We’re publishing an update this morning from the Daily Sceptic’s in-house doctor in which he analyses the latest NHS hospital data. Conclusion: no need to panic.
I have been a bit quiet lately, partly due to being on holiday and partly due to waiting a while to examine what trends are emerging from the hospital admissions data over the later summer.
On looking at the latest figures and associated media commentary I have been reminded of an old Russian aphorism from the Soviet era: “The future is certain, but the past keeps changing.”
For example, on February 3rd, 2020, Boris Johnson, warned of the danger that “new diseases such as coronavirus will trigger a panic”, leading to measures that “go beyond what is medically rational, to the point of doing real and unnecessary economic damage”.
I didn’t catch any reference to that (very reasonable) remark this week when the Prime Minister imposed further taxation on the working-age population and the companies that employ them. Before returning to the airbrushing of recent history, I will consider the hospital level data over the last month to discern trends and discuss what reasonable inferences we can draw from the numbers. I confess that some of the information doesn’t quite make sense to me – I will elaborate on this point later.
The first and most glaringly obvious fact is that the catastrophic tsunami of hospitalisations confidently predicted by all the experts who have assumed the governance of the U.K. has failed to arrive. How annoying that must be for Richard Horton, Editor in Chief of the Lancet, who described the relaxing of restrictions in July as “driven by libertarian ideology” rather than the data. Or Trish Greenhalgh, Professor of Primary Care Health Sciences at Oxford University, who said that “the Government policy seems designed to increase cases” and predicted there will be hundreds of ‘superspreader’ events in the coming weeks. The Lancet published a letter signed by 122 self-identifying experts which suggested that the Government was conducting a “dangerous and unethical experiment” in removing societal restrictions on July 19th.
Just to push the point home, readers may wish to consider Graph One. This shows the seven-day average of positive Covid tests on largely asymptomatic people against total patients testing positive for Covid in hospital. It can clearly be seen that the community tests peaked on July 23rd, rapidly falling off thereafter. Hospital numbers barely changed in response to changes in community test rates – so where is the epidemiological stupidity?
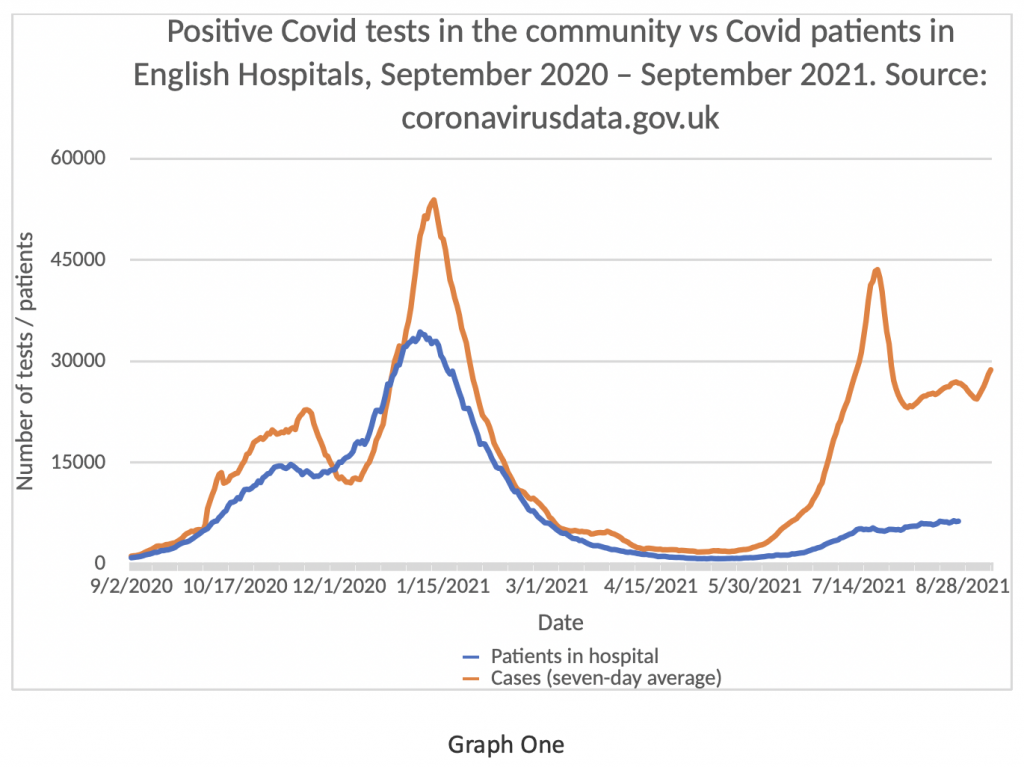
The latest updates on community testing from Public Health England (PHE) suggests that the current incidence of positive tests has been stable or decreased from week 28 (w/e July 22nd) to week 35 (w/e September 9th). I may have missed it, but I have not so far noticed a retraction letter in the Lancet from the expert commentariat.
Graph Two shows the number of patients testing positive for Covid admitted daily to English NHS Hospitals on the blue bars, with the seven-day rolling average on the brown line. It seems clear that there has been virtually no change in this graph since July 19th – the upslope trend levelled off and has remained flat ever since. Perhaps one of our epidemiological intellectuals could explain to me, a humble clinician, why it was ‘stupid’ to at least attempt to get our economy back to some sort of normality?
