
A member of SAGE warned back in February that the return of unvaccinated children to the classroom would create a “significant risk of a resurgence” of Covid infections. This was not the case – only 0.06% of rapid Covid tests of students produced positive results in the week that schools reopened. But how many of these results were actually positive? Professor Jon Deeks, a biostatistician from the University of Birmingham, said in March: “We would expect far more false positives than true positives amongst those testing positive in schools.” New data from the Department of Health and Social Care has now confirmed that more false positive results were produced than true positives in the first two weeks of school testing.
This data, as Professor Deeks points out, is a damning indictment of the use of rapid Covid testing in schools and has resulted in many children having to isolate at home unnecessarily – with their classmates often being sent home too. (At one stage, more than 200,000 schoolchildren were having to self-isolate, forcing them to miss out on much-needed catch-up work in classes.)
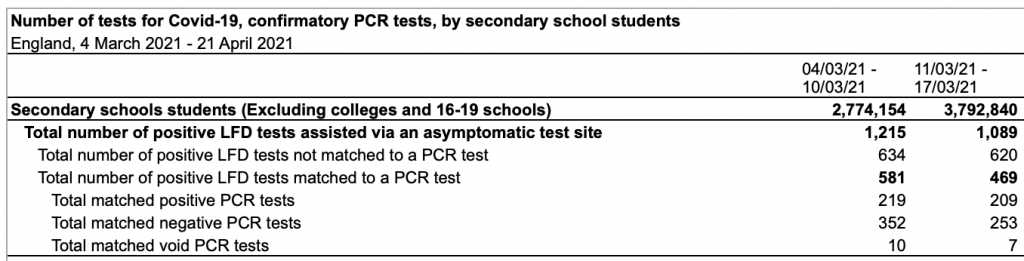
[The] proportion[s] false were 62% and 55% in these two weeks.Of 2,304 positive tests, 1,353 were likely false, with one positive per 6,900 tests done.
The use of PCR tests to confirm or (in more cases) deny lateral flow test results is itself a strange choice, as Lockdown Sceptics’ Will Jones points out, and could mean that the true impact of rapid testing in schools is even worse than this data suggests.
It is interesting that they assume confirmation from a PCR test defines true and false positives, even though PCR tests are more sensitive than LFTs so are no less likely to give a positive from fragments or contamination. What if in some cases the PCR tests are just confirming the false positive of the lateral flow tests?
The British Medical Journal has been warning against the use of PCR tests for “case finding, mass screening, and disease surveillance” since last September (if not before):
PCR is not a test of infectiousness. Rather, the test detects trace amounts of viral genome sequence, which may be either live transmissible virus or irrelevant RNA fragments from previous infection. When people with symptoms or who have been recently exposed receive a positive PCR result they will probably be infectious. But a positive result in someone without symptoms or known recent exposure may be from live or dead virus, and so does not determine whether the person is infectious and able to transmit the virus to others.
Clearly, testing requirements for schools must now change. But the problem is not limited to the classroom. Professor Deeks says that false positive data should now be released for all forms of lateral flow testing.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
testing should be voluntary and the testee should pay themselves. would stop overnight
The whole regime has been a right load of testees from start to finish.
Testee-cles.
The PCR test produces false positives
Who knew?
(Other than every single fecker on here for the past twelve months)
All test produce false positives. No one denies this. The PCR tests have an extraordinarily low probability of a false positive – the absolute maximum is about 0.2% and it is probably much lower. We know that for certain because that is the percentage of positive results we get out of all tests when virus levels are very low.
Utter bollocks. This might be true if you were testing 1,000 people in low prevalence. But they are testing 1.5 million. Therefore the fpr is more like .8% could be as high as 4%. This test was never meant to be used for this and is not fit for purpose. The ONLY people who should be tested are people who feel sick.
I propose an epidemiological study. Identify a large sample group of people who suspect they had COVID before February 2020. Ideally, this would be individuals who had signature COVID symptoms, went to a doctor because of these symptoms, got an influenza test … and tested “negative” for influenza. (BTW, there is no shortage of such people).
