
We’re publishing a guest post today from our in-house doctor, a senior clinician in private practice who used to work for the NHS. This one’s a bit of a shocker.
On Thursdays, the NHS releases the weekly summary data in relation to Covid patients. Normally this is a more granular version of the daily summaries – it has some hospital level detail and figures on non-Covid workload for comparison. Usually interesting but not especially informative.
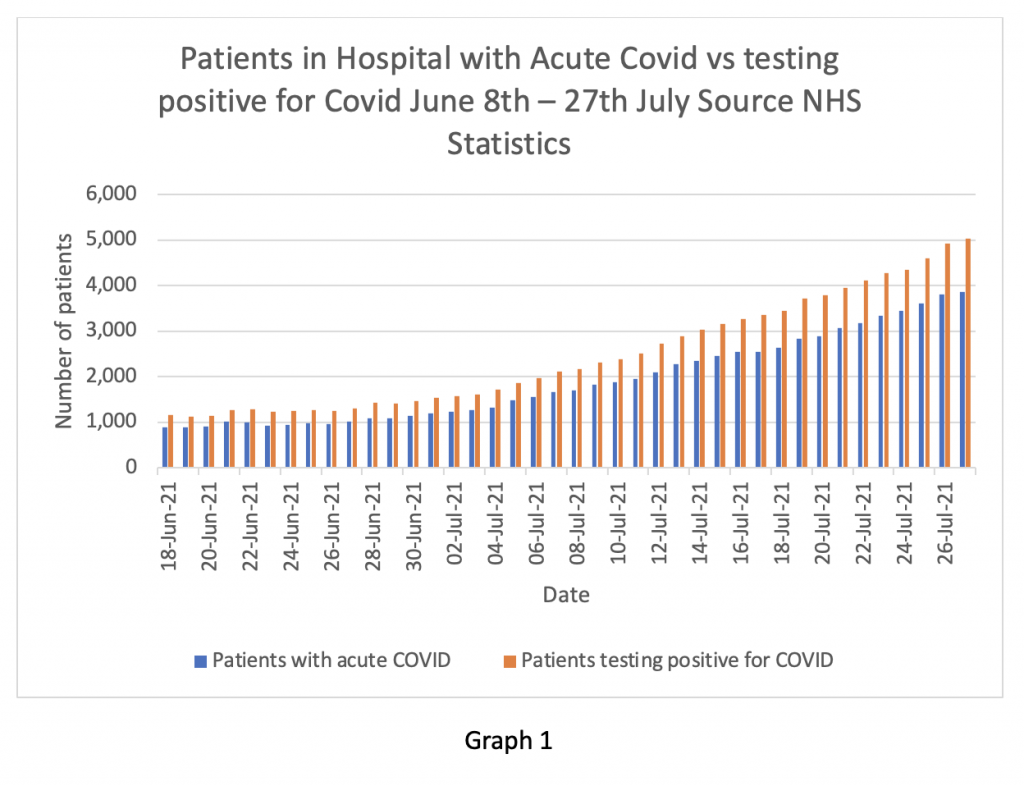
Yesterday was an exception. Placed down at the bottom of the page, almost like a footnote, was a ‘Primary Diagnosis’ Supplement. Graph 1 shows the information contained in that spreadsheet. I find it astonishing. In essence it shows that since June 18th, the NHS has known its daily figures in relation to ‘Covid inpatients’ were unreliable at best and deliberately untrue at worst.
The yellow bars are what the NHS has been telling the nation were Covid inpatients. The blue bars are the numbers of inpatients actually suffering from Covid symptoms – the difference between the two are patients in hospital who tested positive for COVID-19 but were being treated for something different – where Covid was effectively an incidental finding but not clinically relevant.
For example, on July 27th, the total number of beds occupied by Covid patients was reported as 5,021. However, until today, we were not allowed to know that only 3,855 of those were actually admitted with Covid as the primary diagnosis. There has been a fairly consistent over estimate of the true number by about 25% running back to mid-June – figures before that date are “not available”.
Why does this matter?
Well, in one way it doesn’t matter very much. Whether the burden of Covid inpatients is 5% of the available beds or 3.5%, isn’t massively significant – it’s still a relatively small proportion. NHS managers are already arguing that even patients with Covid being treated for another condition still need isolation procedures and present an extra burden on the system. They may argue that the NHS is still under strain from staff absences, stress levels and the waiting list backlog – so it doesn’t really matter if the published figures are somewhat inaccurate.