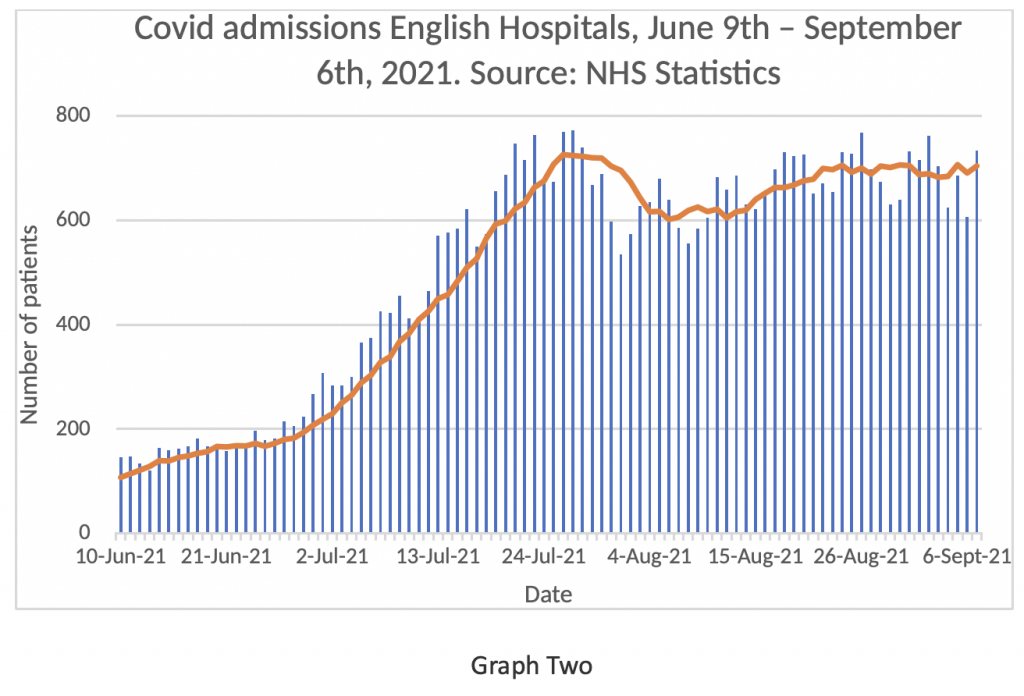
I noticed something else slightly odd about this graph. I have highlighted the Mondays (or Tuesday August 31st in the case of the bank holiday) in red. It seems to me that there is a ‘weekend trend’ emerging in relation to Covid admissions from the community. How can that be? Acutely ill admissions with respiratory infections do not usually predominate during the working week and fall off at the weekend. One possible explanation is that on Mondays the numbers could be boosted by patients being admitted for routine matters who just happen to test positive for Covid, rather than being acutely ill. There may be other explanations for the weekly pattern of variance which are not immediately obvious to me. Graphs Three and Four might shed light on this point.
Graph Three shows the number of patients in hospital testing positive for Covid over the last few months. There has been a small increase in numbers over the last six weeks, but not by any means a massive rise. Given that there are approximately 120,000 beds in the English NHS, this represents a Covid positive bed occupancy of around 5%.
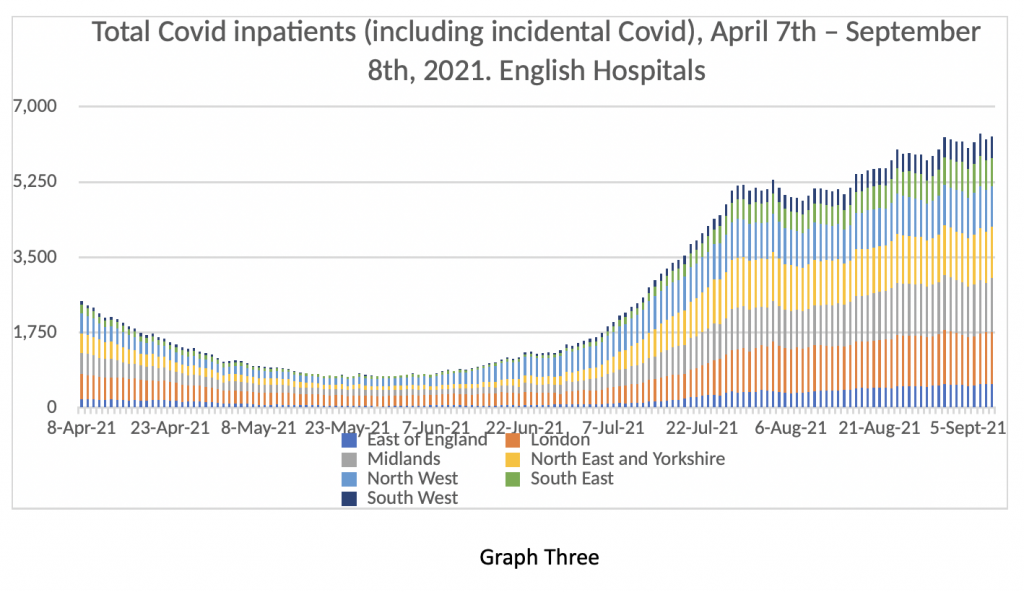
And yet, Graph Three is not all that it seems. Readers may recall the Department of Health was forced in July to release the ‘Primary Diagnosis Supplement’ – an extra spreadsheet detailing patients in hospital testing positive for Covid but not suffering from acute Covid – in other words where a positive Covid test may be an incidental finding. Graph Four shows that the NHS is still overstating the numbers in hospital with acute Covid by about 25%.
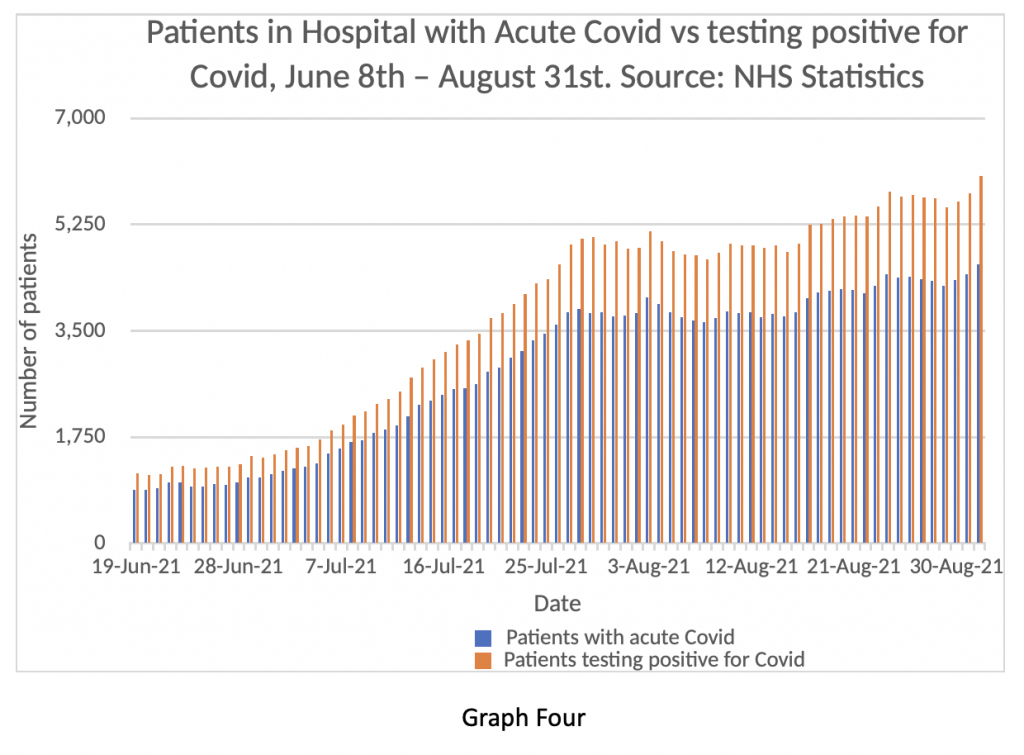
I naively expected when the authorities were forced by political pressure to finally release this information that NHS spokespeople would then revert to expressing the daily numbers differently and report only the numbers of patients in hospital with acute Covid. But clearly not. So, when the NHS say there are about 6,000 patients in hospital who have tested positive for Covid, by their own published numbers one can see that just over 4,000 of these are actually suffering from Covid symptoms – a bed occupancy of 3.3%.
