The Omicron variant is known to have a relatively high number of mutations, including in the spike protein, and is therefore better than previous variants at escaping vaccine immunity, especially, and also natural immunity. As a new pre-print study from South Africa explains:
The Omicron variant is characterised by between 26 and 32 mutations in the spike protein many of which are located within the receptor binding domain (RBD). In addition Omicron has three deletions and one insertion in the spike protein, and mutations outside of the spike protein. Many of the mutations are either known or predicted to contribute to escape from neutralising antibodies, and work on earlier variants of concern has demonstrated that such variants can be antigenically very distinct.
The study looks at the reinfection rate in successive waves in South Africa and finds that the recent Omicron surge was characterised by a reinfection risk over twice as high as in the original wave – though it should be noted that this is from a low base, as studies have found natural immunity to confer 85-90% protection from reinfection (pre-Omicron).
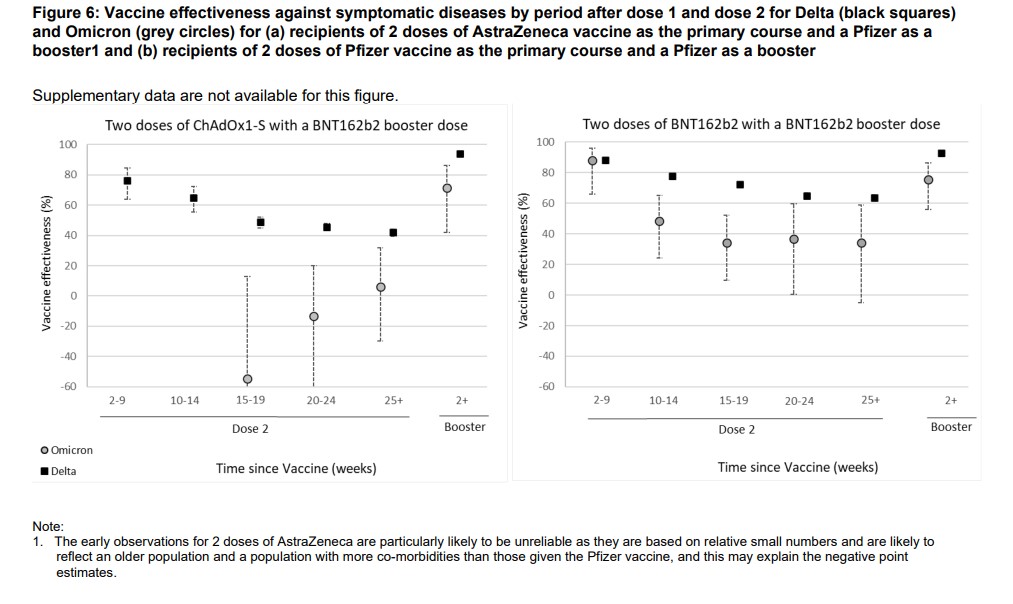
As far as vaccines are concerned, the UKHSA recently acknowledged the weak protection from two doses of the vaccines against Omicron, even publishing a graph showing negative effectiveness for the AstraZeneca vaccine, albeit with very wide confidence intervals.
Nonetheless, there is good evidence that previous infection will continue to provide robust protection against the variant, albeit at a slightly reduced level. Further evidence of this enduring protection comes in the UKHSA’s latest daily Omicron report from December 19th. It shows that Omicron is partially replacing Delta to different degrees in different regions, suggesting the two variants are largely competing for the same pool of susceptible people.
