
Public Health England (PHE) published their latest weekly vaccine surveillance report on Thursday. Usually these just summarise other studies so are not particularly interesting, but this week something new appeared that has been widely asked for but elusive: data on cases, hospitalisations and deaths broken down by age and vaccination status.
Although the fortnightly technical briefings on the variants of concern have a breakdown of sequenced Delta cases broken down by vaccination status and into the over-50s and under-50s, this is the first time PHE has published general data on all cases (not just sequenced ones) split up by age and vaccination status.
The data comes from the Second Generation Surveillance System (SGSS), the relationship of which to the Government dashboard data is unclear, though the figures are similar. It reports 722,728 cases in the reporting period, compared to the dashboard figure of 727,010 by specimen date, so this seems comprehensive. On the other hand, it includes 6,605 hospitalisations, whereas the dashboard has 21,242, more than three times as many, though this may be due to how it counts hospitalisations (“Cases whom [sic] presented to emergency care (within 28 days of a positive specimen), resulting in overnight inpatient admission”). It has 2,381 deaths, against the dashboard’s 2,496, so again this is most of them.
It is just data for the past month, August 9th to September 5th. We can use it to calculate a rough estimate of unadjusted vaccine effectiveness in different age cohorts for this four-week period.
However, the report itself cautions against using it for this purpose. It says: “The vaccination status of cases, inpatients and deaths is not the most appropriate method to assess vaccine effectiveness and there is a high risk of misinterpretation. Vaccine effectiveness has been formally estimated from a number of different sources and is described earlier in this report.”
These “different sources” are the various studies that are released by PHE from time-to-time, which tend to involve some heavy adjustments to the data and a number of other issues, and which consistently overestimate vaccine effectiveness compared to real-world data.
The report explains why the data should not be used to calculate vaccine effectiveness:
In the context of very high vaccine coverage in the population, even with a highly effective vaccine, it is expected that a large proportion of cases, hospitalisations and deaths would occur in vaccinated individuals, simply because a larger proportion of the population are vaccinated than unvaccinated and no vaccine is 100% effective. This is especially true because vaccination has been prioritised in individuals who are more susceptible or more at risk of severe disease. Individuals in risk groups may also be more at risk of hospitalisation or death due to non-COVID-19 causes, and thus may be hospitalised or die with COVID-19 rather than because of COVID-19.
This is claiming that the vaccinated are more likely to be in high-risk groups, which implies to me that a breakdown by other risk factors like comorbidities would be useful. However, now that most of the population is double vaccinated, particularly in the older age groups, this point would seem to be much less valid, so that the picture painted by this real-world data should be truer to the reality. In any case, let’s see what it shows.
I have calculated the unadjusted vaccine effectiveness against reported infection, hospitalisation and death for each age group and also for the under- and over- 50s.
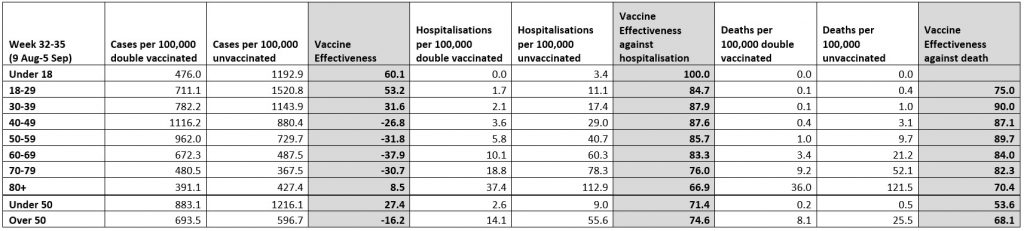
Strikingly, during this four-week period the vaccine effectiveness is negative in all the over-40s age bands except the over-80s – the vaccines seemed to make things worse, with the vaccinated having disproportionately more infections than the unvaccinated. For 60-69 year-olds it hits as low as minus-38%. This makes a nonsense of vaccine passports or any measure based on the notion that vaccines prevent infection.
One factor in this will be that, as we know from the technical briefings, the vaccinated curve rose and peaked later than the unvaccinated curve, which will have exaggerated vaccine effectiveness initially and underplayed it later. A longer period than the last four weeks would therefore be useful to take into account this unexpected phenomenon.
The vaccine effectiveness against hospitalisation and death is still looking pretty good. One thing worth noting is that the vaccine effectiveness in the larger age brackets of over- and under- 50s can be lower than it is in each finer age band. So the vaccine effectiveness against death in the four age bands over 50 is up at 89.7, 84, 82.3 and 70.4. Yet in the over-50s group when taken as a whole it is only 68.1%, lower than in each of the individual age bands. This is an odd quirk that occurs because of the big differences in risk between the age bands, so that as the very high number of deaths in the highly vaccinated over-80s are mixed in with the deaths in the younger age groups the overall effect is to depress the vaccine effectiveness. This means the more age-specific values may give a more accurate guide to the true effectiveness of the vaccines than those from the broader age cohorts. Interestingly, for effectiveness against infection in the over-50s the pooled value is higher than the value for the separated age bands, though is still negative at minus-16.2%.
Looking at the proportion of reported cases and hospitalisations which are vaccinated and unvaccinated, overall 39% of reported cases are double vaccinated versus 35.4% unvaccinated. In the over-50s, 82.6% of reported cases are double vaccinated versus 7% unvaccinated. For hospitalisations, overall 48.9% are double vaccinated versus 43.8% unvaccinated. In the over-50s this is 69.2% double vaccinated versus 26.7% unvaccinated. These statistics give the lie to any claim that it is the unvaccinated who are primarily spreading the disease or being hospitalised with it.
Having said this, 71.1% of hospitalisations in the under-50s are unvaccinated versus 16.5% double vaccinated. Also, 38% of total hospitalisations (2,538 out of 6,605) are in the under-50s, so this is not a small number. However, it’s worth noting that only 6.7% of the deaths are in the under-50s, so these hospitalisations are considerably less serious than the 62% of hospitalisations in the over-50s.
It’s good that PHE has finally released data broken down by age and vaccine status, even if only for one month.
Here’s a radical suggestion for PHE: why not make all the data publicly available so people other than the chosen few can analyse it for themselves and get a fuller picture?
This post has been updated.
Postscript: This article was subjected to a fact check by Full Fact who found it was “incorrect”. You can read that fact check here and Will Jones’s response here.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
No surprise. Covid has shown the medical profession to have been bought. lock, stock and barrel
What is HPV ?
https://www.nhs.uk/conditions/human-papilloma-virus-hpv/
Thanks 👍🎄
Hocking another unnecessary pointless vaccine for harmless virus!
You mean another unnecessary harmful and occasionally deadly vaccine for a harmless virus…
https://childrenshealthdefense.org/defender/merck-hpv-gardasil-vaccine-adverse-event-database-court/
Some of the signature impacts observed following HPV vaccination — which afflict a number of the plaintiffs — include permanently disabling autoimmune and neurological conditions such as postural orthostatic tachycardia syndrome (POTS), fibromyalgia and myalgic encephalomyelitis/chronic fatigue syndrome, The Defender reported .
There have been thousands of reports of adverse events worldwide, peer-reviewed scientific literature from the U.S., Australia, Denmark, Sweden, France and Japan, and statistics published by public health agencies in each of these countries that demonstrate plausible associations between HPV vaccination and autoimmune conditions.
Sound familiar?
They must have been Banksy-style data that erased themselves as you read them. Or maybe the dog ate them.