There follows a guest post by Dr Ros Jones, a retired Consultant Paediatrician and member of HART.
We have heard a lot in the last few weeks about Yellow Card reports for any adverse effects of vaccination, so I shall seek here to give a little background to the system and where it can work well but where it can seriously fall short.
The Yellow Card system was introduced in 1964 following the thalidomide disaster as a way of formalising the reporting of adverse effects, especially for new drugs. Tear-out cards, printed on yellow paper, were inserted at the back of the British National Formulary (BNF), which acts as the bible for UK prescribing. This book, updated twice yearly, was given to every practising doctor. Any doctor or pharmacist seeing a patient with unexpected symptoms relating to a prescribed medicine could quickly complete one of the cards and send it to the regulatory authority. But already you can spot the problem here – the system depends on the health care professional recognising that the symptom might be related to a particular drug, so if the connection is not made then neither is the report. Take for example a busy orthopaedic SHO treating an elderly lady with a fractured hip. Will they think to report this as an adverse reaction to her blood pressure tablets? This matters. Studies show up to one third of hospital admissions are due to iatrogenic causes i.e., drug side-effects. Nowadays, the BNF is an online book and the Yellow Card system is also online, so perhaps even more ‘out of sight, out of mind’, especially if the ward is really busy at the time. If you ask colleagues whether vaccine adverse outcomes have been reported to MHRA, they often reply: “I’m not convinced it was the cause, it could have been due to anything.” But physicians are not responsible for deciding whether a clinical event was caused by a drug or was coincidental – that is the role of the MHRA.
All new drugs and vaccines are subject to trials, starting with animal trials usually involving a number of different species, then building gradually through small pilot studies on humans to establish dosage regimes (for example) and short term safety, before rolling out to large scale trials looking for both efficacy and longer term safety. In such trials, all adverse outcomes will be reported, with the control group acting as the base-line for any symptoms against which the new drug is compared. The system works well for reasonably common side-effects and here the size of the trials is important. You will see in drug information leaflets side effects listed as “very common: affecting greater than 1 in 10 people”, through to “very rare: affecting less than 1 in 10,000”. Generally speaking, “very rare” side effects are only listed if severe. Many drug and vaccine trials are only large enough to detect “uncommon” side effects and for any new drug it is only through post-marketing surveillance that rarer side-effects can be discovered. New drugs are marked in the BNF with a black triangle for two years, to remind doctors to complete yellow card reports. In addition, most drug trials will exclude certain groups – for example children, pregnant women and people with risk factors such as kidney and liver disease, so safety for these groups is very much dependent on animal studies or assumptions from other similar drugs. Species difference in adverse effects may occur too, so damage to the developing foetus may only be seen after a drug starts being used by humans. Certain age groups that are under-represented in trials, such as the very elderly, may also be at greater risk. If post-marketing surveillance reveals an unexpected problem then the drug licence may be withdrawn or modified (e.g. limited to certain age groups, as with the AstraZeneca vaccine).
Where an adverse event comprises something very rare, it may be obvious to the attending physician (or indeed the regulator) that this is a potential drug effect. So for example, thalidomide caused a limb-shortening birth defect, phocomelia. This was totally new to the obstetricians and midwives of the day, so it was quite quickly realised that this was a teratogenic effect. But because of the time lag between drug ingestion in early pregnancy and the discovery of the harm, despite withdrawing the drug, over 10,000 babies were affected across Europe. Turning to the recent concerns raised with SARS-CoV-2 vaccines, cerebral venous thromboses (CVT) are rare. A general physician might only see one case in several years, so when a number were reported, it soon became apparent that they might be linked to the vaccine. But if the side effect is a significant increase in a common condition, it may be much less obvious. An elderly patient admitted with a stroke would not ring alarm bells but if suddenly a lot more people were dying in a two-week period after receiving a new treatment, then this could be highly relevant. Another concern for the vaccines is that they have been granted a temporary licence ahead of the long-term safety reports. Over time, many of those volunteers in the control arm of the trials will have received a vaccination and the power of the randomised controlled trial in terms of assessing safety will be greatly reduced.