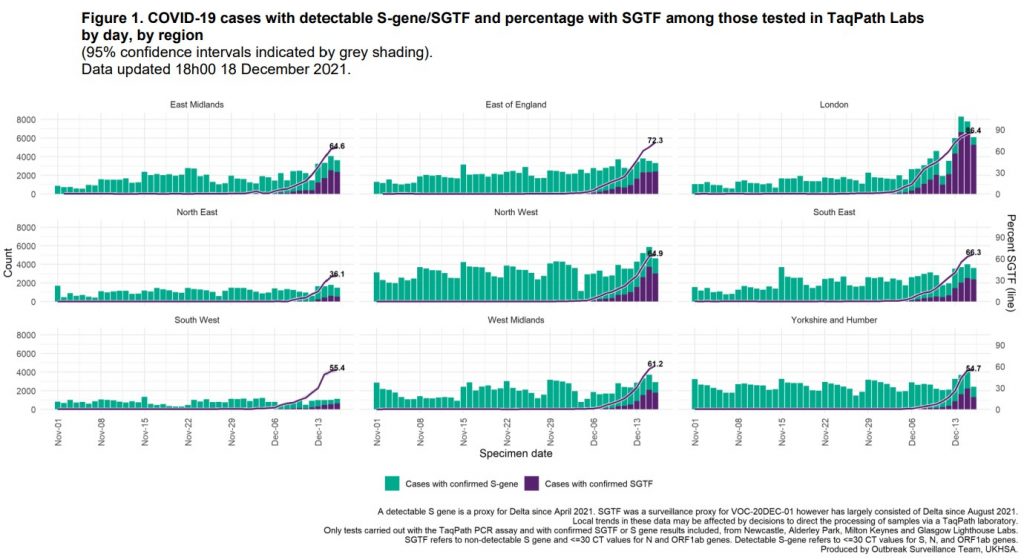
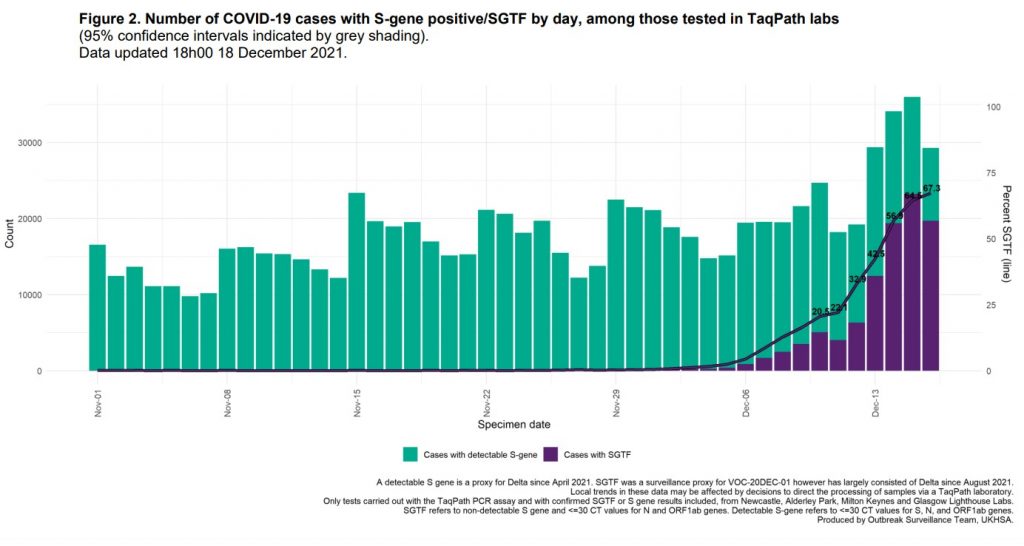
The purple lines in the charts above show the daily change in the proportion of PCR-positive samples with S-gene dropouts in low-Ct PCR positives, which are interpreted as Omicron. What’s interesting about these charts is that almost all of them show a flattening in the rate of increase of the Omicron proportion in each region in the last few days, but they are plateauing at different levels. London is flattening around 86% whereas the South West is flattening around 36%, and the rest are somewhere in between. Nationally, the Omicron proportion has begun to flatten around 67% (see below). Note while the overall number of positives (the height of the bars) for recent days may change as more test results come in, the proportions are unlikely to change much as there is no particular reason why delayed positives are more or less likely to be Omicron. Also, note that while overall reported infection numbers have spiked since December 13th, so far this appears to be mostly due to increased testing and there’s little sign yet of a similar spike in test positivity.
Why might the Omicron proportions be levelling off well below 100%, and at different levels in different regions? London has been the least affected by the Delta wave – it had average positivity of 5.2% between June 3rd and November 17th, compared to 9.5% in Yorkshire and the Humber – and so may be more susceptible to Omicron because of lower population immunity from over the summer and autumn. Here are those figures for each region.