Next, identify what percentage of these individuals subsequently tested “positive” for COVID/the virus with a PCR test.
Hypothesis: If a disproportionate percentage of these individuals have not subsequently tested positive for COVID, would this not qualify as compelling evidence that these people had acquired natural immunity to the virus … before the virus was even supposed to be spreading?
Somehow I don’t think such a study will be commissioned. Which in my opinion is a “tell” about how sincere “public health officials” and infectious disease experts really are when they tell us they are very interested in investigating the possibility of “early spread.”
I have about 1,500 Facebook “friends.” From posts on my Facebook page, I solicited feedback from people who suspect they may have had COVID before February 2020. (Or if these individuals know close friends or family members who meet this profile). I also have spoken personally to some people who fit this description.
From these solicitations, I identified at least 50 people who think they might have had COVID before the lockdowns.
About two months ago, I followed up with most of these people (some didn’t respond to my inquiry). From this follow-up, I learned of two (2) people who thought they had COVID pre-February 2020, but later did test “positive” for COVID. So, these people probably did NOT have COVID.
However, of the balance (close to 50 people) none had later tested positive for COVID.
We now know that about 11 percent of the people in my state (Alabama) have developed “confirmed” cases of COVID.
Per my “study,” only about 4 percent (2 out of 50) of those who thought they’d already had COVID did test positive at a later date. Four percent is a lot less than 11 percent.
Plus, we all know that a lot more than 11 percent of the population has now contracted the virus. Even conservative estimates say that 20 to 33 percent of the population has actually had the virus by now ….And 20 to 33 percent is a huge increase over 4 percent.
I’d also note that my hypothesis does not state that everyone who “thinks” they had COVID actually had it. I’d even say that most people who think they might have had COVID pre-March 2020, probably didn’t. Still, if even 10, 20 or 30 percent of the “sick” people from November 2019 through February 2020 – people who tested negative for influenza – actually DID have COVID – that’s a LOT of people (The CDC estimates that as many as 55 million Americans had an “influenza like illness” in the “flu season” of 2019-2020). In short, what I’m describing could be our real “first wave” of COVID.
And I do think a REAL epidemiological study that questioned likely/possible “early cases” to see if they subsequently developed a “confirmed” case of the disease would be a smart way to further test this hypothesis.
If, say, 90 percent of this “possible early spread” group did NOT later develop COVID – what other conclusion could one make other than many of these people likely (or very possibly) did have acquired immunity. Which many of these people (I’m one of them) might still have today.
… One should also not rule out the possibility that at least some number of people who have good reasons to believe they had COVID pre-February 2020 … and who later DID “test positive” for COVID … could have contracted the virus for a second time.
We really can’t know the true “re-infection” rate because our baseline that gives us this answer didn’t start until PCR tests were widely administered. And no one got a PCR test before February 2020.
Given that even T-Cell and B-Cell “immunity” is believed to last 8 months (or longer) for “most people,” this “protection” would have expired in some people if they had, in fact, been infected in, say, December 2020 … and then tested “positive” in say, December 2021 (12 months later after immunity may have “lapsed.)
FWIW, I DO think more people have been “re-infected” by now than the experts believe.
Another footnote to my hypothesis and proposed study: People CAN have influenza and COVID at the same time. Plenty of studies prove this. Thus, at least some people who were sick pre-February 2020 and DID test positive for influenza … may have also had COVID.
… In fact, I KNOW some people had COVID and influenza at the same time.
I wrote the feature story linked below on Tim McCain from Sylacauga Alabama who had ALL of the COVID symptoms in December 2019. In fact, he almost died from what I’m sure were complications of COVID in the first week of January 2020 (which would have made him the first “known” fatality in America).
But Tim also tested positive for influenza. As my research for this story revealed, there are/were plenty of other cases of critical COVID patients who also had tested positive for influenza. (Tim later tested positive for COVID antibodies).
His wife, who also became sick when he did, has now had FOUR positive COVID antibody tests. She also was tested for influenza at the time, and this test was “negative.”