To explore this point further, Public Health England have just released an influenza and COVID surveillance update. To summarise the information in this very detailed document, the rates of both hospitalisation and death from COVID per 100,000 population are much higher in unvaccinated people compared to fully vaccinated. Transmission of the virus seems similar in both groups for ages over 40, but transmission that does not lead to hospitalisation is of dubious clinical relevance. Unfortunately, the report provides figures as ratios, rather than providing raw numbers, which makes detailed analysis difficult. Further there is no breakdown in the document in relation to severity of hospitalised cases. My anecdotal information (which I can’t reliably corroborate) is that the majority of severe cases in ICU are unvaccinated or markedly obese and that severely ill vaccinated patients almost always have very significant co-morbidities.
This data really matters because it is now clear that there is a defined ‘at risk’ segment of the population susceptible to severe infection, and that for the vast majority of British citizens the virus really does pose minimal threat. That being the case, there can be no justification for any further restrictions on civil liberties with the attendant economic damage so clearly articulated by the Prime Minister in February 2020.
Graph Five shows daily Covid discharges on the blue bars displayed against Covid admissions and positive tests in hospital on the orange bars. Again, these numbers don’t really make sense to me – if there was this degree of disparity between admissions and discharges, one would expect the numbers of inpatients to accelerate at a much faster pace. There may be some double counting going on, or the definition of an ‘admission’ may also encompass patients seen in A and E and sent home without spending any time in hospital. Release of length of stay data could help resolve these discrepancies – such data does exist, but we are not permitted to see it. Readers may draw their own conclusions.
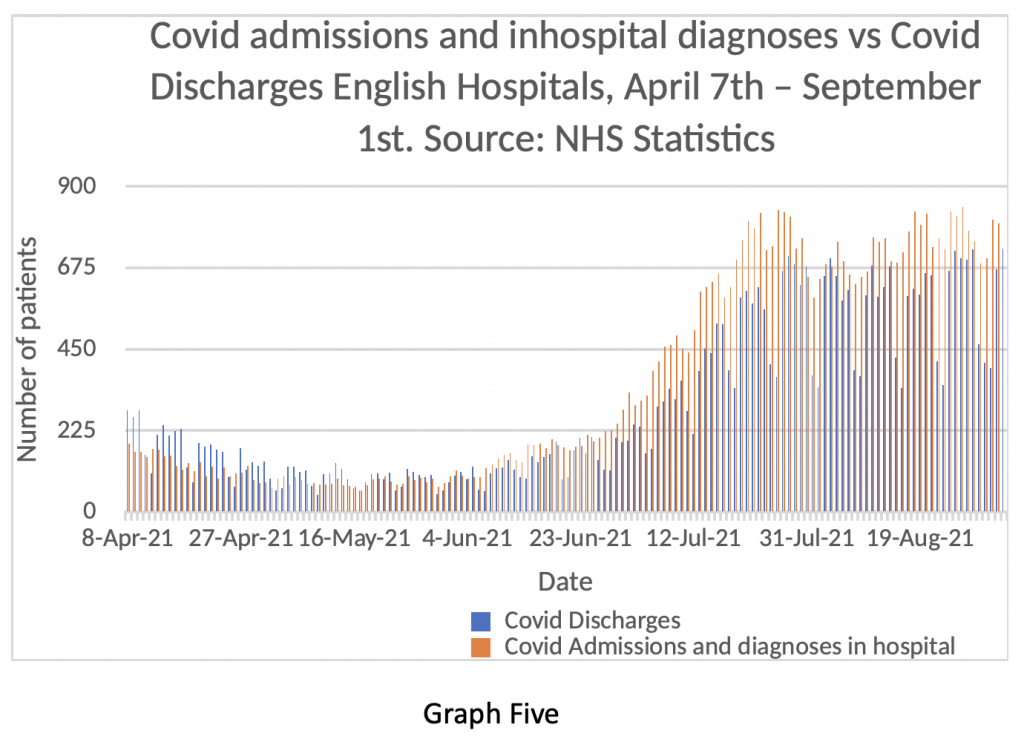
Once again, the ‘weekend effect’ can be clearly seen in the blue bar discharge data. Despite all the hype around seven-day working, the NHS doesn’t really function at the weekend. Maybe the extra £20 billion of taxpayers money might change that. Or maybe not.
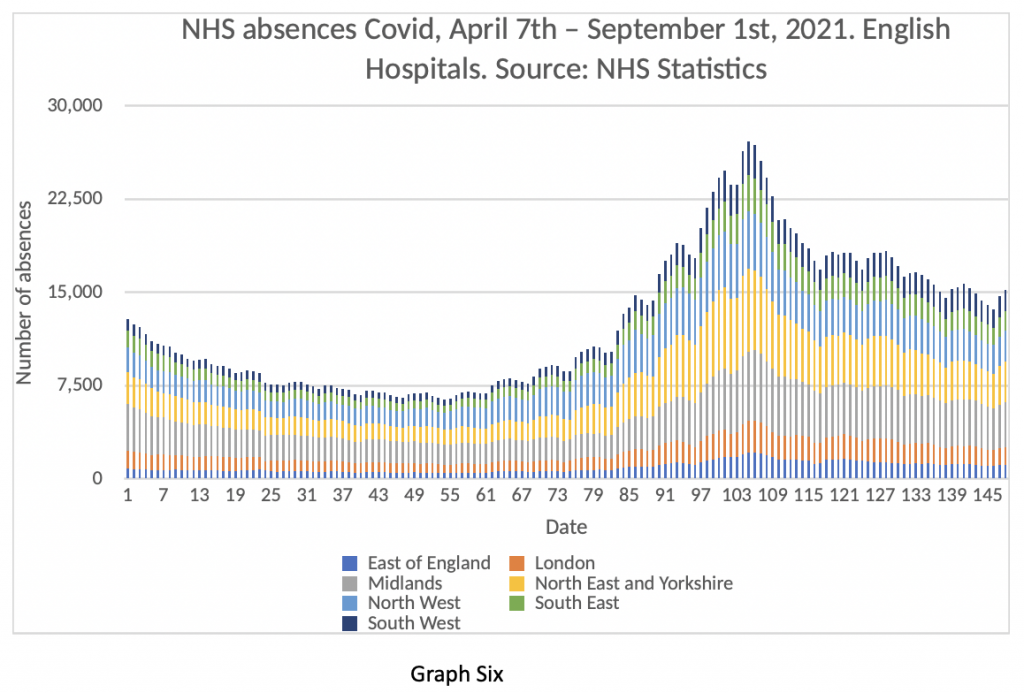
Finally in this update, readers may wish to assess Graph Six – the number of daily Covid staff absences in the NHS – still running at about 15,000 per day. The total number of staff off work every day for reasons of ill health is about 73,000.