But in another way it matters hugely.
Firstly, it clearly shows that the NHS has been exaggerating the burden of Covid on hospitals by 25% since at least the June 18th and almost certainly for longer. All the senior NHS leaders and politicians quoting the number of Covid inpatients for the last six weeks have been painting a seriously distorted picture, significantly worse than the true position. Were they in ignorance about the true numbers, or were they deliberately misleading the public?
This also prompts questions about whether Government ministers have been given the same inaccurate information, or whether they too knew the information was exaggerated. This goes to the heart of how important decisions are made in the U.K. If ministers are being provided with incorrect information, they will make poor decisions. Has the NHS been deliberately ‘filtering’ information passed to ministers with the intention of influencing important decisions and maintaining restrictions on the public?
On the other hand, if the decision makers were aware that the published figures were false and that the true picture is significantly better, why have they been so slow to unlock and so ready to talk up the threat? Hospital inpatient numbers and the burden on ‘our NHS’ have been used for months to justify maintaining coronavirus restrictions or introducing new ones, such as vaccine passports, excessive and expensive testing for foreign travel and an unprecedented curtailment of civil liberties. Have ministers been aware all this time that the true picture was far less of a ‘threat’ than they have publicly stated? I think the public need answers to these questions from our elected representatives – and honest ones rather than the usual obfuscation and circumlocution.
On July 12th, Mark Harper MP, the Chair of the Covid Recovery Group, asked Sajid Javid in the House of Commons whether the information being published about Covid inpatients was accurate. The question was captured on the Parliamentary TV channel. Javid replied to the effect that the information may not be strictly accurate and he had asked for clarification from the Department of Health on these points. If these new figures are true, we now know the extent of the inaccuracy.
Of course, many readers will have long questioned the validity of the official data. I myself have found it difficult to reconcile the admissions from the community numbers with the monthly discharge figures set against the ever increasing numbers of ‘Covid inpatients’. The figures just didn’t make sense – now I know why.
In previous posts I have preferred to look at daily admissions from the community, rather than the figures for patients diagnosed in hospital, based on my suspicion that the data was manipulated. As readers will know, the number of positive tests in the community has been falling for the last week. Graph 2 shows daily admissions to hospitals from the community on the blue bars and the three-day rolling average on the orange line.
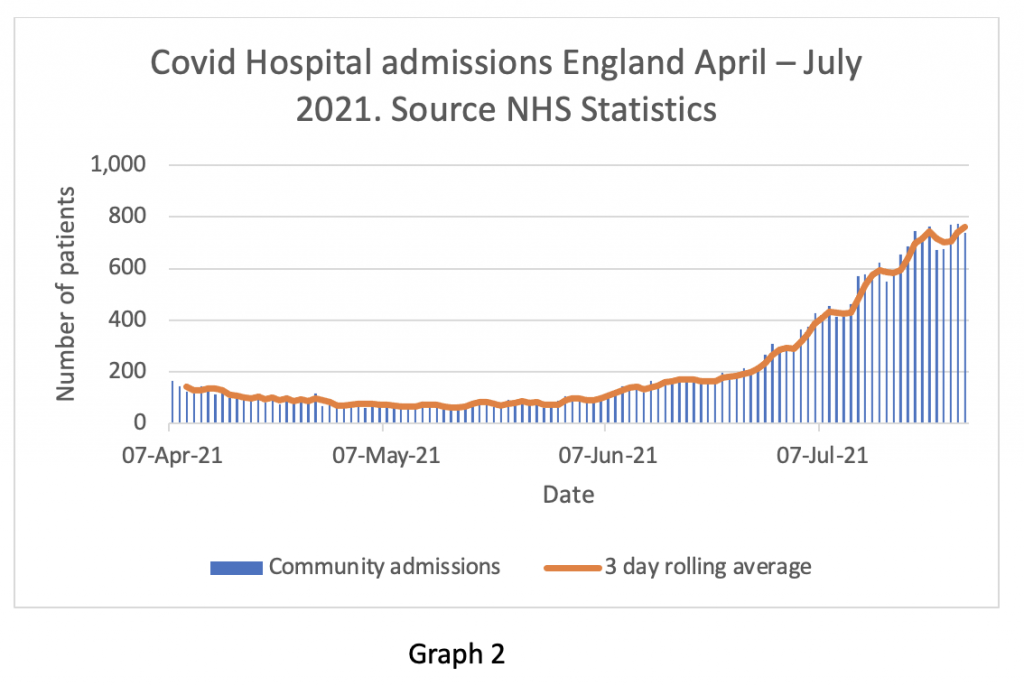
The rate of admissions seems to be levelling off – readers should remember that admissions usually lag positive community tests by 10 days or so. This is an early finding and may well prove to be a false indicator, but at the moment it is changing consistently with falling test numbers. The next week will be important in assessing whether admissions will mirror tests and start to fall. It is entirely reasonable for readers to question whether these figures are also exaggerated – I wonder that myself. Nevertheless, it is the trend rather than the absolute value that is the important issue, so I do think this dataset has utility. Fewer positive tests in the community should filter through to fewer positive tests on admission – even for patients admitted for other primary diagnoses – so it should be a fair reflection of the prevalence of the virus in the U.K.