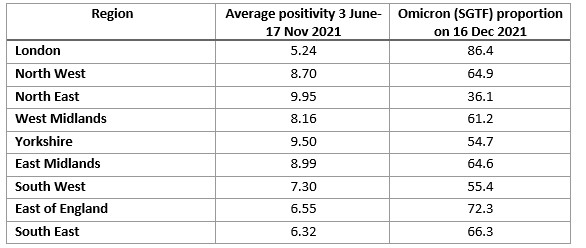
Is there a relationship between how strongly a region was affected by Delta and how susceptible it is to Omicron? Here’s the data in the above table plotted on a chart.

That’s a strong negative correlation, meaning the more Delta a region had, the lower the level of the Omicron (SGTF) proportion plateau. Does this help to answer the question of why the regions are flattening out at different levels?
Regions harder hit by Delta are, by definition, more susceptible to Delta (for reasons such as being less hard hit in earlier waves). So it makes sense that, now that Omicron is on the scene, the regions where Delta has been making more of an impact are finding Delta is better able to compete with Omicron and hold onto more of its market share. In places where Delta has struggled more, such as London, Omicron faces less competition from it and so can grab a bigger market share and push it out faster.
It’s true that you might expect regions hard-hit by Delta to have built up a decent amount of herd immunity to the variant by now. But for whatever reason the Delta outbreak has continued at a relatively low for six months (at different levels in different regions) and hasn’t shown signs of fading out, so evidently some susceptibility remains. The suggestion here is that it is the differing susceptibility by region that is key in determining how well Delta can compete with Omicron and so how much Delta can stay in the race. A number of countries last winter had a winter wave that was a mixture of different variants, and it appears that the U.K.’s winter wave may be a Delta-Omicron mix this year.
The broader point is that the fact that Omicron is not able to push Delta out completely, at least not yet, combined with the as-yet muted spike in positivity, is further evidence that natural immunity is holding Omicron off to a similar degree to Delta. If it wasn’t we would expect to see Omicron taking over everywhere and causing a big surge in overall positivity to boot.
Last year, countries around the world including the U.K. saw reported infections peaking and falling almost in unison in early January. Later analysis from Imperial College London using antibody testing showed that U.K. infections peaked in Christmas week. Winter flu waves often follow a similar pattern. One possibility is that it is the run-up to and celebration of Christmas itself that accelerates the surge to herd immunity (and beyond), which then abruptly peaks and falls once the festivities are over. This means we may see a similar phenomenon this year; one to watch out for.













To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Another Fine Mess
Too true!
Just look at the picture of those pair!
Our future???
Wonder if they share their ties?
Total imposters and squirming parasites that will soon be in charge of how we all live. I hear North Korea is nice this time of year, maybe we should all seek asylum
Labour scare the hell out of me and I am not Jewish but my background is although my family deny it. Hey, where did Goldsby come from. My Mom looks like Beatty on the old adverts.
If I were a Jew in England today I would be booking a flight out. Labour is an antisemtic party and David Lammy is the most racist person I can recall coming across.
And he actually called Brexit voters worse that Nazis.
Any country which recognises a Palestinian state is certifiably insane. I’m going to stick my neck out and optimistically say that the majority of the population from these insane ( Western ) countries do not agree with their lunatic politicians on this matter;
”Israel has long been the primary supporter of the Palestinian people, both on the West Bank and in the Gaza Strip. Israelis have opened their borders to Palestinian workers, to whom they pay high wages. They have accepted Palestinian patients, including even terrorists, into their excellent hospitals. Some of the Israeli kibbutz residents who helped Gazans were murdered by them on October 7. Even during the current Gaza war, Israel has provided more food, medicine and humanitarian aid to Palestinians than any country has ever done during wartime.
What have other countries done? Very little. Consider the fact that no Arab or Muslim nation has been willing to accept Palestinian refugees from Gaza. Perhaps these nations recall that anyone who has tried to help the Palestinians has lived to regret it.
After Israel forced its own people out of Gaza in 2005 to allow a Palestinian “Singapore on the Mediterranean,” instead, in 2006, the Palestinians elected Hamas, which built more than 350 miles of terror tunnels, a “city under a city.”
No wonder their neighbors prefer not to take Gazans in.
Perhaps Ireland, Norway and Spain might extend invitations to the Palestinians to become residents there?