I’d add that state health officials and CDC officials have never contacted the McCains about their almost-certain early cases. And they know about them because Brandie McCain and myself called and emailed them many times, pretty much begging public health officials to investigate their likely early cases. Crickets.
https://uncoverdc.com/2020/06/25/an-alabama-man-nearly-died-from-covid-19-the-first-week-in-january/
Bill – the data on Covid is irretrievably corrupted. One can only speculate. In the UK all that is reasonably certain is that the mis-attribution has been massive.
Let’s face it – most people don’t know the difference between SARS-CoV-2 and ‘Covid’ illness.
I agree and subscribe to the views of the author published a couple of days ago at this site who opined that damn near everything we know about COVID … is wrong.
For me anyway, at the top of this list is the still unanswered question of when the virus actually began to spread and how “prevalent” this virus spread was in the weeks and months before we went into lockdowns (to prevent or slow said spread).
That is, the “conventional wisdom” on the “start date” of virus spread is definitely wrong. The inferences or implication that flow from this would be/are myriad and seismic.
With any investigation or research project, where does one begin? At the beginning … or one attempts to begin at the beginning. That is, establishing a likely chronology of events is crucial.
Well, with COVID, the “start date” (of wide spread) is almost certainly wrong. So every conclusion that flows from this bogus assumption might very well be wrong.
To cite just one example: Much has been said and written about how many world inhabitants have contracted this virus by now. However, all (or most) of these models assume that the virus began to spread widely around December 30, 2019 – and that “case zero” was probably in one city in China.
Well, what if the virus was already spreading in November, or October 2019? Wouldn’t more people have contracted the virus, and thus be expected to have acquired natural immunity?
If the entire purpose of the lockdowns was to stop or slow the spread of the virus, would this even be possible if MILLIONS of people in your country already had the virus when these lockdowns commenced?
I could go on an on. As readers of my posts on this topic can no doubt tell, I believe “early spread” is the “elephant in the room” of the entire COVID narrative.
There was certainly some new virus circulating pre-Xmas and afterwards until early March, not flu and not a cold. I had it, which left me with a dry cough for two months. Far more people that I know had that than the classic CV19 symptoms. Whether it was actually CV19 or not I don’t know.
I had “something” that wasn’t the flu in late January 2020. My symptoms were classic COVID, including acute shortness of breath, lingering dry cough, fatigue and loss of smell and taste.
I did get an antibody test in mid-May, which was negative. However, since I’d learned that COVID antibodies are basically undetectable in most people within two months I don’t think this “negative” antibody test can rule out the possibility I had COVID.
I can also report that I never have tested positive for COVID since (and my wife, who I slept next to every night) did. Anecdotal “evidence” I know, but I’ve heard from a lot of other people who thought they had COVID who have also never tested positive since.
For my entire life, no medic has been even faintly interested in any cold / cough / flu / respiratory illness presented to them, even if you’d been hacking away for a month and could barely crawl through the door. Just a virus. Something going around. It’ll get better. You were lucky if anyone peered at your tonsils or got a stethoscope out, mostly you got sneered out of the doc’s office as an ignorant timewaster. Even when a relative died of a chest infection, denied a doctor’s visit. You carried on, ops normal, went to work, and nobody ever thought anything of it. Now, they want to test you even if you’re not bloody ill!! Not only that, the message is that us ghastly biologicals are all walking health hazards to the herd and must be tagged and tracked from the cradle to the grave!
It’s sinister, illogical, crazy, and feckin’ expensive, probably to the extent that we can’t earn enough to pay the costs of this nightmare. We’re enslaved.
So much for the Modern Slavery Act, when did we become owned and managed by health care providers?
I reckon I had corona Feb 20, when the skiers came back. Nasty little cough for a few days. Kept working. On the other hand, I got a classic viral peel a couple of months ago, so maybe that was it. Who knows, who cares. Never been tested, not going to. Just another bug.
“Something going around. It’ll get better.”
… which was usually the case. A genuine problem for health services has always been hypochondriacs spreading minor infections via doctors’ surgeries.
