve already made it in the contracts that if anyone takes them to Court over these vaccines the government has to pay for the defence costs of the pharma company.
Ah well.
A few points on this:
I’m going to put my observations to you, as you seem to have real knowledge of the technical side of things (I don’t know if you’ve said in the past that you have a background in this area; I’m going partly on your posts which I think are very informative and the name you’re using).
Does it strike you as odd that the colour-coded tables for VE, after having been only coloured green for high confidence as far as symptoms were concerned and pink, low confidence, for everything else for as long back as I can remember seeing this table, that this week all the other columns are now yellow coded, for medium confidence? Is there no need to explain why the change from one week to the next in terms of confidence level for every single column? I appreciate the claim is that there are more studies, greater certainty, but on what basis?
Have you seen the (I think) Chinese study regarding the Vero Cell vaccine which indicates immune suppression for at least 28 days after administering of the vaccine and other problems? If they have that study (it covers at least 90 days) for that vaccine, surely Pfizer and Modern now have similar studies for theirs?
Jane — thanks for that info on their summary table — I’d not been looking at it because it seems largely made up (and has done from the start).
Anyway, I had to laugh at it when I looked, because they’ve changed the colours but still have the same references. Ie, they’re changing their conclusions with the same input data and without explaining why (this is naughty is science/statistics).
But, as I say, they appear to be largely made up, so it is no surprise…
Re the Vero Cell vaccine study — I saw that too. I find it extraordinary that this research hasn’t been done on all of the vaccines. It is vitally important stuff, but they’re determined to vaccinate children anyway.
FWIW, I’d suggest that the problem isn’t the specifics of the vaccines, but what they’re doing — I believe that this is an autoimmune problem caused by anti-covid-spike-protein antibodies (rather than the spike protein itself). Thus I fear that there is a substantial risk of the problems identified in the paper being present for all of the vaccines. I’d also note that the Vero Cell paper’s data was based on rather small numbers of people — ordinarily this would be an issue (too few to make reasonable inferences), but in this case the effects are profound and appear to be seen in pretty-much everyone — this is very concerning.
Thanks for the reply.
I know the VC study was on a small group, but even to a layperson (it was very technical), the indication that the vaccine was causing unforeseen negatives seemed pretty clear. It might be extraordinary that the other vaxx makers have not carried out such a study – the cynic/realist in me says they do have precisely such studies, have had them for months and they are tucked away gathering dust.
The reason is clear – as you say, the problem is probably the same for ALL the vaccines, because the problem is the antibody response to the spike protein, something I’ve been reading about since February/March. A lot of accessible info was available on that on Childrens Health Defense, an excellent site for people who are not yet familiar with it.
Some months ago there was a small article in a Dutch newspaper about research at the University of Amsterdam. I found a very technical article about the research (in English). The researchers had found an existing drug that regulated the immune response to the covid spike protein, without suppressing the entire immune system, as steroids do. The research indicated that the people who had excessive immune reaction appeared to do so after becoming sero-positive with anti-spike antibodies. I believe their conclusion (or implication, not sure) was that it was the anti-spike antibodies that were the problem.
The infection window post infection was demonstrated in care homes infection data way back in March. It’s WHY they have changed the definition of a vaccinated person to cut out the first 21 days post jab.
I’m not necessarily referring to infection risk. The study in question showed other harm in relation to diabetes, kidney, coagulation. I think those things might be what appeared over the 90 day period. It’s worth having a look at the study itself. TheyLiveandWeLockdown posted a link to it in a comment under the Merkel article yesterday.
Nature article I’ve posted elsewhere, the jab harms your immune system (and causes diabetes like symptoms including raised HBA1C which FUBARS healing).
amanuensis do you want to write something about vaccine effectiveness above the line? Seems like you have some mastery of the field. If so, email me at lockdownsceptics@gmail.com. Some goes for other peeps below the line. If you think you have something interesting and original to say, email me at that address.
Good for you Toby.
Nice one.
I run these numbers every week, graph them and make my own conclusions.
Fancy a look?
Continued
Continued
Continued
Continued
Continued
I can’t read them, type too small!
Click on them. Click on the black background to return.
Yes, I understand that! But still too small, fewer charts per page would help.
Magnifies OK on my tablet, sorry you can’t read them.
