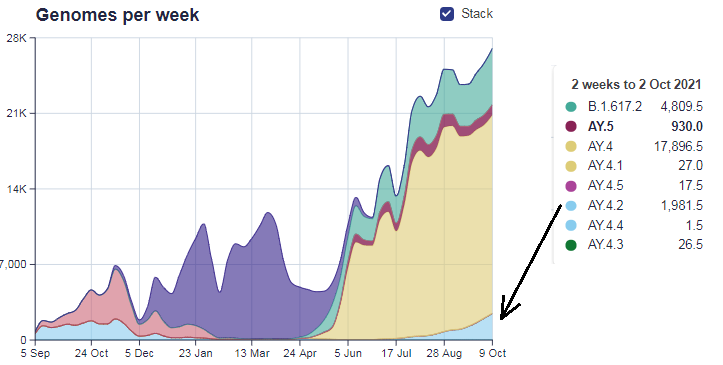
There’s a new variant in town. Or rather, a sub-variant – AY.4.2, an offshoot of the Delta variant, said by some scientists to be up to 10-15% more transmissible. As of the end of September it made up around 6% of new cases and is on an upward trajectory.
However, there’s no reason to panic – and, for a change, that’s the message coming from the top. The Prime Minister’s official spokesman said: “There’s no evidence to suggest that this variant… the AY.4.2 one… is more easily spread. There’s no evidence for that…”
Francois Balloux, Director of the University College London Genetics Institute, said while the variant is “likely to be up to 10% more transmissible”, it is not comparable to Delta when it arrived in the U.K, which was at least 50% more infectious than Alpha.
Professor Balloux played down the likely impact of the increased transmissibility on infections, adding:
Here we are dealing with a potential small increase in transmissibility that would not have a comparable impact on the pandemic… As AY.4.2 is still at fairly low frequency, a 10% increase in its transmissibility could have caused only a small number of additional cases. As such, it hasn’t been driving the recent increase in case numbers in the U.K.
AY.4.2 is not yet classed as a variant of concern, although it is being monitored by the U.K. Health Security Agency (the successor body to Public Health England) and “is likely to be elevated to the rank of ‘variant under investigation'”, Prof Balloux thinks.
It’s certainly good to hear the absence of panic. Professor Balloux is right to point out that a 10% increase in transmissibility is unlikely to make a noticeable impact on the spread. Technical Briefing 24 from UKHSA includes a graph showing the secondary attack rate (SAR, the proportion of contacts an infected person infects) of different variants over time. Splitting them into household and non-household contacts, it shows that Delta has hovered around the 10% mark for household SAR (and 5% for non-household SAR) since June. That means around 90% of people who live with an infected person do not become infected themselves (or rather, 90% of people who live with someone who is PCR-positive do not themselves report being PCR-positive).
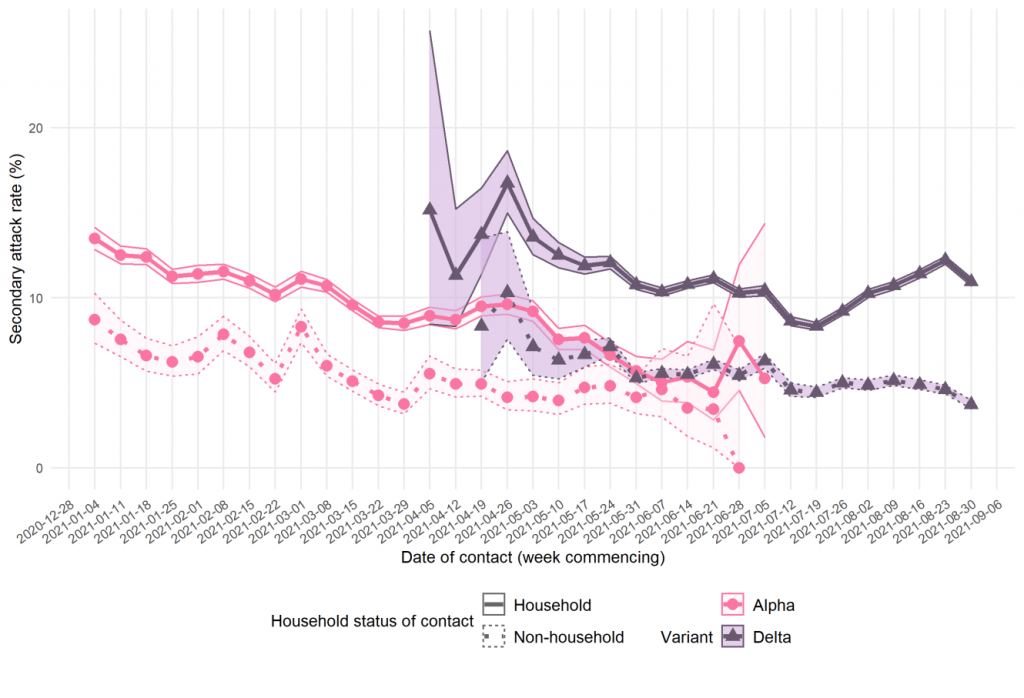
A 10% increase in transmissibility would therefore equate to a household SAR of just 11% and a non-household SAR of 5.5%. That’s hardly going to make any difference, particularly as the SAR varies over time anyway.
As to the claim, repeated by Professor Balloux, that Delta is 50% more infectious than Alpha, it can’t be stressed often enough that this only holds when Delta first registered as a variant of concern in the spring (see graph above). At that point Alpha’s SAR had already declined (presumably due to variant-specific herd immunity and a change of season). The earliest reliable values for Delta household SAR put it around 14%. That is below the 15.5% direct-contact SAR recorded for Alpha using data up to December 20th 2020 in Technical Briefing 3, showing the two variants were comparable at their peak, with Alpha possibly having the edge (aided by winter). In the same briefing, Alpha is reported to be infecting 10-70% more contacts than the other (non-Alpha) strains around at the time. Again though, this is comparing the old variants which are in decline with the new variant which is surging. We don’t have SAR data for the original spring wave, but looking at the steep gradient on the infection curve in March 2020 we can be confident it was no lower than Alpha’s in December.