“Kept working”
… and that was your (common) mistake. A short period of staying away is all that’s needed to cut down spread. The ‘soldiering on’ mentality is the opposite pole to hypochondria. Neither are a good idea.
I was in the “keep working” camp, unless I was so ill I could hardly move (rare). I would think twice about that now, for various reasons. Though I do wonder if some exposure to what’s going round has benefits as well as dangers.
I read somewhere that re-exposure to chickenpox as an adult, ie when your kids or grandkids get it, leads to less likelihood of developing shingles.
Epidemics are caused by people who won’t go to bed when they should.
And people who go to bed when they shouldn’t.
I rarely go to a doctor (maybe 3 or 4 times in 30 years) for respiratory illness, when I went it was really bad, and not being a frequent attender expected them to take an interest. The 4 month hacking cough was debilitating, although with hindsight it was probably whooping cough. I’d go into work with a sniffle, but not if it made me want to lie down. I know you can’t treat viral illnesses, except with megadose vit C and good nutrition to help your system fight it off.
Regarding my efforts to get some “public health official” or mainstream journalist to at least investigate these likely “early spread” cases, I feel like I’ve plunged into Alice’s Rabbit Hole.
No one will follow-up, look into or write about the mountain of evidence that supports early spread. Elsewhere on this site you can see my links about people who were sick with COVID symptoms in November and December 2019 and later got positive antibody tests(plus my link to the Red Cross blood study).
But the strongest evidence of early spread is the MILLIONS of people who were sick with “something” (something that was NOT influenza) … especially between December 2019 and through January 2020.
I’ve actually saved hundreds of posts from readers (made in Reader Comments sections) that describe their symptoms and explain why they think they may have had COVID. If you read any of these accounts, you will see that many of these people describe symptoms that were different in some ways from these people’s past bouts with the flu (or other bugs). Significantly, most report that they DID get tested for influenza and these test results were “negative.”
The painful, “dry” and persistent cough, the shortness of breath, the extreme fatigue, the loss of smell and/or taste, etc. are symptoms that these people did not experience to this level or nature during previous illnesses.
Again, I’m not saying that all (or even most) of these people had undiagnosed cases of COVID. But I am saying that some percentage of these people who were sick with obvious COVID symptoms almost certainly had COVID. Maybe this percentage is 10 percent, maybe it’s 30 percent. (I know of one doctor who believes the figure is “30 percent.”) Whatever the actual percentage, in the aggregate, MILLIONS of world citizens probably had COVID in the weeks and months before the lockdowns.
Furthermore, I find it impossible to believe that at least some “public health officials” didn’t know this, or at least strongly suspect this by, say, March 2020 (if not earlier).
Basically, I am saying the almost certain “early spread” of this virus has probably been covered up. I support this view by citing examples from my own reporting where I personally told public health officials about individuals who almost certainly had the virus in December 2019.
If CDC officials are/were sincere when they said (as they did in a May 2020 press conference) that they were continuing to actively investigate possible cases of early spread, they would have spoken to these people and pronto. They did not and have not … Even when provided specific and copious details about these possible/likely early cases.
Today, Watergate is considered the greatest “cover-up” scandal in American history. Well, what if we found out that at least some public health officials KNEW this virus was spreading – and spreading widely – throughout America (and the world) months before the lockdown … and never revealed this to the public?
What should or might qualify as a major scandal is, in fact, a nothing burger – another topic that’s “off limits” to real investigation.
What happened to the mysterious “vaping pneumonia” reported in the US back in summer 2019? That sounded like corona, with 20/20 hindsight.
still no 3rd wave in europe – someone’s bullshitting me!
https://euromomo.eu/graphs-and-maps/
Europe 3rd wave: ancient history
South African variant: ancient history
Brazilian variant: ancient history
Kent variant: ancient history
It’s all about India now.
Which is ironic because do you know which country tops the table for weekly COVID mortality per capita?
Hungary.
India, meanwhile, is in 62nd place.
covid ‘deaths’ in India 2000 per day. Barely a rounding error in a population of 1400 million and 27,000 all cause daily deaths
2000 die a day from diarrhoea – day in, day out for year after year – not this few weeks like covid. and that genuinely is kids rather than geriatrics – rather more QALYs involved
poor Hungary with no excess mortality.