So, what can we make of all this information? Well to be frank, it’s really quite boring. I could have written many more pages with charts of ICU patients and deaths and comparisons of real-world data vs. various confidently stated predictions from experts. They all show the same thing – no significant change in hospitalisations or deaths, or severity of disease for at least the last six weeks, despite the predictions of doom.
Does this mean the ‘pandemic’ is over? Again, to be candid, I simply don’t know. Further, I don’t think anyone knows. I have seen some well-argued pieces lately, particularly by Andrew Lillico in the Telegraph, analysing the herd immunity threshold in relation to the RO of the virus – his conclusion is that it is highly unlikely we will see a resurgent wave this autumn and winter. I sincerely hope he is right – time will tell.
In autumn 2020 we also had a gradual rise in cases which flattened out in late autumn before the Alpha variant took everyone by surprise in mid-December and kicked off the winter surge. Could this happen again in 2021? The difference this year is that we know vaccines have a significant effect on preventing hospitalisations. According to the Office for National Statistics, approximately 93% of adults in England have Covid antibodies either by natural infection or induced by vaccines.
There are two plausible ways in which Covid could make a resurgence in the same way as April 2020 or January 2021. The first is a novel variant which escapes vaccine induced immunity. The second is early waning of immunity induced by vaccination or natural infection. In the latter case, this should be detectable early and remediable by booster vaccines if needed. I note that Dame Sarah Gilbert recently commented that vaccine induced immunity seems to be holding up well and that, in her opinion, booster vaccinations should not be necessary for the majority of people.
It seems to me that we are now in the consolidation phase of the Covid episode, characterised by various professional groups striving to consolidate their gains over the last 18 months. Lest readers think I have adopted pretensions as a preternaturally gifted savant, I conclude this based on the behaviour of homosapiens over centuries. Humans have tended to pursue power, money and influence throughout the course of documented history and to exploit moments of crisis to accrue more of these things – I can’t see why this would change now. In detail I note that:
- The Government are demanding extension of emergency Covid powers to the middle of 2022 ‘just in case’. In other words, we continue to be governed by ministerial fiat, without parliamentary scrutiny on the pretext that we are in an emergency – the data does not support that argument.
- The NHS high command seems to have achieved almost complete ‘state capture’ and judging by this week’s announcement on raising NI contributions they now appear to be running the Treasury as well as virtually every other Government department. Spending on health and social care is expected to account for 40% of Government expenditure by 2025 and seems set to rise further – as the MP Marcus Fysh observed, the U.K. now appears to be a Health Service with a country attached to it.
- The various testing companies and associated paid advisors (some within parliament such as the former minister Owen Patterson who is paid £8,333 per month by Randox) will attempt to extend their activities into other infectious pathogens such as influenza, particularly if we have a significant flu outbreak this winter. The genetic sequencing firm Oxford Nanopore, a conspicuous beneficiary from the pandemic, has announced its intention to float on the London Stock Exchange, prominently advertising the potential profits still to be made from testing services in this and possible future pandemic threats.
- The unions, especially the teaching unions, are doing their best to prevent their members from actually doing any teaching on the grounds that interfacing with children is too dangerous for their members.
Most importantly from the consolidation perspective, the fear among the public must be maintained. Fearful people are more compliant and less likely to push back against arbitrary rule. The prospect of an imminent catastrophe must constantly be front and centre to ensure maximum benefit for the full spectrum of vested interests. Models will continually be adjusted to reflect the possibility of danger ahead – the woeful track record of predictions to date will be tactfully ignored by the mainstream press, to keep the confected risks in the public mind – danger and worry sells more papers than calm reassurance and sober assessment of the numbers.
The 19th century German philosopher Frederick Nietzsche commented in one of his essays that circumstances can arise where “the dead bury the living”. He meant that a false interpretation of history creates a situation where the living are too fearful to live fully, preferring instead to cower away, just in case calamity strikes. In this case, people are willing and indeed grateful to cede liberty and authority to centralised government in return for the illusion of safety.
The future is certain.










To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Oh dear: sounds all to plausible, and Boris getting more and more lunatic in his governance, a kind of Nero burning down the great city in the interests of what? The extension of government by fiat is intolerable, and so is the acquiescence of our only representatives in the polis, our MPs. On the state being now captured by the NHS, yes, again how true and grotesque. See article by Dr Smith in the DM today
As a complete aside. I’ve been wondering for sometime (time being the operative bit in that word) how you Sir managed to comment on this article 23 hours ago when I only received TDS at 0400 this morning (Sunday)? Presumably you had read this piece by 08:30 the previous day (Saturday)? Very strange. As I said I have been perplexed by this for sometime. Explanations please on a postcard to…..
They update throughout the day to prevent the poor loves having to stay up to 5am every day completely remaking the page.
CV isn’t and never was a problem for the NHS. However the “measures” take by the cretins running this country to ease the “burden” on the NHS mean that we know have record numbers on NHS waiting lists for every other treatment.
So there most certainly are problems with the NHS – just entirely different to those “predicted” relating to CV by the thick muppets like Ferguson.
Ferguson is not thick.
Nor are his errors accidental.
Yes, there is an almost wilful reluctance to accept what is patently clear. Ferguson works for Imperial, which has been sloshing around in the Bill Gates’s slush fund for a decade or more. Of course Boris Johnson, like Gates a lifelong eugenicist and depopulator, also does all that he can to further the planetary cleansing of the human hordes. Whether Johnson is or will be be paid for his services is not yet known.