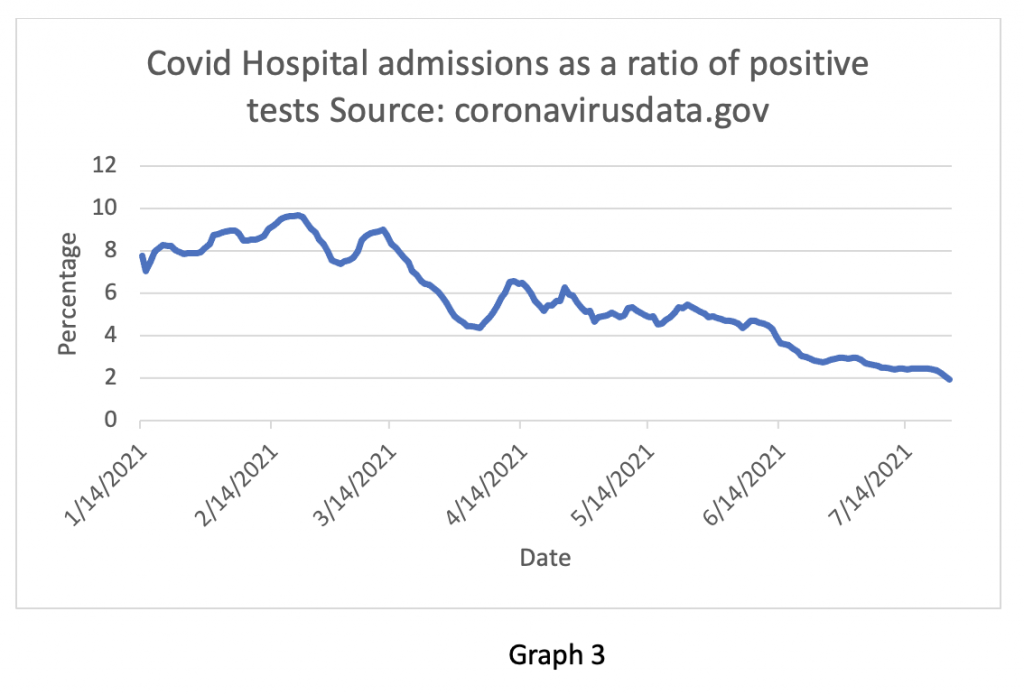
Supporting this finding is Graph 3 showing the fall in admissions in relation to positive tests. In February, about 10% of people testing positive ended up in hospital. Now only 2% do – in essence, Graph 3 shows that the risk of someone ending up in hospital with Covid has fallen by 80% from the peak number in February.
As with in-hospital infection rates, the NHS has once again been caught out concealing important information from the public. I find that truly shocking, but not surprising – in some ways I’m actually more surprised they have admitted it!
My suspicion is that the new Health Secretary and the newly appointed CEO of the NHS are keen to get the true figures in the public domain at the start of their tenure, knowing that it would come out eventually. In business, this is called ‘kitchen sinking’ – where a new CEO gets all the bad news out early with the hope of blaming his or her predecessor and embarking on a fresh start.
Nevertheless, Amanda Pritchard, appointed this week as the successor to Simon Stevens, has been the Chief Operating Officer of the NHS for nearly two years. Is it possible that she has been unaware of the deception until very recently and suddenly undergone a Damascene conversion to the cause of transparency?