No Surprise, They Have An Excellent Vaccination Program.
Talking bollox is your speciality and you get paid for it.
Oh – so that explains why they have such a high death rate!
Drove past my local testing centre today. It was totally deserted apart from a bored looking guy on the gate.
We have 3 near where I live, and never anyone in there. Unsurprising when our north west city is recording around 15 positives only or less a day.
The treatment of our children over the last fifteen months has been a disgrace to the country and its future.
There are many who should hang their heads in shame. Let’s hope our children are more magnanimous and don’t cancel pensions in a fit of pique once they get control of the levers of powers.
Frankly though I wouldn’t blame them if they did.
Bit off topic, but I thought I would share the latest news of the EU travel passport which was voted on today. It going to be called the EU COVID19 Certificate, and expires in 12 months. On a digi or paper record will be vaccination and/or test and/or antibody info. However , partly I think because of the Irish ‘border’ problem and the Schengen rules the following statement makes it clear that they cannot be used to stop freedom of travel.
Which makes a complete mockery of the whole thing, but that is good.
Testing must be universal.
About time, but what will it really mean, and from when on?!
As the article indicates, suggesting that PCR tests provide a sane alternative is nonsense.
STOP ALL TESTING!
Now!
And for good!
Test procedures don’t want changing, they want burying a thousand feet deep, and Wankok and his evil minions along with them.
latest PHE report just out
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/982289/Weekly_Flu_and_COVID-19_report_w17.pdf
page 61 for all cause daily mortality – still unbelievably low by all accounts
Only losers get tested.
“It is interesting that they assume confirmation from a PCR test defines true and false positives, even though PCR tests are more sensitive than LFTs so are no less likely to give a positive from fragments or contamination. What if in some cases the PCR tests are just confirming the false positive of the lateral flow tests?”
Why has this been downvoted? We know the PCR has incredibly high specificity, that’s the whole problem with it. It picks up literally anything no matter how tiny. Also, while they have false positives, the chance of two separate tests picking up a false positive on the same sample is very small. It seems from the data here that the false positive rate on LFT might be 1 in 2,500. On PCR, it’s likely about 1 in 1,000, very difficult for it to be much higher based on current figures. It’s possible but let’s use this as a ballpark for illustrative purposes.
So if you test 1,000,000 using PCR, as we are doing, you will get 1,000 false positives. This means that when you only have around 2k positives a day, as we are doing, at least half of them will be false. It’s entirely worthless to use in this fashion because a 0.1% false positive rate actually makes the test of no value when prevalence is this low.
However using it to confirm LFT results actually does have value. First of all, if a PCR says you’re negative it’s probably a good bet that you really are given the PCR even picks up old dead viral fragments
In the case of proving how worthless the mass testing is, the high specificity of PCR actually helps us. It means we can say with some confidence those positives picked up on LFT but subsequently PCR negative were false.
Also, if the LFT FPR is 1/1000 as it appears and the PCR rate is 1/2500, the maths tells us the chance of both producing a false positive on the same sample is about 1/2,500,000
I think. Happy for someone to proofread my sums.
The Government Must get their hands OFF our children. They will Plan to take off masks for School vaccinations by Sept. ATROCITIES
So yet again sage are fucking wrong by a significant factor. Where is the fucking outcry. Why are they permanently given a free pass? Every one of their models have been miles out and still this shit government uses these figures. They still are saying a third wave in summer. WHY? This is obviously wrong and we can prove that by looking at what happened last summer, not only do we not need a model we don’t fucking need sage.
Why is this country testing so many everywhere??? Just trying to spend as much of your hard earned money as possible. Wouldn’t it be nice if the friend you know could get their long awaited knee, hip, hernia, cataract surgeries. No sorry we are too flipping busy spending your money on unnecessary swab tests.
https://www.restoretheculture.com/?r_done=1
Truth over Fear Summit ll
free 3 days finishing sunday or £ premium for extended viewing.
40 speakers.