So what does a prescribing doctor make of all this? We are taught, “first do no harm”. This does not mean you cannot prescribe a drug with known side-effects (that would rule out most effective treatments!), but it does mean that you have a duty of care to consider the patient in front of you and make a judgement on the balance of risk, i.e., do the likely benefits of this drug outweigh the potential harms? With vaccines, this is made more complicated by the fact that the person in front of you is not ill. Thus, you are weighing up the benefit of preventing severe disease or death from a condition which they may or may not catch (indeed against which they might already have immunity) versus a risk of a significant adverse reaction. Clearly this calculation will be different according to susceptibility to the disease in question, so for SARS-CoV-2 vaccines, a safety threshold for a healthy young adult let alone a child would be set much higher than for a 75 year-old with diabetes.
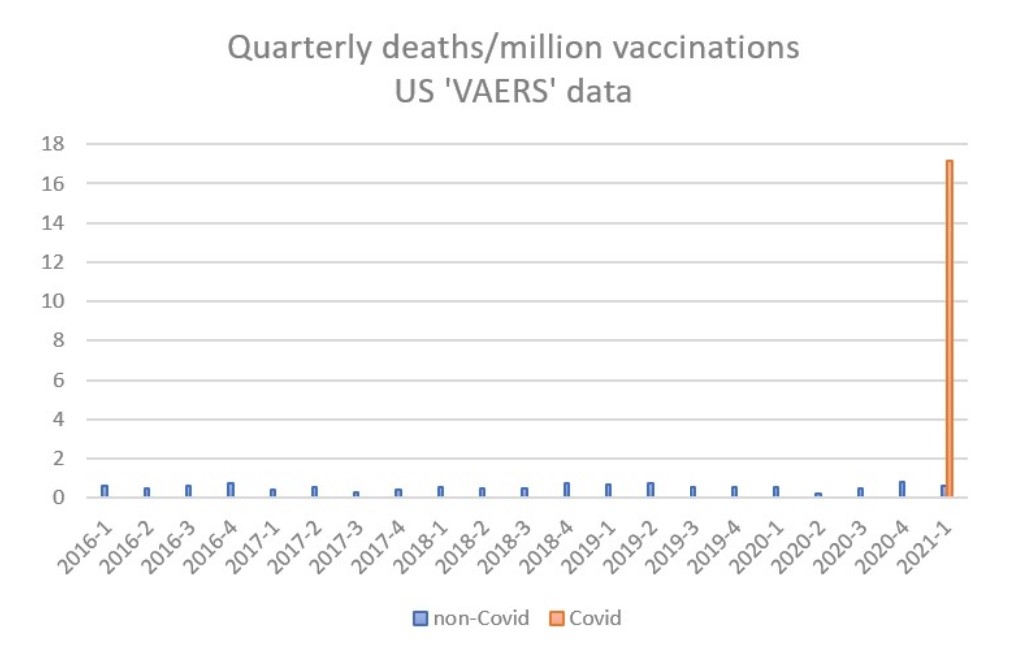
What of the Yellow Card system – is it fit for purpose? I would argue that in the current situation it is not. The MHRA does not provide raw data for scrutiny but the publicly accessible US vaccine adverse effects reporting system (VAERS) illustrates the scale of the problem. From 2016 to 2020, non-Covid vaccines generated an average of 13 reported deaths per month, which, taking account of the number of vaccinations, equates to 0.56 deaths per million doses. In the first quarter of 2021, a total of 2,103 deaths have been reported following Covid vaccines from 130 million doses, giving a rate 16.2 per million doses, i.e., a thirty-fold increase on the background rate. This extraordinarily high rate has been apparent from the first month of Covid vaccine administration, and is not declining.
It is also notable that reports of CVT in the UK increased significantly after several cases had been reported in the press, thus raising awareness amongst medical staff and leading to a change in advice from regulators.