I wonder why Jacob Rees-Mogg backed Boris Johnson then.
i would imagine the same reason Johnson hasn’t had a vasectomy: hypocrisy
Ha Ha! Top comment.
I don’t have any doubt that what he has done/is doing is deliberate, but he is thick to think that everyone would believe his BS.
He’s a thick, but bought, arrogant, vain POS, who fools no-one who is aware of his previous “work” and it’s consequences here in the UK.
Oh, I Do love these pieces of genuine analysis on this website.
So, well done.
The numbers are totally meaningless without some sort of baseline – ie How many people were in hospital with the “respiratory virus du jour” on the same dates in years prior to 2020?
and as for
It never even started.
“For example, on February 3rd, 2020, Boris Johnson, warned of the danger that “new diseases such as coronavirus will trigger a panic”, leading to measures that “go beyond what is medically rational, to the point of doing real and unnecessary economic damage”.“
Nice catch.
February and early March were the crucial period, and that’s the period future historians will need to focus on to try to understand the story of the 2020s social, political and economic disasters.
The scene was set with illiberal and intolerant trends throughout the US sphere from the late C20th onwards, with ever receding limits on the ability of corporate and individual wealth to manipulate opinion and government. But it was February and March 2020 when the battles were fought in which reason was defeated, setting the scene for the madness that has reigned ever since.
It’s no use, the covidians always just doggedly hold the view that any other course would have resulted in the doom predictions coming true!
They can’t get their heads around the idea that people might do so much for so little. There must have been a substantive threat (cause) behind all this they reason. Covidians fail to account for even the uncontroversial fact that the whole thing is based on predictions, not a response to actual events.
In short, they are mediocre thinkers.
The whole thing is based on a long predicted fraud.
Great article. Thank you.
Fully agree with your insightful conclusions at the end.
History is all about people seeking power under the cloak of moral virtue; and using fear as a weapon to get it.
The current era is no different.
It’s a fine article, but it’s trying to use facts and logic to refute cult zealotry.
The issue now is not about reality and reason, but simply about power, and who wields it.
It’s just for us, really. A dry voice of sanity analysing the stats we are given. A voice which is not propaganda.
“ it’s trying to use facts” – but which aren’t the ‘facts’ that they seem.
Figures on jabbed v unjabbed having higher deaths only expressed as ratios. … hmm …. no raw data on that released…. hmm…. or detailed breakdown on severity… hmm.
I thought so.
See my posting on the same issue. I’m sure others have noticed, too.
Yup, as the “doctor” pointed out – the key stats exist but they are not released.
TY/MC will you be putting a FoI request to the ONS for disclosure of the potentially inconvenient figures..?
What are the odds of the phrase “breakthrough infections” appearing in “official figures” this Autumn…?
It doesnt quite add up …..
A cursory glance over today’s Guardian website reveals that the “we’re doomed” philosophy is all pervasive throughout every strand of discourse.
Racism
Homophobia
Environmental degradation
Health services
Social care services
Trade
Brexit (natch)
Urban planning
Afghanistan
Vaccines
Every issue is portrayed as teetering on the brink of impending disaster. Given that the Guardian is the newspaper of choice of the clerisy and that these same people are most likely to be employed in the public sector or in academia, it stands to reason that this philosophical outlook will percolate through into their work.
In the absence of God, or stoicism, or rationality, fear and emotionalism will drive policy, worst case scenario disaster modelling will prevail. There is still no blowback in the media to the authors of disaster modelling that errs on the side of caution. Chicken Licken rules the roost.
The Groan is an appalling propaganda sheet now. But remember there’s plenty of other MSM publishing exactly the same crap.
Daily Mail is even worse with its relentless fear porn to drive the jab uptake.
Ofcom rolls as the puppet of the Cabinet Office.
Errata – that should have read “rools” as Molesworth would say
Is the good Dr saying that its healthy unvaxxed and only vaxxed obese and vaxxed with comorbidities in ICU
i had thought the virus and covid was mainly a threat for obese or/and very elderly and/or the peeps with comorbidities – vaxxed or unvaxxed
Is the Dr saying saying covid is now a threat for the healthy unvaxxed and is this not a new thing? (from the doc’s experience)
Yes – the ‘Good Dr’ is rather gloop blind.
A simple comparison with last year shows no mortality benefit in terms of all-cause deaths (even tho’ this will never be admitted in a situation where the jabs were predetermined to be ‘a good thing’ because of the sunk cost)
? which smacks of the “franking” of deaths from “other reasons” as CV19 – viz. no ‘flu deaths to speak of ? In other words Mortality Causation Syndrome – picture German Empire stamps overprinted with “billions” beyond face value; same thing but officially stamped as “something else”.
Use of Weimar Republic as precursor to NSDAP regime completely non accidental.
Thank you for your candour, which is a rare thing these days.
“In this case, people are willing and indeed grateful to cede liberty and authority to centralised government in return for the illusion of safety.”
Exactly! This has been at the crux of the matter for me. It is the most perplexing, infuriating and shameful thing of all, why have people given up their freedom to make personal choices based upon their own assessment of risk, so easily? This has burdened me from the very get go, I literally can’t get my head round it.
I do think things are starting to change, slowly, slowly in people’s heads. It’s a difficult thing to maintain, I would imagine, living with the thought that a killer virus is gonna get you every day of life. This is why so many people want to jab children. Human selfishness knows no bounds (Dawkins himself displays this regularly on twitter).
We have to keep trying to undermine the “no natural immunity” lies. They have gone in deep, and if you pull that thread alone, the lies unravel.
I can’t help thinking articles like this would carry more weight if we knew who this ‘doctor’ is. I get that s/he has bills to pay and a local clinical commissioning group to answer to, so doesn’t really want to ‘out’ her/himself. But this doctor clearly has a vaccine agenda. Quoting Gilbert claiming vaccine efficiency doesn’t make it so. Claiming ‘anecdotal evidence’ for covid patients all being unjabbed or fat and otherwise already desperately ill doesn’t make it so.
And it completely lost me at “The difference this year is that we know vaccines have a significant effect on preventing hospitalisations.” The ‘vaccines’, sorry, are doing the complete opposite. Ask any ward nurse.
I understand the need for anonymity. But, yes, the piece is very gullible on vaccines.
and very light on proven preventative early treatment to reduce hospitalisations even further to release the – numerically non existent – strain on the NHS.
