Another week, another Vaccine Surveillance report (now published by the U.K. Health Security Agency (UKHSA), the successor to Public Health England), and with it more worrying news on the vaccine front.
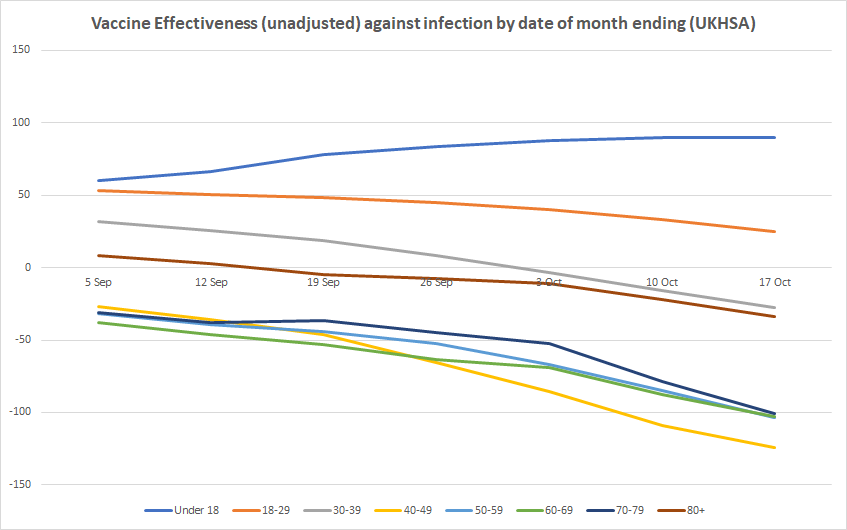
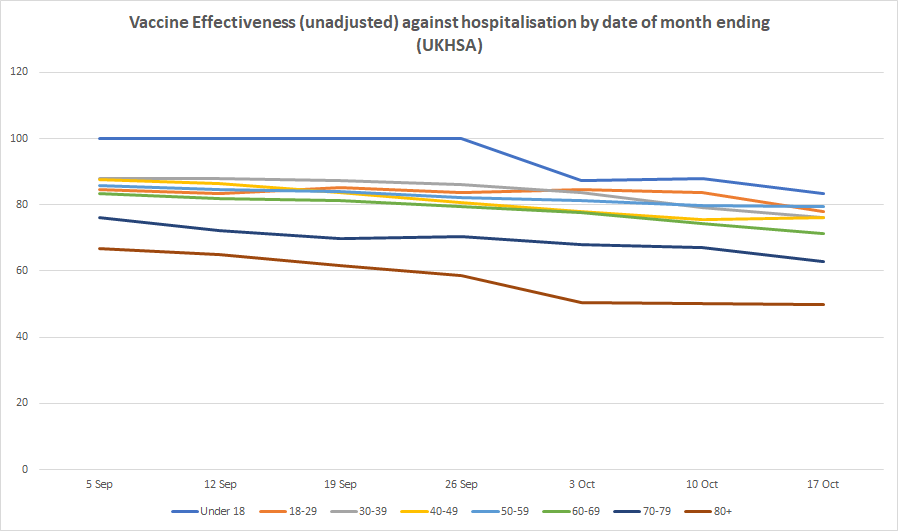
Infection rates in the double-vaccinated compared to the unvaccinated continue to rise, meaning unadjusted vaccine effectiveness continues to decline. Infection rates are now higher in the double-vaccinated compared to the unvaccinated by 124% in those in their 40s, 103% in those in their 50s and 60s and 101% in those in their 70s, corresponding to unadjusted vaccine effectiveness estimates of minus-124%, minus-103% and minus-101% respectively. For those over 80 the unadjusted vaccine effectiveness is minus-34% while for those in their 30s it is minus-27%. For 18-29 year-olds it is 25%, so still positive but low, while for under-18s it is 90%, the only age group showing high efficacy. Vaccine effectiveness against emergency hospital admission and death continues to hold up, though with some indication of gradual slide, particularly in older age groups (see below). (For definitions and limitations, see here.)