Try right clicking and “open in new tab”. Then click on the chart to magnify
I’ve struggled to read these & so think I’m not getting all I should from them due to different scales etc. Could you do a little analysis of say, the 60-69 year olds highlighting what’s interesting? Thanks.
Geert Vanden Bosch is calling it folks. Choppy waters ahead?
https://stevekirsch.substack.com/p/what-happens-if-israel-fails-the?r=o7iqo&utm_campaign=post&utm_medium=web&utm_source=
This chart shows the week on week change in the likelihood of vaccinated v unvaccinated people testing positive for covid over the past 2 months or so.
In each of the age groups between 40 & 80 the vaccinated are more than 100% as likely to test positive. But, as Will notes above, regardless of the veracity of the population data the trend is clear & all one way.
The only justification Whitty & Co came up with for jabbing healthy kids was to stop onward infection. Well, clearly, it doesn’t do that so where’s the justification.
The only justification for vaccine passports is the conviction that unvaxxed people are more likely to pass the virus on than vaxxed people. Well, clearly, that’s not true.
We live in strange times.
Yes this TREND CLEARLY SHOWS that the jabbed are catching it more than unjabbed. This is proof, not correlation
I’ve posted later to point out that UKHSA have changed how they calculate the rates per 100,000 in the double vaccinated and unvaccinated.
In week 43 they used the NIMS population at week 42 and in this week’s (week 44) report they’ve used the NIMMS population at week 41. That is they’ve jumped back 2 weeks.
You might want to adjust your chart for next week accordingly.
Very sneaky!
I can’t think how I’d do that, as I haven’t got the relative NIMS numbers or the absolute numbers in the vaxxed or unvaxxed categories.
Good find though.
The numbers of ‘cases’ are in the spreadsheet attaching to National Flu and covid surveillance reports.
While I don’t like UKHSA chopping and changing I don’t think their changing of the population distorts things too much having looked at it.
You can get single dose numbers in that spreadsheet too.
We are actually quite close to negative efficacy in every age group when you do a straight comparison between vaccinated (one or more doses) vs unvaccinated.
The under 18 age group is misleading as there are so few double jabbed. When you include single jabbed there’s actually negative efficacy there also according to my calculations.
The surest way to refute the claims is to publish up-to-date figures. The absence of current infection rates being published surely tells us all we need to know.
As far as bias is concerned, one could equally say that it is likely that vaxxed are being significantly undercounted as many vaxxed people will not bother getting tested – as they’re ‘safe’.
The nassi pass in NL allows a vaxxed person to get a positive corona test and still go around coughing and sneezing over everyone whenever and wherever they want. They are, of course, being requested not to, but the government has clearly stated it will not modify the nassi pass so that anyone who gets a positive test will not get a QR code, even though virologists and doctors have asked them to do that. I have a vaxxed neighbour who said if he gets symptoms he won’t get tested, because he wouldn’t go out if he knew he had corona – don’t test, don’t know, clear conscience.
They’re rerunning an old ad saying to get tested if you have symptoms, with the addition of “even if you’ve been vaccinated”. They have had bulletins on the news imploring people who are double vaxxed to get tested if they have symptoms, which implies they are quite concerned that vaxxed people are not getting tested (understandably, what was the point of the vaxx otherwise).
I’ve been working at a site where there are rather a few with persistent hacking coughs. None have put themselves up for testing, because ‘they’re vaccinated and thus it won’t be covid’.
Most people are quite shocked to discover the jabs do nothing to stop you catching or spreading SARS2.
Just wait until it sinks in that it probably does little to nothing to stop you from getting ill or dying…
And then we haven’t even got onto the fact that the vaxx may make you more susceptible to catching corona. And then there are of course the long-term unknowns…
Are any Astra Zeneca jabs still being given?
Only to people they catch posting ‘misinformation’ about the vaccines online.
The Emperor has no clothes!
Everything in the UKHSA blog post is rational, but I note they give no estimates for the magnitude of these differences between the two groups, and like Will i cannot see at this point in the fear cycle that these difference can be major – a percent maybe, not a hundred percent.
But, if UKHSA is happy to tell me I’m healthier, more aware of risk, more likely to have lived my life normally, less likely to have been fearful and mask bound, and more likely to be enjoying the open air rather than hiding in my house, yes, they are right. And it’s great that they acknowledge all of this means I’m less likely to be ill, less likely to be infected at this moment and also less likely to NEED A FUCKING VACCINE.