On April 13, more than 1,000 demonstrators marched through the streets of Hamburg, Germany and demanded that the country become a Caliphate, with Shariah law.
The only reason that Ireland, Norway and Spain can safely recognize a Palestinian state is that they do not have to live with the consequences.
The truth is that few outside of Israel really care about the plight of the Palestinian people. The demonstrations on college campuses which purport to be “pro-Palestine” are far more about condemning Israel than about helping the Palestinians. We never see signs calling for a two-state solution, probably because most of these demonstrators do not want Israel to exist. “From the river to the sea” means no Israel and no Jews. If a Palestinian state were to be substituted for Israel in that area, it would be a tyrannical regime. The conflict would be between those who want to see it more like Iran, a theocracy that murders dissidents, or more like China, a communist tyranny that also murders dissidents. As long as Hamas remains a viable military and political force, there is no prospect for a democratic Palestine or a two-state solution.”
https://www.gatestoneinstitute.org/20683/israel-helping-palestinians
Mogwai, that is the most brilliant thing I have ever read of yours.
LOL, you’re a fast reader! All credit to those two authors though. They just tell it like it is. Terrorist-supporters will find something to whinge about though. Inconvenient truths and all….
All credit to those two authors though. They just tell it like it is. Terrorist-supporters will find something to whinge about though. Inconvenient truths and all….
Well, I read a lot and I work with data and words all the time. You hit all the right points. People no longer care about what is right and wrong, they care about who shouts loudest and who garners the sympathy vote fastest.
Successive Governments have failed miserably at combatting terrorist sympathisers. Let’s be honest here, most people are so stupid they took Death Jabs, so, of course they are going to follow fads not facts.
The irony is that they do not realise that they would be first in line if groups like Hamas took control.
I bow down to you mogs!
You really ought to think about political leadership with Gert!?
Hey flatterer Actually, there is an area where mine and Geert’s opinions regarding Islam diverge, and that’s how he says he wants to eradicate all mosques and Korans from the Netherlands. This is pure fantasy, let’s be real, and way too extreme, not to mention unrealistic.
Actually, there is an area where mine and Geert’s opinions regarding Islam diverge, and that’s how he says he wants to eradicate all mosques and Korans from the Netherlands. This is pure fantasy, let’s be real, and way too extreme, not to mention unrealistic.

Everybody should have a place to worship, just as a basic human right. It’s also a sign of a civilised society and demonstrates, even in these post-democratic times, that everybody’s rights to worship be upheld, regardless of the religion they choose to follow.
Mosques in and of themselves are not the problem, it’s the people that use them. Same for the Koran. It’s just a book filled with words, but it’s the people who interpret these words as some literal instruction manual that are problematic.
Mosques need to be somehow surveilled better so that these hate-preaching Imams can be identified and action taken accordingly, for example. But this too is fantasy because I think ( and it’s a close one ) that of all the groups it’s the Muslims that are the biggest victim card holders, so much so that they’re like a protected species, with special status as far as the law’s concerned. Even after the debacle and national shame that was the Pakistani rape gangs ( and some are only just being convicted now, decades later ) it seems the authorities are still petrified of having the ‘Islamophobia’ slur hurled at them.
This is the irony, I find. These people who have come, or whose parent’s came, from a majority Muslim country, look and see how the minority Christians, Hindus, Jews ( if there still are any ) are treat in those places. They’re persecuted and treat like absolute shit, e.g in Egypt, Pakistan, Nigeria etc. Churches are burnt down, non-Muslim girls are kidnapped, abused and forcibly converted then married off to their abuser, men are slain for sport, “blaspheming” or not paying their dhimmi tax ( jizya ).
But these very Muslims who would do this to minority religions over there come here, where they’re a minority themselves ( though getting more and more over time ) but they’re the first to cry “Islamophobia” if people unwittingly say anything that upsets them, let alone shows a picture of their paedo prophet or is remotely critical of Islam. So you see the double standards at play? We must bend over backwards to accommodate them, appeasing them at all times, but if we moved over to any Middle Eastern country ( aside from Israel ) and wanted to live our normal Western lives ( especially females and what is considered normal dress here ), be gay, practice Christianity, wear a bikini on the beach, we wouldn’t last 5 minutes. Our lives would be made miserable and our safety and welfare in serious jeopardy. But we would have no recourse whatsoever.