When rolling out a new drug to a whole population which uses a new and untried technology and which has been commenced under temporary licence without the benefit of long-term safety data, it is vital that any post-marketing surveillance is rigorous. As a minimum, every GP or hospital visit should record vaccination status; everyone receiving a vaccine should be given a pre-paid, pre-addressed card with a tick box for any side effects, to be returned to the MHRA 30 days after vaccination. Only then can even short-term safety be assured.













To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
As far out as this sounds, it can be seen to be more of a useful metaphor in the light of Mattias Desmet’s book “The Psychology of Totalitarianism” Desmet’s book somewhat bridges the reality of what is happening now to what is described by this article. Desmet describes the use of maths, statistics to bolster an ungodly level of certainty we can call scientism, when really it can be demonstrated the certainty claimed is entirely false (and I would say ego driven). Scientism, in furnishing false certainties, has divorced humanity from nature and what is real.
And BTW “the singularity,” which is not a far-out concept given neuralink and indeed the extent to which we are already glued to our phones, results in a kind of hive mind. Indeed I would argue much of the social politics and the straitjacket of woke ideas we see today are a result of the “interlocking” of human-neurons in this hive mind. Any mind hates to “see” itself as holding inconsistent principles, so expect any elements of that are not one with the dominant ethos to be killed off.
And then there is Tucker Carlson, who believe demons, real non human entities are on earth and amongst us right now.
Somehow I suspect we (me and most of the commenters on here) are not the dominant hive mind ethos. So that’s us f**ked for a start.
I would highly recommend reading Iain McGilchrist. I think his explanation for the collapse of society fits perfectly. In an embarrassing attempt to summarise: the brain has two hemispheres, left and right, with the left hemisphere understanding the world through a purely mechanistic vantage point which only see the parts and not the whole, and the right hemisphere understanding (or attempting to) the whole with far less regards for the parts that combine to make the whole. McGilchrist believes, and I certainly follow his logic, that society has become very left hemisphere dominated, and is likely a result of the enlightenment, and sciences refusal to properly consider anything that science cannot explain.
I attended one of McGilchrist’s lectures a couple of years ago. Fascinating man with a deep insight into our human predicament. I’ve yet to read one of his tomes, hopefully by the time I die I will have!
The predictions themselves are delusional. However, the people who have these delusions are real and, if wealthy, powerful or influential enough, are capable of doing a great deal of harm as they act them out. For example, because they think genetic engineering offer the prospect of eternal life, they are eager to try out mass-scale experiments on the human population, hence the manic promotion of the COVID vaccines.
No one needs worry about this. It’s science fiction. In the 60s we were told that by the 90s we wouldn’t be bothering with food anymore – we’d just take pills. But now there are millions more food outlets, a choice in supermarkets no one could have imagined then, more TV programmes about food than ever before. Also, depictions of people of the future would show them in spacesuits, very plain clothes, clothes made of paper etc, and of course things have gone totally the other way! As for the statement ‘In the 2030s, medical nanorobots will begin to integrate these brain extensions directly into our nervous systems’. Whose? There are always going to be some people daft enough I suppose, but these will be a tiny minority – perhaps those who spend their lives playing VR games? But most people will have a healthy instinct and mistrust and will not be interested, and probably resistant.
FWIW, I think the image depicting Ahriman in the article is actually the leontocephaline Mithras. Ahriman’s true form is doubtless too terrifying for mortals to behold.
Yes, yes, you have nailed it!
Steiner prophesied that “the Earth will be covered, as with a web, a web of terrible spiders, spiders of enormous wisdom…demonic “spiders”, spinning out a literal worldwide web for us poor humans to become inescapably entangled within like so many fattened-up flies.”
Fascinating article from Steven Tucker. These spider-forms have also featured in movies like “The Matrix”, “Dr. Who”, and one of the Guardians of the Galaxy films even showed similar tiny airships linking up to form a massive net, as a barrier against a huge incoming spaceship.
It all circles back to Kali-Allah, the Moon Spider Goddess of Death, “The Mother Goddess of All India”, and her Toyboy Shiva=Satan, whose symbol is the Crescent Moon, worshipped by millions of Hindus, Muslims, Sikhs, Buddhists, Native Americans (Grandmother Spider)… and Illuminati.