We see it all around us, it is the vaxxed who are ill, the vaxxed how are cowering, the vaxxed who are infecting others. And they want to assimilate us too? Go fuck yourselves UK Govt.
Because it’s not good for business, is it!
The weekly tables showing cases/hospitalisations/deaths in the vaccinated vs the unvaccinated is useful, but is there data breaking this down further than just vaccinated and unvaccinated?
Presumably the definition of unvaccinated is something along the lines of any person who has not had a second dose more than 14 days ago. That would include people who have had one dose, as well as those who have had their second dose less than 14 days ago – both categories of people for whom the rates are highly relevant. If those groups have a higher rate than those who have’t undergone any gene therapy, then they are artificially bumping up the rate in the unvaccinated, and making the (already bad) effectiveness rates look better than they actually are.
It’s even worse – the 14 day gap wasn’t enough, they have now pushed it to 21 days. You can have been jabbed 20 days ago, get ill, die, and you will go down on the stats as unvaccinated.
This is rolling 4 week data, so after next weeks update, we will be able to explicitly compare case rate data for 3 completely separate 4 week periods running weeks 33-36, 37-40 and 41-44 respectively.
If you look at just the double vacc data and non vacc data standalone purely for trend analysis using the 40-43 week data in the meantime (excluding under 18s), the difference in trends, irrespective of relative case rates between the 2 is striking
Un-Vaccinated
The latest report continues to say
Since the report gives those rates broken down by age, which shows that for most adult age groups the rate in the vaccinated is much higher than in the unvaccinated, it is perfectly reasonable to compare them. The report itself does, for it declares
That is a comparison: the rate in one cohort is higher than the rate in another cohort.
These rates give us a reasonable indication of the rate of infection in groups. If I am among a large group of vaccinated people in their 40s then more people in that group would likely test positive than if they were all unvaccinated. Or to put it another way, the more in the group who are vaccinated, the higher the rate of test positives around me there will be.
It also means that if I draw a sample, including an individual, from most adult age groups then the higher the vaccination rate in the group, the higher the probability of selecting a person who would test positive. To minimize the chance of selecting a person who would test positive one should draw from groups who are wholly unvaccinated.
It certainly says a great deal about the nonsense of vaccine mandates for employees: if the pool is wholly vaccinated then the likelihood of a test positive is maximized.
So we don’t have to make the case by arguing ‘vaccine effectiveness’, whereupon our detractors will argue the case for bias. The raw data, the rates themselves, fatally undermine the basis for vaccine passports, vaccine mandates for employees, and restricting access of those who are unvaccinated.
One continuing problem is the lack of rigour associated with the terms ‘cases’, ‘infections’ ‘disease’ etc.
The elasticity undermines any data that is derived.
This is totally unacceptable. The UK government are clearly intending to mandate vaccination for certain workers while also introducing a vaccine passport.
The only justification for doing this would be if the unvaccinated posed a significantly greater risk to the general population than the vaccinated. Yet – the very metric which would confirm this, i.e. VE against infection, is being withheld and the only data released to the public is claimed to be misleading.
So the VAERS data in the US is misleading, Yellow Card data is misleading, UKHSA data is misleading and, presumably, the data previously released by PHE was misleading.
Is there any data which isn’t misleading?
I do believe that Pfizer’s financial and shareholders’ reports are spot on, if that helps
All cause mortality.
You’re either dead or you aint.
Yes – that’s about it.
But then, you are still ham-strung in defining groups that you may be interested in comparing – even down to the most basic number of all – those dying from Covid.
Also, many of those mortality charts – the so-called baselines – are based on “expected mortality.” Change the expected number, you change everything else.
I imagine there is plenty of data that isn’t misleading but, funnily enough, it hasn’t seen the light of day. One can only speculate as to why that might be the case, but I very much doubt if it is because the data highlights positive vaccine efficacy.
Yeah, those of us who have still (at the point when it’s almost certainly a choice) not taken a shot probably are the same people who are cowering in their houses…
¯\_(ツ)_/¯
‘Yet again I had to draw this graph myself, and yet again, the UK Health Security Agency wants you to know that these rates are extremely, totally, absolutely unadjusted. They just don’t know precisely why or how.