And no nod to Israel, and how 2 vaccines aren’t enough there. Why would they be here? Is there something inherently different in the way the British react to the vaccines?
‘The difference this year is that we know vaccines have a significant effect on preventing hospitalisations.’
Do we know this? Perhaps there is another explanation for the decline in hospitalisations? That following two mild flu seasons, there were more vulnerable people in society (who ordinarily would have died in a hard flu season) who succumbed to Covid-19 initially, and once they died, far fewer people were left to whom the virus posed a serious threat?
‘..the Alpha variant took everyone by surprise in mid-December and kicked off the winter surge’.
And that just happened to coincide with the vaccine roll-out! Weren’t elderly patients then sent back to nursing homes where Midazolam was widely used?
I believe it can be argued that if the MSM hadn’t been used to drive a fear narrative, we would have thought a very nasty cold virus had arrived, which posed a threat to the old and vulnerable (as flu does each winter) and life would have gone on as normal!
But this isn’t a health issue and never was – it’s part of the ‘Great Re-set’ plan.
I think there would, however, have had a spike in elderly/vulnerable deaths – because of the accumulated ‘dry tinder’ susceptible to the appearance of even a moderate infectin.
Agreed – the two “cohorts” identified as most at risk…..apologies to you for stating the blindingly bleedin obvious
They should stop testing. It’s the only thing driving this madness and by using Ivermectin and HCQ in the early stages would have prevented many deaths. But most of us on here know this Virus was and always was politically motivated and by some revealing stories deliberately manufactured in a laboratory.
BD, agree 100%; latest unreacted Fauci emails reveal Daszak &Co including MS Zhengli (if memory serves me) confirming to other interested parties they had successfully created 8 chimeras from which two were genetically enhanced to have transmissibility as tested on humanised mice – and all those poor creatures who developed CV19 from the non naturally occurring spike protein induced by the backbone inserted at the turn cleavage site of these chimeras – died.
So a virus which originated in bats was genetically engineered with similar viruses in rats to produce a chimera pathogenically lethal to some humans – SARS COV 2 – which does not occur naturally in the wild; no trail of human transmission from the bat caves to Wuhan is ever established and that element is very quietly buried subsequently. Emails then sent to Fauci, cc’d to Drosten, Zhengli, Farrar, other European scientists, and one P.Vallance as head of R&D @ GSK at the time, from scientists who had examined the SARS COV 2 virus to find elements that were engineered “if you look deeply at the detail” ( my precis, not verbatim) . Fauci immediately kicks into action a Daszak controlled misinformation exercise, denies the virus was both manufactured in and “released” from …the WIV lab. Dazsak then is appointed to head an “investitigation”, since completely discredited as an exercise in deflection by the CCP and Chinese military, “lab leak theory discounted”, after a group of supine “experts” sign open letter published in that organ of truth and rectitude, The Lancet.
Fauci demonstrated to have lied, several times, to the US Congress about his agency funding GoF. Emails from Dazsak now confirm funding was sent to WIV via EcoAlliance using funds from Fauci. P.Vallance knows all about this as he has been “cc’d” in these emails but declared none of this when appearing at press briefings throughout 2020/21.
I cannot believe the UK/US/5 Eyes Intelligence Services are blind to all of this; if this information – and I don’t recall Daszak denying that the recent unreacted “Fauci” emails are genuine – is in the public domain, is not a gigantic “black ops propaganda” campaign for some reason, what else do they know – after all GCHQ and the US at Menwith Hill record every email – take a look at the server cable links under the sea… – and I have read information which hints that they also read WhatsApp type traffic – don’t believe the bleating from the Intelligence community for one nanosecond that they don’t have the means to do this….apparently it is very possible and there is precedent in eavesdropping technology in the past ( granted far less sophisticated than is capable now ) and perhaps why Nato is so concerned at Russian sub activity.
And “they” think we, the GBP, don’t “get” all this?…”Pandemic my arse”
Excellent summary. Biden is so deep in Faucism, his “dark money” backers must be the same guys running this show. Plus dark money from China.
“furin”. apologies
oops “redacted” too
For crying out loud. COVID-19 has a mortality rate in range with regular flu. The average age of COVID death is 82 years in the UK. There never was a health emergency, none of this was ever necessary, nor has it achieved ANYTHING worthwhile – ZERO BENEFITS ONLY DESTRUCTION. This is an agenda, coming from the very top, which is why all the laws are being over-ridden. Go try and publicly over-ride some laws yourself and see how far you get.
GOVUK came out on 19th March 2020 – BEFORE THE FIRST LOCKDOWN – and DOWNGRADED COVID-19 from a high consequence infectious disease, citing “LOW OVERALL MORTALITY RATES” as the reason. COVID is not, nor ever was, a super killer virus, we’ve all been conned, they’ve murdered a bunch of people on the wards by fast tracking them to mechanical ventilators and filling them up with Remdesevir. They killed people in nursing homes with Midazolam and they denied the real COVID victims access to safe and effective drug treatments. They even went to the extent of running sham trials to make it appear these drugs were unsafe. It’s genocide, plain and simple, wuith plenty to come, what with the ADE and cancer suppressors in the mRNA shots.
And this doctor, who is writing anonomously, cannot bring himself to admit that ADE is going to be an issue. Yawn. It’s clear that Toby has a “NO ADE” in the main articles policy, despite it being possibly the most important issue we face right now. This is controlled opposition, this is how it works, so it is up to people of integrity to get out there and inform the public of the real issues.
High consequence infectious diseases (HCID) – Status of COVID-19
https://www.gov.uk/guidance/high-consequence-infectious-diseases-hcid#status-of-covid-19
Professor Dr John Ioannidis confirms early in the scamdemic that mortality rate is in line with regular flu, which means all this destruction has been for nothing. It’s a shame that between this doctor and Toby Young, they cannot handle this.
BREAKING NEWS ! Prof Dr John Ioannidis Stanford University On Real Data On Coronavirus Pandemic – April 2020
https://www.youtube.com/watch?v=btvDL6kIDsA
The mRNA shots SWITCH OFF cancer suppressors, to be clear, so it’s likely there will be an uptick in cancer. How bad will it be – we don’t know, its an illegal, immoral, unethical, unlawful medical experiment with no long term data to inform us of such things. All jabbees are guinea pigs but they have not received informed consent – quite the opposite they have been lied to and told it’s all safe and effective plus bullied coerced and threatened into complying by these tyrants and criminals. It is as sick and evil as you can get.
I believe Dr Fleming set this out in his “Crimes against Humanity” presentation , among other revelations?