What this issue is really about is trust, which is at the heart of any doctor-patient relationship. I can’t overstate how important trust is in clinical medicine. The managers of the NHS expect clinicians to practice a ‘duty of candour’ when interacting with the public. It seems they don’t consider themselves to be under the same obligation. A curious parallel with recent ‘double standards’ from our politicians.
NHS managers at the highest level have repeatedly been caught out concealing important information or distorting published data. They did it with in-hospital infection rates, with reported death figures and now with hospital inpatient numbers. Viewed in a generous light, this could be attributed to serial incompetence rather than deliberate deception. However, there is a pattern of behaviour here: concealment, denial, cover-up; trashing and vilification of people questioning the official narrative; followed by reluctant forced admission, spurious post hoc justification, dismissal of criticism and an appeal to the public to trust ‘our NHS’.
Our political and health care leaders may be about to discover that trust is a fragile commodity – and it’s running out fast.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
overall mortality is normal
everything else is dodgy stats
no ‘excess mortality’ anywhere in europe
its a fake pandemic (or at least is now)
I concur 100% Steve. It’s all confected.
I’m a Brit retired to Spain. My GP is a sixty-something, pragmatic, straight shooter who has refused the experimental ‘vaccine’. When asked a Covid-related question by a patient, his reply was, “I’m just a GP, you’d better ask Sanchez.”
My guess is that although this is what they are admitting to, it is in fact an under-count, deliberately. The truth, maybe 1 in 3, or even 1 in 2, will not come out for years.
https://www.sciencedirect.com/science/article/pii/S1201971220307311
It has been sequentially confirmed in subsequent studies that ADE of SARS-CoV and MERS-CoV also occur, with different mechanisms. Whether ADE works in other kinds of coronavirus infections remains to be investigated. Unlike dengue virus, ADE in SARS and MERS is not triggered by a heterovirus strain, however it is clear that the effects of both have negative consequences for the human body and are probably an obstacle to the development of viral vaccines.
“the NHS has been exaggerating the burden of Covid“
In other news, the current Pope at least pretends to be Catholic, and bears have been seen going to the toilet in the woods.
In all honesty, a mere 33% exaggeration is stunningly close to reality, based on the general standards set by covid panickers in our media, politics and healthcare professions over the past year and a half.
“… since June 18th, the NHS has known its daily figures in relation to ‘Covid inpatients’ were unreliable at best and deliberately untrue at worst.”
I don’t buy that.
It has been obvious from mid-2020, to any data-literate person, that almost all figures relating to Covid were totally f.ed. Then we had the PHE debacle – but essentially nothing much changed, simply because the pile of trash was unsortable.
I can’t believe that statisticians in the NHS were unaware of this glaring inaccuracy.
Why else have we all – from that early date – been resorting to all-cause mortality figures to tease out some truth about actual impact?
I am not at all sure that this latest downward revision has got it sorted. Questions about diagnosis/attribution remain – and the use of the term ‘Covid’ in a loose way doesn’t inspire confidence.
Do they have to keep up the ‘threat’ to push through to the end game of COV-ID, ‘segregation passports’
“This one’s a bit of a shocker.” Lol. Shocking that they’ve admitted it. And I don’t believe them – it’s most likely much higher than that.
I still think it’s worse than this. I reckon a significant proportion of the blue bars aka patients with “acute covid” are people who have still been admitted for something else but also have a bit of a runny nose so they’re not being treated for covid.
Impossible for the NHS not to know the true figures from day 1. That information about every patient is sent on discharge.
Absolutely superb piece as always. I fully understand why the author can’t give his name to these articles, but how I wish today’s article could be published in the Daily Telegraph.
If they openly admit 25% after 50% went through the press, they’re trying to save their numbers by relatively marginally reducing them: Ok, we admit, we did lie to you. But only a little bit and it didn’t matter, anyway.
My (absolutely unjustified) guess would be “25% without any flu symptoms”, “50% with slightly raised temperature or a runny nose or something like that” and maybe 25% who are actually treated because of COVID.
Even the much-hyped continuous cough is a flu symptom and one that usually goes away on its own after a few days. It’s just pretty rare.
It would also be interesting to find out just how these patients were tested for Covid. As we know, the lateral flow tests have already been ‘trashed’ by the CDC as not fit for purpose and the swabs apparently contain carcinogenic material. Now I read that the CDC will not renew the emergency approval for the ‘gold standard’ PCR test when it lapses at the end of December, because, reading between the lines, the test can’t differentiate between Covid and Flu.