‘As I noted on Twitter, it’s emerged that UKHSA inserted all of their ill-advised disclaimers after coming under fire from the Office of Statistics Regulation, a regulatory body which periodically complains about statistics published by the British government.
‘OSR director Ed Humpherson met with UKHSA hours before they published their Week 43 report, demanding they do something about these awkward graphs. They responded by ditching the graphs altogether and calling every last number unadjusted. This failed to satisfy him, so in the days afterwards he issued this fairly unbelievable open letter.’
https://eugyppius.substack.com/p/ukhsa-efficacy-stats-death-watch
The blatant bias in ferreting out data problems is amazing in its transparency.
Suddenly, such problems are a bone of official contention in one area where the wishful thinking of the Narrative doesn’t stack up.
In fact, we have, of course, known about this problem right from the get-go, since experimental data had shown that absolute risk reduction was minimal. Of course that contradiction of relative risk reduction was never highlighted.
… and meanwhile, such major absurdities as the use of uncontextualized PCR+ results, the 28-day window on test results to determine ‘cases’ and the unverified counting of death from – or with – any general respiratory infection as ‘Covid’ – all these continue unchallenged as valid ‘science’.
The agency instead takes the view that the problem is systemic biases in the data which mean it “should not be used” to estimate vaccine effectiveness
That’s a bit misleading. The agency also accepts that the use of NIMS can lead to an overestimate of the population and therefore an underestimate of the infection rate for the unvaccinated, especially in younger age groups:
One of the basic problems with NIMS is that it contains some people who were registered with the NHS but may have moved – for example overseas – but these people have not yet been removed from the database – these are often called “ghosts”. Because vaccine uptake has been so high, even a small number of additional people included in the database will inflate the number recorded as unvaccinated – so this makes the rate of COVID-19 cases in some of the younger unvaccinated groups appear lower than it should be.
Keep clutching at straws. The amusing thing is that this isn’t even news. The crowd all know the emperor hasn’t any clothes on. The vaccines don’t stop infection or transmission and the outcomes are worsening as vitamin D levels drop. The authorities know this, which is why they haven’t released any of their vaccine effectiveness surveys, for six months.
Fortunately it looks like endemic equilibrium has been reached in the vaccinated population, it was achieved in the unvaccinated months ago, as Spector highlighted before he was spiked.
The situation in Europe doesn’t look so clever and their wave of infection in the vaccinated is coincidental with falling vitamin D levels; vitamin D levels which could, just as easily, have mitigated outcomes over the summer. Anyway, at least they have the fig leaf of vaccine mandates and masks to cover the emperor’s imminent embarrassment!!!
UKHSA have made a sneaky change to how they calculate the figures that I can’t see anybody else has noticed.
In week 43’s report (which covers weeks 39-42 they used the populations of unvaccinated/vaccinated from NIMS as at week 42 for the denominator used in calculating ‘case’ rates in the unvaccinated and vaccinated
However in this weeks week 44 report (which covers weeks 39-43) they use the populations of unvaccinated/vaccinated from NIMS as at week 41 for the denominator used in calculating ‘case’ rates in the unvaccinated and vaccinated.
That is they’ve jumped back 2 weeks in terms of the population denominators.
You can see this numerically if you are calculating the rates per 100,000 yourself from the population and ‘case’ data but notice also how the report wording has changed
In the week 43 report they say
The rate of COVID-19 cases, hospitalisation, and deaths in fully vaccinated and unvaccinated groups was calculated using vaccine coverage data for each age group extracted from the National Immunisation Management Service
But in week 44 there is a subtle change to add in mid-point
The rate of COVID-19 cases, hospitalisation, and deaths in fully vaccinated and unvaccinated groups was calculated using vaccine coverage data for each age group extracted at the mid-point of the reporting period from the National Immunisation Management Service
It also means that the double vaccinated under 18 group used in their calculations has gone from about 240,000 to 140,000 and back to to 240,000 in successive weeks. And probably will jump back to 240,000 next week! Again something they’ve sneaked in.
I don’t diasagree that using the mid-point is better, but they should have made it clearer that they were changing especially as they say the figures are useful to look at trends.
Just in case anybody else is looking at it.
The above applies to the unvaccinated numbers now being based on week 41 was 42 the previous week..