Thanks for that timely reference back to a document that should be in every rationalist’s armoury.
Excellent post, far more to the point than this article which still heavily relies on crap data born from the fraudulent PCR test.
Your comment that this site is controlled opposition becomes more apparent by the day unfortunately.
And let’s not forget that by declassifying Covid as an HCID post-mortems are no longer required.
Ah! That’s why they declassified… I missed that. Thank you.
A mixed bag of analysis, that is fine as far as it goes; there is certainly no health emergency (but never has been in actuality). This is a political crisis, and, indeed one run by the government with the collusion of the ‘top brass’ of the NHS, who are irredeemably politicized.
However, we still have analysis based on PHE and NHS data that is entirely flawed in its basis in PCR testing with ludicrous Ct levels and absurd time-frames. Although ‘incidental’ PCR+ findings are mentioned as a problem, the flaw doesn’t get the central place that it deserves as a health warning ( 🙂 )
i.e. this is knitting with spaghetti rather than wool.The flaws in PHE data that were scandalous last year have been only partially corrected.
The acceptance of ‘vaccine’ ‘efficacy’ from dodgy data is also very, very dubious, relying as it does on highly propagandized sources. Yesterday a bar chart (and other information) was presented here that puts the issue in an entirely different perspective. Remember this one? When adjusted for distortion, it gives a very different picture of the absolute risk of death with and without the jab :
Thanks for posting that graph again, but as the PCR test is involved, even that should be treated with caution!
And, even putting that caveat aside, there is no way of knowing how many of the unvaccinated dead weren’t able to take the vaccine because of an existing medical condition – and it’s that condition which has killed them, not Covid-19.
That data simply hasn’t been made available (as far as I am aware), so we need to maintain our sceptism in the light of all these sleights of hand.
You are absolutely right about additional reservations. But the point is, that even in PHE terms, when you put the data in perspective, you see the claims are utter distortions.
P.S. I keep looking at this bar chart, simply because, when you envisage the reality (instead of the distortion), the danger from Covid is shown to be so starkly minimal.
… and that’s starting from a PCR+ base – not the whole population!
RickH, are we not forgetting that the WHO reined back, more than once from their “Gold Standard” mass testing regime, effectively saying in at least two bulletins from 2020 that the (Cormen-Drosten RT-PCR scam) positive test result must not be relied on, must be separately ratified? Even Drosten, who detuned the WHO mass testing specification from 3 gene segments to one, always remembering that PCR does not and cannot test for the whole gene sequence never mind it does not distinguish between live or inert material, is quoted confirming that the test result in isolation cannot be relied on…”so why is it?” ( rhetorical..)
Perhaps TY/MC can prepare a timeline of these inconvenient truths as a link to enable perspective – I feel sometimes that significant revelations disappear from view as time goes by – I know Reiner Fuellmich is preparing a case on this but we non legal types need a reference guide constantly updated, warts and all?
Memories are so short. Glenn Greenwald has an excellent article on his site about compulsory vaccination and ACLU reports. The 2008 and 2021 reports are diametrically opposed. In 2008 the authors were concerned about liberty. In 2021 they are not.
In amongst comment based on some NHS data are the following passages;
”My anecdotal information (which I can’t reliably corroborate) is that the majority of severe cases in ICU are unvaccinated or markedly obese and that severely ill vaccinated patients almost always have very significant co-morbidities”
”The difference this year is that we know vaccines have a significant effect on preventing hospitalisations.”
”The second is early waning of immunity induced by vaccination or natural infection. In the latter case, this should be detectable early and remediable by booster vaccines if needed.”
If I was reading a typical article in say the Times and read these passages I would shrug to myself that its what you expect to read from an organ specifically trying to promote the ‘vaccines’.
In an article here, my reaction is that the ‘nudge’ unit would be proud of such a subtle way to inculcate their philosophy.
This Doctor may be a ‘lockdown’ sceptic’ but he is no friend of the wider sceptical thinking of the use of gene therapy injections.
Anyone noticed the MSM outcry about the last ludicrous modelling about disease levels made by the computer games industry?
No? I thought not.
Nor any mention of the flaws in previous fictional ‘crises’, such as last autumn, with its 6000 deaths a day.
I’m so surprised.
Why are the dates on the base lines of these graphs showing “25” and not “21”?
Planning ahead? Do they know something we don’t?
He is using the 1904 date system in Excel. It’s a Mac compatibility thing, plus, useful for some charting and formula.
There is a third reason — that covid is a seasonal disease with relatively low numbers of ‘more than very mild’ symptomatic disease during the summer. A bit like pretty much all upper respiratory tract viral infections. If this is the case then we could see problems emerge this winter (dependent on how well the vaccines are actually doing).
The pattern is not dependent on ‘vaccines’ – except in a negative way, with the gloop interfering with the expected decline to endemic levels.
The whole agenda is driven by modelling. Real world data shows this time and time again across the world
https://www.researchgate.net/publication/353837019_A_TALE_OF_TWO_SCIENTIFIC_PARADIGMS_CONFLICTING_SCIENTIFIC_OPINIONS_ON_WHAT_FOLLOWING_THE_SCIENCE_MEANS_FOR_SARS-COV-2_AND_THE_COVID-19_PANDEMIC
And if I am. not mistaken , that modelling mantra with additional code thrown in comes from….ICL/Ferguson and their cohort cronies, adopted by “gullible” administrations worldwide, who have never heard of the previous success of “The Swine ‘flu pandemic and modelling Affair”
Oh thanks heavens for that: no need to panic, the relief is immense!
Somehow the press missed this.
Data suggests that a messiah was reincarnated within the last month.
Perhaps after all we will soon experience the end of the world as we know it
Up to Aug 18th
The MHRA has received 508 UK reports of suspected ADRs to the Pfizer/BioNTech vaccine in which the patient died shortly after vaccination, 1,056 reports for the COVID-19 Vaccine AstraZeneca, 17 for the COVID-19 Vaccine Moderna and 28 where the brand of vaccine was unspecified.
Up to Sept 1st
The MHRA has received 524 UK reports of suspected ADRs to the Pfizer/BioNTech vaccine in which the patient died shortly after vaccination, 1,064 reports for the COVID-19 Vaccine AstraZeneca, 16 for the COVID-19 Vaccine Moderna and 28 where the brand of vaccine was unspecified.
Wow.
Sound of thundering hooves, a pale horse…
Hmmm… 40% of Government expenditure eh?