Nothing to see here, move along and get your jab.
Had a conversation with man this morning who came to mend our hot water tap.
His grandmother died “from Covid”. How old was she? 93. She had gone into hospital with another (unspecified)problem but with a negative ”test” result. The lady in the next bed “tested” positive and then grandma did too. Obviously it was Covid that killed her, in spite of the fact that she was hospitalised for another problem entirely!
Very interesting interview here about the ingredients of the Pfizer jab:
STEW PETERS SHOW : DEADLY SHOTS! Former Pfizer Employee Confirms Poison
https://www.bitchute.com/video/SK9KsEBENXJd/
Maryland Nurse describes horrific side effects she is seeing in the vaccinated:
https://twitter.com/i/status/1420427803749662724
ADE: Is a Coronavirus Vaccine a Ticking Time Bomb?
https://sciencewithdrdoug.com/2020/08/01/is-a-coronavirus-vaccine-a-ticking-time-bomb/
If you can please look at this Facebook group John Dees Almanac masses of stats to show how PHE are manipulating the figures
https://www.facebook.com/groups/johndee333/?ref=share
BELOW a screenshot of data definitions on the UK GOV coronavirus dashboard (see ‘about’ sections) telling us plainly that that inpatients will count as an “admission” if they happen to test positive during their stay for whatever reason they happen to be in hospital in the first instance.
Notice also the wording of the second sentence which plainly states they count admissions to mental health and disability trusts as well as independent service providers. None of these are centres where COVID is actually treated but they still count!
It’s not just this. Everything has been geared to exaggerating the extent and severity of Covid 19. For example, if you die from any cause within 28 days of testing positive for SARS-COV-2 then you are recorded as dying from Covid-19. Patently absurd!
If it wasn’t for Carl Heneghan everyone who had ever had covid and died from whatever cause was a “covid death”, forever.
This article from 2020 perhaps gives a much better idea of how many cases were from covid cases. By late April 2020 most cases were with not from (see attached chart from that article)
Changes in the hospital admission profile of COVID-19 positive patients at a central London trust
And then there was the Scottish audit from Summer 2020
Counting people in hospital with COVID-19
Audit findings
The audit of inpatients identified 384 patients in hospital at 1am on 26 August across Scotland who had previously tested positive for COVID-19.
The majority of these patients (87%) were in hospital for a condition unrelated to COVID-19:
The audit showed that 8% of patients were either receiving treatment for COVID-19, were in rehabilitation after their treatment for COVID-19 was completed, or were in hospital for COVID-19 related complications. (5% of patients could not be classified into the above categories.)
(note that Scottish audit was before they changed the definition in Scotland to positive test within 28 days but it still illustrates what was going on)
I will never trust the NHS or any Government ever again- this is not a good position for me or them.
The ratio of admissions to positive tests (see above graph ) is very low and falling because the tests are inaccurate and at up to a million a day most positives are indeed FALSE.
) is very low and falling because the tests are inaccurate and at up to a million a day most positives are indeed FALSE.
Still only a small minority of people, Sceptics etc, are even interested in these essential truths. Very frustrating…
I remain unsure whether to blame the politicians, who as lay folk have the same inability to consider epidemiological evidence as the general population. However your in-house doctor has missed a small trick in his/her excellent commentary (I would love to know who he is, as we have views that are almost identical).
Many months ago I questioned whether hospital admissions were from Covid or with Covid. Strictly this is not accurate. Admission with a positive “Covid” test is NOT admission with Covid, but an admission of someone who has or has had infection with SARS-CoV-2. Covid-19 is a distinct clinical condition that results from SARS-CoV-2 infection – in other words, it is a subgroup of infected people (who get very sick). Thus it is important to maintain the clear distinction between the two.
Furthermore if you are admitted and then found to have a positive test, that may mean you never had SARS-CoV-2 infection on arrival. I am not clear whether the “Covid” figures distinguish between those who had a positive test on admission and those who later developed one, in other words who acquired it in hospital. The evidence suggests they don’t.
So please let us be absolutely clear that a positive test is NOT confirmation that you have Covid.
Of course nothing on the BBC about this the Olympics are a very useful cover big up the games ignore the NHS blundering!