My values do not align with theirs, and that’s why I’d never move to a Muslim country. Their values don’t align with ours but yet they move here anyway and we must accommodate their alien ideology and customs, capitulating for ever more? Make it make sense!
Great comments on this issue by you again as others have pointed out, and getting rid of Mosques and Korans will never happen as you say and if we have churches and Chapels then other religions perhaps need their buildings to do their religious stuff as well.
The problem comes about because Islam is NOT just a religion. It is a political and legal system as well. I have no problem with people worshiping, but I do have a problem with practices alien to our own culture eg regarding treatment of women, what clothes they should be allowed to wear, what education they are allowed to get, whether they can drive, whether they can go out without a male relative etc and gay people and many other things. So if that is what Islam wants then I don’t want it here. Please worship but do no bring any of that to this country please.
Cheers Varmint, and agreed. As Tommy Robinson said: “If you put Islam before British values, you’re not a British Muslim but a Muslim living in Britain.”
As Tommy Robinson said: “If you put Islam before British values, you’re not a British Muslim but a Muslim living in Britain.”
Plenty of evidence of this around, unfortunately.
Agreed! If we censor, then we are no better! Live and let live
Powerful.
What I’d add to it is that the West has become so complacent that peoples lives are a fashion fad. It changes faster than handbags. A few years back it was “oh Jeremy Corbyn”.
Then it was Mother Theresa Zelensky who denied a democratic vote to a third of his population and removed their right to hold any public office.
Now, it is ignoring the beheading, rape and torture of 1200 innocent people.
Many Jews in Israel have dual citizenship and they should be encouraged to leave Israel back to their other country.
Israel should revert back to Palestine and be governed by the indigenous Palestinians.
Peaceful Jews who want to stay would be welcomed.
Foreign Jewish Zionists are not welcome.
76 years of an Israeli State has been an abject failure.
Oh, here he is yet again, Mr Yellow Star of David. I doubt I’ve seen or heard anyone more antisemitic than this creature. Well, Labour could give him a run for his money I suppose.
What exactly qualifies “Peaceful Jews who want to stay would be welcomed.”.
Welcomed to their own country?
Or would it be the Jewish slaves who adhere to Arbeit Macht Frei?
Would they be encouraged in the same way as the other bunch of creatures like you “encouraged” them to get onto trains?
I note that one person gave a thumbs up to this sickness. Would you mind explaining why? I thought not. Sick people never do. After the murders they say “nothing to do with me”. Do you realise you put a thumbs up to babies being beheaded?
August 25, 1933, is the date of the signing of the Transfer Agreement, which enabled 60,000 German Jews to leave for Palestine while taking some of their money with them.
Millions of others left on trains.
“Persecuted Jews attempted to find safe havens abroad. Emigration reduced the number of Jews in Germany by about 170 thousand by 1938 (from a total of more than half a million in 1930). Unfortunately, many countries, among them the USA and Great Britain (in Palestine), imposed restrictions on refugees at this time. As a result, even those Jews who expressed a desire to leave Germany were unable to do so before the start of the war. As a consequence, they died afterwards at death camps in the East.”
So, hey, Mr Yellow Starman, is this what you mean? You disgust me.
A peaceful one state solution where Muslims, Jews, Christians and other faiths live in harmony.
Your being a little tongue in cheek!
Religions live in harmony??
Could an irresistible force be stopped by an immovable object?
ie: your god..my god?
“Our god says its our land”
“Well our god says its our land!”
Never ending story!
That doesn’t on the face of it sound very realistic. Nation states can be pretty fragile, and there seem to be quite dramatic differences between the different groups that are now living on that land.
That is Galloway’s proposal.
The massacre of October 7th has shown that is not possible.
Why are there no street protests about last years ethnic cleansing of Armenians? Why aren’t Lammy and Starmer exercised about that? In any case, their foreign policy will have to be whatever Washington’s is.
Well said. It should be called The Holy Land – idea courtesy of philosopher Charles Eisenstein.
Destroy Hamas?
Do you agree?
OK easy yes or no
Do you back hamas?
No.
I agree with the position China has taken.
China signals that October 7 was an exercise in international law.