AY.4.2, on the other hand, is not currently showing any of this new-variant zing for infectiousness. In Denmark it reached a 2% frequency but then decreased. Until we see that change, it isn’t anything to get excited about.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Professor Balloux. It’s like reality is trying to tell us something. Can’t think what.
😉Nice one reality.
https://s.w.org/images/core/emoji/13.1.0/svg/1f388.svgFriday 22nd October 11am https://s.w.org/images/core/emoji/13.1.0/svg/1f388.svg
Yellow Boards Event – Stand by the Road
Tesco Superstore
17 County Ln, Warfield, Bracknell RG42 3JP
Wokingham https://s.w.org/images/core/emoji/13.1.0/svg/2764.svg Stand in the Park https://s.w.org/images/core/emoji/13.1.0/svg/2764.svg Sundays 10am
Make friends – keep sane – talk freedom and have a laugh
Howard Palmer Gardens RG40 2HD
behind the Cockpit Path car park in the centre of the town
Telegram http://t.me/astandintheparkbracknell
Variants lies and damned lies
Friday 22nd October 11am
Yellow Boards Event – Stand by the Road
Tesco Superstore
17 County Ln, Warfield, Bracknell RG42 3JP
Wokingham Stand in the Park Sundays 10am
Make friends – keep sane – talk freedom and have a laugh
Howard Palmer Gardens RG40 2HD
behind the Cockpit Path car park in the centre of the town
Telegram http://t.me/astandintheparkbracknell
I see that there are also some small demonstrations outside the Commons – just two or three concerned women with placards when I passed.
Indeed. An unfortunate name for a man who relies on not being accused of talking something that is often written with the same first and last letters.
One could also accurately modify his first statement to ‘There is no evidence that lockdowns worked’, but that would never make it through the reality-filters applied by the MSM for their Fear Porn project.
Reality? I’ve forgotten what that is. Maybe we need a cross-party Parliamentary group to issue a report on it. I’m sure it would help us better understand this reality of which you speak. Now, back to my “Be Boris VR game to see how many kids I can father and promises make.”
Professor Bollocks is playing good cop.
Meaningless drivel for a coronavirus with a 99.6% survival rate.
Watch the pea.
Francois Balloux – known to his mates as Frankie Bollocks.
Another scariant was inbound so this one is right on schedule
Why no discussion among the officially-approved experts of how infectious this and other variants are compared with the previous strains (Alpha, Delta, etc.) ? This strain might spread faster and more easily, but if it’s less dangerous surely that’s good news to be shared.
Why? Perhaps because it doesn’t suit the narrative.
It isn’t transmissibility that should be of concern but virulence as it is this that affects mortality and morbidity rather than how fast people become infected. Apparently Ebola has low transmissibility but it certainly has a high virulence.
Both matter of course. We have had an inverse Ebola the past 19 months, with very high transmission but a very low IFR. Unless they are claiming the jump in deaths is due to this variant-variant (and not the move into Fall), then this is like hyping a bad television show of a decent movie. Moving on.
I should add, when I say low IFR some people think I am ignoring human suffering and death. I’m not. I’ve performed funerals and visited hospital sick. Both are awful. But I’ve visited those with cancer, car accidents, and any number of other issues. We are a species that begins to fall apart about 20 and sooner or later our bodies give way. We’d love for everyone to have more years but, it’s the life and impact we make in whatever years we have that makes the impact. Sad too many have lost sight of that the past 19 months.
This is how they should announce them.
Who needs evidence? Not the Nudge units.
Priming the public for the arrival of the New Really Scary Variant by first sending a message of objectivity and measured response about this new Not-So-Scary Variant.
Covid Crusher: Mix one heaped teaspoon of Iodine table or sea salt in a mug of warm water, cup a hand and sniff or snort the entire mugful up your nose, spitting out anything which comes down into your mouth. If sore, then you have a virus, so continue morning noon and night, or more often if you want, until the soreness goes away (2-3 minutes) then blow out your nose and flush away, washing your hands afterwards, until when you do my simple cure, you don’t have any soreness at all, when you flush – job done. Also swallow a couple of mouthfuls of salt water and if you have burning in your lungs, salt killing virus and pneumonia there too.
Gargling, using saline solution or tablets is a waste of time, because they deal with Covid in the body and not the virus in the head, where it is at its most vulnerable – how silly such an easy thing to destroy, is left to become the
bio-weapon which kills you.
I have been doing this for over 27 years and not one person has died from this simple cure, or been injured from it from those I have been able to pass it on too, myself included.
The Iodine in the salt kills Coronavirus or the Flu, in the nasal passages of the head and flushes out the escutcheon tubes to the ears, the brain stem and the brain bulb, so no long Covid either – dead Coronavirus = no Covid in the body ever and the salt water provides a protection over the surfaces where Coronavirus and the Flu like to breed – pour a bit of solution on a flat surface and see how it dries – what viruses hate, because it murders them, kills them dead.
Irrespective of if you have been vaccinated or not, do my simple, free cure and avoid further booster shots if you can – or better yet, don’t get vaccinated at all – the vaccines kill, one way or another and horribly too, sooner or later and then we get around to those Nanobots and other things in the vaccines (shudder).
Richard
Please can someone tell me if the lateral flo test and the PCR test can tell the difference between the Comman cold flu or covid or are they just saying it’s covid??!Help I’m confused