However the double vaccinated numbers now seem to be based on week 40. The week 40 figures were updated around week 43 but it’s the old figures it appears that they are using.
All very odd, unclear and opaque.
Finally fully worked out which population they use for each weeks figures (not easy as you have to work back) in the vaccine surveillance reports.
So instead of using week 43 figures this week by using the population at the end of the 4 week period being considered as they have been doing, they’ve gone back to week 40 which they call mid-period. I’m not sure it makes that much difference.
It’s the same for vaccinated and unvaccinated so ignore my previous bit bit about it being different.
Week 44 (covering weeks 40-43) is based on the week 40 from the up to week 40 spreadsheet
Week 43 (covering weeks 39-42) is based on the week 42 from the up to week 42 spreadsheet
Week 42 (covering weeks 38-41) is based on the week 40 from the up to week 40 spreadsheet
Week 41 (covering weeks 37-40) is based on the week 40 from the up to week 40 spreadsheet
Week 40 (covering weeks 36-39) is based on the week 39 from the up to week 39 spreadsheet
Week 39 (covering weeks 35-38) is based on the week 38 from the up to week 38 spreadsheet
Week 38 (covering weeks 34-37) is based on the week 37 from the up to week 37 spreadsheet
Week 37 (covering weeks 33-36) is based on the week 36 from the up to week 36 spreadsheet
Week 36 (covering weeks 32-35) is based on the week 35 from the up to week 35 spreadsheet
Note the up to week x spreadsheet is found in the figure 62 sheet ‘covid vax uptake’ of the week x+1 excel spreadsheet. By up to x, I mean the population figures go up to week x. Note there was no ‘up to week 41’ spreadsheet which is why both week 41 and week 42 figures used the week 40 figures and why the latest week uses week 40 rather than week 41 as the mid-point. Next week should be based on week 42 from the up to week 42 spreadsheet I think.
This is hard to watch/comprehend:
FUNERAL DIRECTOR: I JUST SEE THE DEAD BABIES IN THE FRIDGES
https://www.bitchute.com/video/ZwWN2QS0SPV9/
I appreciate Will’s research and commentaries on this topic. He is actually serving a journalist’s most important role as a “watchdog” of authorities and government officials. He is digging deep into the data and is not afraid to question it or ask for more relevant data. He points out where the data is probably intentionally misleading (for example, by using statistics from back in the months when the Alpha Variant was the dominant strain).
Needless to say, there is not ONE journalists from a big corporate news organization who is doing the analysis he is doing. This FACT is quite scary when you think about it.
They test for the flu since they’ve never isolated Covid-19. Which makes me wonder how they can tell there is a delta variant. They never isolated the virus but they use a test to show the damage of a solution does on monkey kidney cells then show the cellular debris as proof of the virus. So, they can use this method to claim an UNENDING! amount of variants. A lot of cancers and “viruses” are probably just different forms of parasites. Since the tests can’t differentiate between cold and flu and covid then doesn’t that mean ivermectin cures both the cold and the flu? Welcome to “they’ve been lying to us our entire lives about everything”. Get your Ivermectin while you still can! https://health.p0l.org
So why are unvaccinated people not having their human rights not restored worldwide, the same as vaccinated people?
because it is not part of the plan to introduce vaccine passports that will turn into digital passports that will control your whole life. Imagine all over 50s being instructed to take statins or you can only access your bank account if you behaved well.
Initially vaccine passports were labeled as a conspiracy and now it is being introduced all over the world
Please can anyone explain the stats showing that the jabbed are anywhere between 55% and 99% protected from hospitalisation and death as these are the figures that my jabbed friends and family throw at me?
The UKHSA data about infection rates completely destroys any arguments that could possibly be made in favour of vaccine passports. If people want to believe in fairies that is their lookout. If the vaccines don’t stop infections or infectiousness then choosing to take them is a personal decision; it makes no difference to anyone else so it is no one else’s business.
The vaccine passports have nothing to do with health and transmission. they are about control and preparation for the global ID system which at that point will control every aspect of your life and will have the ability to cut you off from even your own assets if you don’t “behave”.