The UKHSA has continued to receive criticism for publishing this data, with claims that the figures used for the unvaccinated population are unreliable and likely too high, artificially suppressing the infection rate and vaccine effectiveness. Cambridge statistician Professor David Spiegelhalter put out a scathing tweet on these lines on Friday, but he didn’t elaborate on his claim or link to an article explaining it further.
Professors Norman Fenton and Martin Neil have argued that in fact the PHE/UKHSA data may underestimate the number of unvaccinated rather than overestimate them, which would have the reverse effect.
Either way though, what wouldn’t change is the fact of the large and fast decline in effectiveness against infection. This is now generally acknowledged among many scientists (likely caused by waning over time or new variants or both), though has not had the logical impact on Government policy one might have expected and hoped for of eliminating the rationale for vaccine passports and mandates.
A further point revealed for the first time in this week’s surveillance report is that the vaccines may actually hobble the body’s ability to develop the strongest immunity once infected. As noted by Alex Berenson, the report mentions (in passing) that “recent observations from U.K. Health Security Agency (UKHSA) surveillance data” show that “N antibody levels appear to be lower in individuals who acquire infection following two doses of vaccination”.
The report does not elaborate on this, but on the face of it it is a startling admission. It is basically saying that a certain kind of antibody which is not produced by the vaccines but is usually produced by infection (and hence is used by PHE/UKHSA to identify those with antibodies-from-infection) is not produced so well by those who are infected post-vaccination. Insofar as this is true it means the vaccines may actually prevent the immune system from developing the strongest form of protection against reinfection. This phenomenon of the immune system being in some way hobbled by the way it first encounters a pathogen is well-known and is referred to as original antigenic sin.
There would be a number of implications of this. It would mean that since the vaccine rollout got going the prevalence of N antibodies in the population has ceased to be a reliable measure of how many people are previously infected (which might explain why it has been rising so slowly during the Delta surge). It would also mean the vaccines may make reinfections and serious illness upon reinfection more likely. Plus likely other things as well.
This is something that should be investigated fully and the results published so that its impact can be properly assessed and understood.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Pointless law. Unenforceable without creating all sorts of knock on problems. Like driving even more support for the religious martyrs they will create.
We’re stuck with the problem. Shouldn’t have let all those Muslims in in the first place if they didn’t want them to have political influence.
It’s one thing to let Muslims have political influence over worldly affairs which concern them, eg, regulations for mosques in resdential neighbourhoods. But Imams claiming that Allah requires people to ‘vote’ for a certain foreign policy is something entirely different, as they’re not formally speaking in their own capacity as fallible and opinionated humans in this case. An atheist would claim that they obviously do because this cannot possibly be different. But not all people are atheists.
Does it really matter what the method of coercion is?
What’s the difference between an Imam saying God will be angry with you or a BBC appartchik telling you you’re a facist if you think certain things?
To me both act with coercive intent.
To believers I guess there would be a huge difference
Not even the most ardent admirers of the BBC believe that life is a temporary trial to prove yourself worthy in the eyes of the BBC and that – after death – a council of former BBC directors general, Dr Who actors and Chris Packham as climate expert will judge your eternal soul to either be worthy of joining the ranks of the blessedly carbon free in paradise or spend an eternity being tortured among the other damned in hell.
Two historical examples:
In Mein Kampf, Hitler made a dedicated effort to show that what he believed to be his political mission was grounded in a positive vision of lived Christanity and that he was really doing (or rather, panning to do) the true work of God on earth.
From January to September 1915, divisons of the German 5th army under crown prince William of Prussia conquered most of the forest of Argonne in a series of bloody, close-combat trench fighting actions from the French. This involved weeks of digging saps while constantly being shelled until the sap heads where sufficiently close to the French trenches. After preparatory artillery barrage, the German infantrists would climb out into the open, work their way accross the devasted forest of no man’s land as good as they could and finally, break into the enemy trenches and kill those who didn’t surrender with hand grenades and bayonets. After each major success, a field church service the crown prince attended would be held where the exact same people, now in as good a dress uniform as they could muster, would listen to a sermon and sing hymns to thank the Lord Almighty that he had granted victory to them.
Religion used to mean a lot more to people than us modern moral relativists and spiritually lazy agnosticists can imagine. It sill means a lot to people who aren’t.