How much smaller could that be if, instead of chasing the game, the NHS actually were allowed to promulgate ‘good health’ by prescribing exercise and a good diet, and proscribing highly processed food-like substances?
There have been several good programmes on the broadcast media that have set out what should be considered healthy food and how much exercise is necessary – did anyone in Government take note?
Considering the amount of time wasted by local council Public Health depts on programmes for healthy eating, exercise and stopping smoking, I’m sure the govt considers itself above all that. Besides amazon (and other assorted dodgy factories/warehouses) and supermarkets would absolutely definitely collapse if they couldn’t force their staff to work 50+hrs a week, who needs exercise and good food when there’s profit and tax at stake.
Why are the horizontal axes of these graphs all labelled 2024 and 2025? Have I overslept? R. Van Winkle, Nuremberg
It’s the Excel 1904 date system. Used for Mac compatibility.
The point surely though is that the Global State is exceeding its powers and we do have lots to worry about. Objectively Covid may be somewhere between a bad flu and a hoax, but is it reasonable how they have acted? The state is either corrupt, thick, or tyrranous. Or all three. This situation is rightly perplexing because there is no end to the ramifications. We are watching the world as we know it being ended.
Superb article. Thank you.
‘State capture’. That is the truth and how vested interest in making money out of covid forces the Government agenda. Well at least Jacob Zuma in South Africa ended up in jail. Perhaps there is light at the end of the tunnel and we can see Fatty Boris doing some stir.
Does anyone else find the date format in these graphs incomprehensible? They appear to refer to 2025. Apologies if anyone else has picked this up..
What’s with the x axis of all these graphs? Why do we have the American dating system in one, why is it 2025, why are there no red highlights as described in graph 2 and why does the last one just count forward with no starting date. It’s hard to take seriously an assessment with such careless mistakes in it.
He is using the Excel 1904 date system. Prob data sent from a Mac to a Windows. The dates serial numbers are 4 years different.
Always interesting article from the inside of NHS. Appreciated. But the Israeli experience cannot be hidden. The vaccine immunity is rapidly falling and even with 3rd Booster in Israel 62 deaths after third shot in Israel in Aug. There is no way it could be different in the UK or other countries; it is just coming later depending upon the rollout of the vaccination programmes.
Why has not the hospitalization rate gone down in UK as in previous “unvaccinated” summer? Due to waning immunity of the vaccines, we have an ever-growing susceptible people in the community possible to infect for the virus, now mutated and with less morbidity but vastly more contagious (caused by mass vaccination’s strategy). The dry tinder effect means there are less very susceptible left but as this is now an endemic virus this will continue its path unrestrained by anything we can do.
The only caveat is if the influenza virus will return, and replace it, as it has in India, which seems to be the first country going into the endemic phase of C 19. We could have a winter flu which could be severe due to lack of influenza last year. Any NPI, TTT, vaccine, border control, and mass testing will not stop this natural passage of respiratory viruses,whether influenza or coronavirus.
That’s what the Faucists hope for – Covid plus winter flu. But unless it is a new strain, I don’t see how it could have a big impact given the dry tinder is gone and widespread immunity. I haven’t had flu since swine flu in around 2007 – my immune system has simply updated with each new variant. If the world hadn’t gone bananas, I would have said I’d had a nasty flu in March 2020 of course.
I am beginning to wonder about this alleged doctor – the unvaccinated are the ones who are sick in hospital when the data he refers to shows that in the most vulnerable and less vulnerable categories that proportionately, more double jabbed are in hospital …..I am thinking that this is a pro-vax doctor filling the missing and vague information gaps in a manner which feeds his bias
Perhaps because the data goes back to when few were vaccinated and the doctor has forgotten to take this into consideration …..
Ignore that, double checked but there is little difference between unvaxed versus the rest when u look
I’d like to see the guidance given to hospitals on fitting patients into categories for graph 4. It suggests 25 per cent of patients have not got serious Covid – is that unsymptomatic, by any chance? Or unsymptomatic and mildly symptomatic, ie not requiring oxygen because of Covid specifically?
There’s a lot of room for fudging there.
Fudging galore – NHS/ONS/PHE/SAGE/NERVTAG/JCVI etc fudge operation at full bore – whilst the NHS clinicians on the wards, CV and non CV, are burnt out since Jan 2020, GP fundholders go awol to count their cash, turn their own patients away to “Engage” or A&E, wind up their own trade union to selectively quote “Official” stats to show f2f appointments continue unabated – despite the actual experiences of desperate, sick people telling the exact opposite ( with full acknowledgement to those GPs who have not dumped their Hippocratic oath in the Sharps bin ). It ain’t following the older brigade of Consultants and others, not me – but it is sinking the “NHS working for you” mantra finally.
I hear ( from TOH, career NHS, so 100% accurate) that hospitals , not exclusively A&E teams either, regard GP fundholders as the devil incarnate and the degree of enmity generated by GPs is not resolvable….
oops again – “fooling” – IHPT!!!
On a long journey today the commercial radio station we were listening to had constant adverts about cancer, encouraging people to contact their GPs of they had symptoms because “your NHS wants to hear from you”. How we laughed… 🙁
“The difference this year is that we know vaccines have a significant effect on preventing hospitalisations. According to the Office for National Statistics, approximately 93% of adults in England have Covid antibodies either by natural infection or induced by vaccines.”
How do we know the vaccines are preventing admissions/ creating covid antibodies rather than existent immunity or immunity due to recovery? This data appears to come from blood donors (PHE latest report), presumbably on the basis of donor info as to whether or not they’ve been jabbed? Or does the immunity of one look different from the other?
People’s immunity is not tested (as it ought to be) before jabbing so we won’t know. The proposed timeline evidence for SARS CoV2 emergence is, according to US Gov House Foreign Affairs Committee, September 2019. This was followed in October by the Military (international athletic) Games in Wuhan. Athletes from around the world returned home, many reported to be ill. It is described as a super-spreader event.
https://gop-foreignaffairs.house.gov/wp-content/uploads/2021/08/ORIGINS-OF-COVID-19-REPORT.pdf
Therefore this virus, whatever it is, was doing the rounds from autumn 2019. The numbers of people exposed, infected, recovered before the lockdown measures of March 2020 is unknown, but potentially considerable given other extensive academic/business contacts between Wuhan and the rest of the world. If one were a conspiracy theorist one might suggest there is no interest at all in finding out who has existent/recovered (as in unjabbed) immunity. What happened to the promised T-cell tests?
why are the dates in the graphs relating to 2024/25?