The “fake data” you refer to is normally created by cherry-picking the time period. Most of the data designed to reinforce the official narrative uses data that starts in Jan 2021, when almost nobody was vaccinated so all (100%) of hospitalisations and deaths were in the unvaccinated. That remained the same (see below) until May and included the large “hump”. After then, we were in the Spring and Summer period when “cases” disappeared as the numbers of “vaccinated” increased so creating a double bias in the data.
The other enormous misuse of data concerns the definition of “vaccinated” as being second dose + 14/21 days. Most hospitalisations and deaths from the vaccines occur within that window (which is why this definition of “vaccinated” is used). They want to pretend that anyone “Vaccinated” (Second shot + 21 days) somehow doesn’t have to come through the window before achieving that status.
How to lie with statistics is becoming an art form with Covid data and you need to be very careful. Question everything!!
It’s an interesting question.
Any efficacy (and on the surface at least there appears to be some limited efficacy against hospitalisation and death from these UKHSA tables) is against your hospitalisation or death being labelled as covid
But the real metric to look at is does the vaccine prevent your hospitalisation or death (regardless of whether that hospitalisation or death comes with a recorded positive test).
If you seek medical help for serious complications of diabetes are hospitalised and subsequently die of those complications, then any positive test for covid is incidental in that hospitalisation and death, They are either finding ways to record unvaccinated deaths as covid or the vaccine is preventing the positive test but not addressing the real cause of illness that results in the death. In the USA they are using different cycle thresholds for the PCR test for vaccinated and unvaccinated, some other trick might be in play here in the UK.
Let me show you a chart from this ONS publication for the age 60-69 age group to explain how the data suggests this is happening.
What the chart shows are all cause deaths (the solid red and green lines for the vaccinated and unvaccinated respectively) and covid labelled deaths (the red and green dotted lines for the vaccinated and unvaccinated respectively).
The solid blue line is all cause deaths across all groups. The blue line starts at the green line because at the start nobody has been vaccinated and ends up nearly at the red line once most of the age group have been vaccinated.
All these are death rates per 100,000 in each category.
Don’t get too concerned about the green line being above the red line at 24th September 2021 it’s probably an underestimate by the ONS of the proportion unvaccinated not a real affect, although it could be the unvaccinated are an unhealthier group than the vaccinated. But it doesn’t affect the overall shape of the curve.
If you look at the solid blue line first you see that the experimental vaccination started after covid labelled deaths had peaked around 29th January. And you see the dotted red and green lines representing covid labelled deaths in the unvaccinated and vaccinated fall away after about 29th January.
There are some end of life people or people who are seriously ill in hospital who are too ill to get vaccinated. As healthy people get vaccinated that pushes those seriously ill people to be a disproportionate part of the unvaccinated proportion. And the vaccinated people are disproportionately healthy compared to the age group as a whole because the healthy self select out of the population to be vaccinated, and so the vaccinated group doesn”t contain any of the ill people who can’t get vaccinated.
That is my theory for the peak of the death rate per 100,000 at 2nd April 2021 for the unvaccinated (green line). Note that the rise up to that peak happens after covid labelled deaths in the unvaccinated (the dotted green line) has started to fall, so it tells you that hump is not in any way related to covid.
By 18th June the green line (the unvaccinated) has fallen completely from its peak as the end of life people who couldn’t get vaccinated have died and those in hospital have either died or recovered and have then been vaccinated.
Because numbers in the unvaccinated group are quite small after all who have chosen to get vaccinated have been vaccinated, the green line (unvaccinated) wiggles about a bit. However note that covid labelled deaths in the unvaccinated (the dotted green) line goes up around 16th July. But the solid green line to 24th September after some wobbles stays at the same death rate as at 18th June.
What this is showing is that the increase in covid labelled deaths in the unvaccinated is not following through into extra all cause deaths. So these covid labelled deaths are deaths from other causes mis-labelled. Note also how the red and green solid lines are roughly running level (if you even out the wobbles in the green line due to small numbers) even though there is no corresponding increase after 16th July in covid labelled deaths in the vaccinated.
So what this data is tentatively indicating is that any apparent efficacy of the vaccine in preventing a covid labelled death is only in preventing the death being labelled as covid, And there is no efficacy in preventing the death itself. So if you are unlucky enough to die the vaccine may stop your death being labelled as covid but it doesn’t stop you dying.
Why this is happening is unclear. It may be that there is some bias going on in recording death. Or it may be a positive test is incidental to the person’s hospitalisation and death.