Hardly a problematic law if it has been applied only once.
Useful else otherwise churches will have to register as campaign organisations and account for their expenditure; more seriously it would facilitate religion based politics which we got rid of a long long time ago in GB.
It’s nice to see Mr Tucker apply his considerable writing skills to a serious topic instead of just trying to be funny.
Giles Fraser, a left-wing Anglican priest, or, worded in another way, Giles Fraser, a professional Christian preacher who just doesn’t believe in God, is making a fallacious argument, either knowingly or because he simply can’t imagine that religion could be more than going through some traditional motions: 500 British business leaders arguing for a certain economic policy they believe to be necessary is them talking about a topic people can legitimately have different opinions about. Eg, is a policy 500 British business leaders favour really good for everyone or mainly for themselves and could 500 British business leader not as well live with policies favoring them a little less and other people somewhat more? This is not true for a Vote for Rufur Lameun’ or your soul will be damned for eternity! statement by some set of religious leaders. These deal with absolute truths. They’re not absolutely truths to non-believers, like one Giles Fraser, but to believers, they are.
The very concept of elections requires that voters are free to make up their own mind, ie, that elections are part of the way humans organize their own worldy affairs with God tacitly tolerating whatever folly comes from this. People who claim otherwise seek to abolish them.
The spiritual influence law should definitely not be repealed, but I would not be at all surprised if it was being broken behind closed doors and in a language other than English.
In some constituencies the Imams instruct the ‘bruvvers’ to apply for postal votes and when received the Imam sends his troops out to collect the unmarked slips which are then filled in at the local mosque.
George Galloway won the Rochdale by-election with a postal vote amounting to 42 % of votes cast. Fraud? Heavens know. Move along now.
Seems pretty clearly to be a free speech issue. The imam should be free to make his statement about who should be voted for. The person who votes has the autonomy to follow the imam’s directive or not. Any other organisation or person can mount a campaign against the imam’s directive if they think it is wrong. The best counter to misinformation is information, not suppression.
“The person who votes has the autonomy to follow the imam’s directive or not.”
Our idea of democracy relies fundamentally on the protestant notion that man is the arbiter of his own conscience. Religions which deny that can only coexist peacefully with it when the religious leaders refrain from making political statements in their capacity as such. The Imam is free to speak his opinion. But he must not claim that it would be the will of God instead of just his opinion.
Freedom of speech refers to the freedom to inform others and not to the freedom of giving illegal or illegitimate orders to them.
I suppose Blair will be kicking himself fo not revoking that law as he revoked so many other useful laws. No doubt hiw protege Starmer will do it instead.
Our Jess only won her seat by 600 votes.
On the other hand, Dr Alin-Khan who has done medical service for charities in Gaza and Israel increased her majority by some thousands.
On the Gaza issue itself, as a start-up party with little funding, the Workers Party secured 200,000 votes.
And these Labour MPs try to deflect attention from all this by claiming that people from all diverse backgrounds voted for Labour.
Shouldn’t Steven Tucker be concluding that we ought to discriminate against Moslems for some or all of … entry to the country/right to reside/right to vote/citizenship?
I’m sure he left that to us. And I have long thought as much.
Although I hate to say to, and I’d love to think I am wrong, but as our present governments, including those of the future, will not see a problem until it is far too late, there is a high probability of a civil war of religion within the next fourty years.
Yes, I do fear for my grandchildren.
But why leave it at all? Why not follow what he thinks to where it takes him? Is he, for all his outspokeness, afraid to take that last step?
The British Establishment, particularly Labour, currently has the tiger they imported by the tail but their grip is visibly slipping.
They are now terrified of what they have done, since it has started to impact on “their people.” The widely publicised pictures of Angela Rayner, wearing a cover-all dress, pleading with a group of Muslim “Community Leaders (all men, no women permitted) for their votes demonstrates that Labour is now awake to the threat but thinks that appeasement will work.
It won’t.
We are rapidly heading towards large-scale civil unrest.
What of the ‘spiritual influence’ of political activist college tutors sending out e mails to their students to get up and vote Labour? That certainly happened and no doubt happens.