The Chinese representative points out to the ICJ that armed resistance against the occupation is enshrined in international law and is not terrorism.
No straight answer then?
76 years of failure.? Not for Israeli’s. They have built a successful and prosperous nation, despite being in the middle of hostile neighbours. Maybe if you think about the Gaza Palestinian people being oppressed by their choice of leaders, rather than the State of Israel, you might start to see why we see a different point of view.
“Prosperous” due to billions in aid from the US and the theft of land and resources from the Palestinians.
I think it fair to say that we dont see eye to eye on this, and so I wont be engaging you in discussion again about it.
Have you ever considered moving to palistine?
Sounds like you’d love it there, amongst your own kind!
And leave us amongst our own kind, if that’s OK?
If your going to lecture us about our shortcomings, do it from your place of loyalty, not from a safe distance place like the west!
I have always found Labour a disturbing party but the current iteration is the most appalling yet.
Following the Galloway result in Rochdale and then the local elections Kneel realised that his huge postal vote – the third worlders from the Indian subcontinent – was draining away and rapidly putting his dreams of Downing St at risk. What to do?
Bollox to Britain and the British people the election is all about Gaza.
What a patriot.
Deep shit pending.
Oh for a bit of balance for a change DS. Anyone might think you’re a bit pro Israel.
I mean, nobody even in authority in Israel would advocate and countenance the removal of Palestinians from Gaza much less actually say it –
https://www.aljazeera.com/news/2023/12/31/israeli-minister-reiterates-calls-for-palestinians-to-leave-gaza
Then there’s this –
https://www.nbcnews.com/news/world/gaza-nakba-israels-far-right-palestinian-fears-hamas-war-rcna123909
So on the face of it one could say they’re as bad as each other, unless you look at the actual death/injury totals for Palestinian/Jew side since 1948.
Steyn on Farage
“Nigel took his gatekeeping seriously – and not just on the domestic front, “distancing” himself from Tommy Robinson and Tommy-associated issues such as Islam and the industrial-scale sex-slavery of thousands of English girls. As Gavin Mortimer reminds us, a decade ago Farage also rejected any Euro-collaboration with Marine Le Pen because her party had “anti-Semitism and general prejudice in its DNA“. Geert Wilders (for whose fine book I am proud to have written the introduction) was furious with Farage and attempted to broker a rapprochement. Nigel was having none of it.
So here we are a decade later:
I think Nigel over-gatekept.”
I think it would have been difficult to predict what has happened over the last 10 years and the journey we have all taken…
Mark Steyn nails it.
Unprincipled scum will do anything to win a few votes. I hope this little wheeze backfires.
The author displays a one-dimensional view unworthy of the usual standards of the site. It is not just a case of rewarding or recognising Hamas. UK Labour is joining the growing proportion of the world that recognises and wants actively to end 80 years of Zionist oppression of the Palestinians.
Mr Jones is probably too unsubtle to understand that while people like me do indeed condemn the attacks on civilians of October 7 we nevertheless understand what desperation can do to an oppressed people. We can imagine life as a black US or Arab Moslem or Spanish slave. We understand the colonising evil done to a US Indian or to an apartheid-era black person in South Africa. Indeed many of us see Mandela as a hero.
And, in an ironic twist on the reality of human nature, that includes people who say they support Israel. Funny old world that is beyond the ken of people like your Mr Jones.
There should be no Palestine and no Israel. Only one country should exist covering that region and it should be called the Holy Land. Here all Christians and Muslims who are currently being persecuted by the Zionists may then live peaceably with Jews. The philosopher Charles Eisenstein came up with the idea. Nothing else will work. The Zionists have destroyed too much of Palestine for a separate state and should one arise they would only seek to destroy that too.
Could the poll of Palestinians that this article references have been conducted after the Israeli had started destroying Gaza, in which case it is not a surprising result.
People understand instinctively that rewarding the worst pogroms since the Holocaust with a push for Palestinian self-determination is an example – to put it mildly – of rewarding bad behaviour. …
Are you referring to the approximately 1200 Israelis killed during what has repeatedly been referred to as a military action on 7th October, two-thirds of which were probably killed by ‘friendly fire’?
Or are you referring to the tens of thousands of Palestinian civilians bombed, shelled or machine-gunned since?