And what a fantastic quote this is! “Elon Musk, once said: “With Artificial Intelligence we’re summoning the demon. You know those stories where there’s the guy with the pentagram, and the holy water, and he’s like – yeah, he’s sure he can control the demon? Doesn’t work out.”
Parents may well kill their children, or children their parents, by sending signals to them, but they must wait afterwards lest they become zombies!
Explanation (so that it doesn’t mess up the effect of the sentence): The people who created UNIX certainly had a very peculiar way of naming things. A process (running program) can become a parent by forking (executing a fork system call) which creates an identical copy of itself called a child. A signal is a numeric message a process can, subject to permission checks, send to other processes. The default action of most signals is to kill, that is, ask the kernel to forcibly terminate, the process it was sent to. A terminated process has a so-called exit status which is another numeric message the parent is expected to poll for by executing a so-called wait system call (which waits for the killed process to terminate if this didn’t already happen). Until this has been done, the kernel keeps the exit status of the deceased process which appears in a listing of all process on the system with a status of Z, standing for zombie.
That’s also where the daemon programs mentioned in the text comes from. A daemon is a background process not associated with a user session.
It is the void and the phallus. The penis and vagina. It has been said that it makes dumber people dumber and smarter people smarter. Obviously there are holes in this but you can look at it as an offering. Feast your eyes on it. Let it corrupt you or exalt you make of it what you will. There is a karma that comes with untruthfulness and dishonesty about one’e own abilities.
I never thought I wqould hear mention of anthrposophy on this page. This is truly a cause of rejoicing. That knowledge that they talk about and try to pass on – it isn’t imagination or analysis. The path of spiritual science can only come about through clairvoyance and this can only be achieved in our time by reading accounts of it and then that world slowly starts to appear. Perhaps now we are ready for that as a culture. Steiner said that it would be around our time.
The human spirit needs to reel against the eigth sphere. We are moving towards the next level of our evolution but these forces can imprison us in a world that essentially sets up an endless loop of torment and vampiorism. As James Joyce said, the walls of hell are four thousand miles thick and made of solid granite. You want to avoid getting into this situation to begin with. Ahriman could be understood as the tyranny of numbers or perhaps as the reduction of the trinary nature of the divine anthropos to the binary. In the secret teaching the three comes before the two.
Ahriman was at his strongest in 1850 just look at that age and the transformation that occurred. The rise of industialism occuring concurrently with a very cold exmination of nature. All sorts of critters with a pin through them after a visit to the killing jar. We had to go through this phase but we need to know when it has to end. Just look at where it has led in economics. Because even Ahriman is less toxic than human greed and when you put the two together you end up with hollowed out countries just like the one we have.
This is the only thing that really matters in our time. If you stop and contemplate you will see that this the crux of the evil that we have to face now.
If you want a good introduction to the secret teaching of all ages there is a Youtube channel called Rudolf Steiner Press Audio. It has an archive of thousands of lectures and courses. I would recommend it for those who are ready for this path.
There is no lazy way out or cheating your wait out or sitting around and biding your time in the hope that others do it. Because the whole meaning of this time is that it is asking you to come to the table untramelled. Nobody will support you it will never be a mass movement. You either ken it or you don’t. We have all wasted our lives to some extent.
My parents sent me to a Rudolf Steiner school, but I refused to believe the gospel and dismissed it, rather undiplomatically, as some sort of “deluded nonsense about fairies and elves running the world”. My parents had to appear in front of a tribunal, where my teachers recounted my many sins, agreed that my heretical views were unacceptable and at the end announced my expulsion from their cult.
30 years later I work in IT and control (sometimes even create) the daemons that help to provide the internet. Working with computers certainly changes you, but I would argue that a lot of programming and other IT work is actually creative problem solving and certainly less harmful than doom scrolling and binge watching. That said, I also think that it’s good to spend a lot of time away from screens and interact with the real world.