Given the low absolute risk of dying from covid and all the adverse affects of the vaccines that we are reading about, it doesn’t make any sense to get vaccinated for illusory benefits and real harms.
We know the infection rate in vaxxed is vastly greater than the unvaxxed. See Dr Mercola’s newsletter this morning. Doesn’t look good for the vaxxed in the UsA this winter.
any chance of having Joel Smalley as a regular writer on lockdown sceptic?
Great article indeed:
Dr. Robert Malone: International COVID Summit
https://articles.mercola.com/sites/articles/archive/2021/11/06/international-covid-summit.aspx
Hope you don’t mind me sharing my experience? I had covid in March 2020, I picked it up at the Cheltenham Gold Cup festival or, more accurately, my wife did and very kindly shared it with me. I was feeling pretty rough for around two weeks, it felt much like the flu.
I have not been vaccinated as my doctor (off the record of course) thought it would probably be detrimental as I have already had the virus.
At the beginning of August we were out to dinner one evening in a very small enclosed “pod”, myself and five others. As the evening wore on I could feel, what I thought, was a cold coming on, the next morning I felt rough and suspected that I had covid again. I used one of the tests we keep around for work purposes and it showed positive (I’ve taken these tests many times before and always negative). Anyway, I felt rough all day and into the next morning but by lunchtime I felt much better and by the evening I felt fine again. I took another test a couple of days later for work and was still showing as positive even though I felt fine! No one else in the “pod” that evening became infected and only one had been jabbed.
Draw your own conclusions.
Yes, it’s obvious that Government is not happy that this data is even available. In the US it isn’t – a decision was made not to maintain data by vaccinated/unvaccinated categories, making for a much happier CDC.
The problem with all of the data is a) it is all for “Covid” cases and events which is subject to manipulation (PCR? Deaths WITH Covid etc) and b) the definition of “vaccianted” is second shot + 14 days, which now seems to be increasing to 21 days.
In fact this approach hugely slants hospitalisations and deaths towards the “unvaccinated” because the vast majority of these happen after the FIRST injection and before 21 days after the second injection. If this period is re-defined as “Partially vaccinated” and separated from “unvaccinated” the picture looks very different. IMHO this is also a deliberate, in fact THE most deliberate, manipulation of the data.
The only way to look at the real picture is to use TOTAL mortality (much more difficult to manipulate) and for all parameters divide the data into the above 3 groupd NOT just 2 groups as at present.
These points have been very eloquently made by Prof Fenton who has, for his trouble, received the same treatment as the eminent Physicians who have dared to question the official narrative in the name of real science.
The only good thing to say is that it’s getting harder for them to hide the truth.
Well done to Will for his efforts, describing these UKHSA vaccine surveillance report figures and fighting back against the nonsense criticisms to his very balanced stuff with clear explanations.
However one bit I would quibble with is the line when talking about efficacy against testing positive where the article says
Vaccine effectiveness …………………….remains high for under-18s,
I don’t agree with that at all.
Firstly there are very few under 18s who have been double vaccinated.
The UKHSA reduced their under 18 double vaccinated numbers abruptly from about 240K to about 140K a few weeks ago. So something clearly massively wrong with those double vaccinated numbers for such a change to happen. The UKHSA sneaked that correction in without any explanation.
But the figures for week 44 are based on about 236K double jabbed, because UKHSA are basing their figures on old population estimates before their correction was made. So the positive test rate per 100,000 is clearly understated even on their current wonky estimates.
It’s clear UKHSA haven’t been recording an accurate record of double jabbed under 18s and the positive test rate per 100,000 can’t be reliable as a result in any case. Will they halve numbers again in the future when they find other errors?
In addition there are about 140K double jabbed under 18s but 890K single jabbed under 18s (based on week 44 figures) so the double jabbed are much smaller in number than the single jabbed.
And the positive test rate in the single jabbed under 18s per 100,000 is 40% higher than the unvaccinated under 18s rate.
We need to wait for things to stabilise because the figures are dependent on which week’s numbers are used and single jabbed numbers are changing rapidly.
But that caveat aside if we compare vaccinated (any dose) with unvaccinated the experimental vaccine has about negative 13% efficacy against testing positive currently
So there isn’t high effectiveness more like none at all in the under 18s.