
No surge as schools open in the UK, no surge as Texas throws off restrictions, free states like Florida and Georgia doing no worse than lockdown states – is anyone in Government watching the real world or are they too busy gawping at the curves of Neil Ferguson’s latest model?
Jeffrey A. Tucker at AIER has gathered together some of the alarmist predictions made about Texas that have, so far, not come to pass:
- California Governor Gavin Newsom said that opening Texas was “absolutely reckless.”
- Vanity Fair went over the top with this headline: “Republican Governors Celebrate COVID Anniversary With Bold Plan to Kill Another 500,000 Americans.”
- There was the inevitable Dr. Fauci: “It just is inexplicable why you would want to pull back now.”
- Robert Francis “Beto” O’Rourke of Texas revealed himself to be a full-blown lockdowner: It’s a “big mistake,” he said. “It’s hard to escape the conclusion that it’s also a cult of death.” He accused the Governor of “sacrificing the lives of our fellow Texans… for political gain.”
- James Hamblin, a doctor and writer for the Atlantic, said in a Tweet liked by 20K people: “Ending precautions now is like entering the last miles of a marathon and taking off your shoes and eating several hot dogs.”
- Bestselling author Kurt Eichenwald flipped out: “Goddamn. Texas already has FIVE variants that have turned up: Britain, South Africa, Brazil, New York & CA. The NY and CA variants could weaken vaccine effectiveness. And now idiot @GregAbbott_TX throws open the state.” He further called the Government “murderous.”
- Epidemiologist Whitney Robinson wrote: “I feel genuinely sad. There are people who are going to get sick and die bc of avoidable infections they get in the next few weeks. It’s demoralising.”
- Virus guru Michael Osterholm told CNN: “We’re walking into the mouth of the monster. We simply are.”
- Joe Biden famously said that the Texas decision to open reflected “Neanderthal thinking”.
- The chairman of the state’s Democratic Party said: “What Abbott is doing is extraordinarily dangerous. This will kill Texans. Our country’s infectious-disease specialists have warned that we should not put our guard down, even as we make progress towards vaccinations. Abbott doesn’t care.”
- The CDC’s Rochelle Walensky didn’t mince words: “Please hear me clearly: At this level of cases with variants spreading, we stand to completely lose the hard-earned ground we have gained. I am really worried about reports that more states are rolling back the exact public health measures we have recommended to protect people from COVID-19.”
Are any of these experts and commentators now reconsidering their fundamental assumptions and examining the data? What do you think?
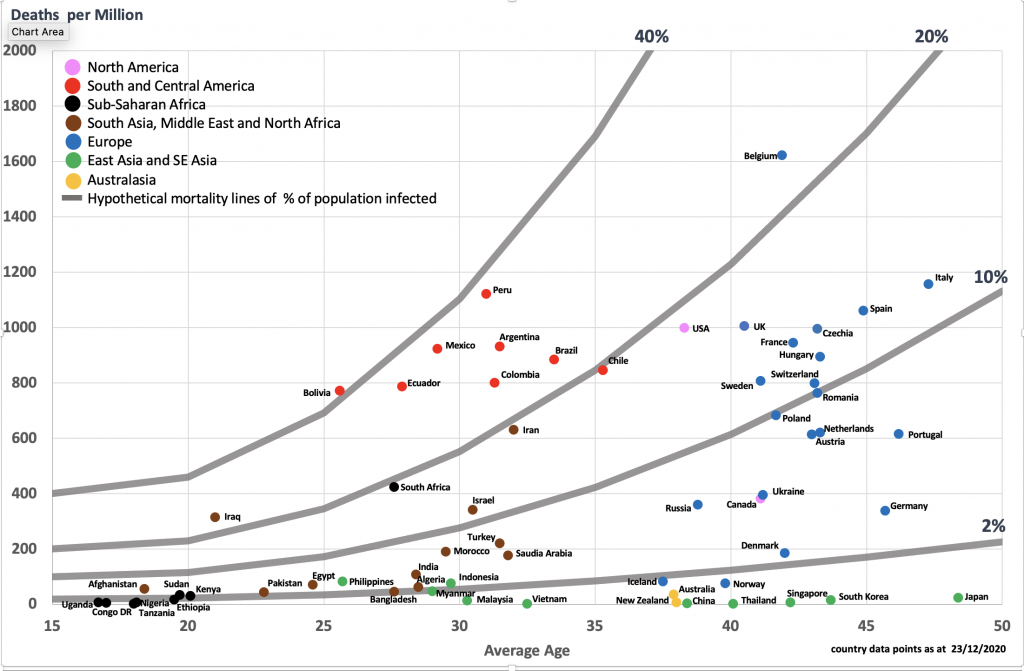
The coronavirus has certainly surprised many of us in the past year, defying expectations by being more deadly in Europe and North and South America than it was in South East Asia, while in Africa and India it surprised by its mildness.
The lazy mainstream assumption that the differences between countries are explained primarily by their restrictions or interventions has not been borne out by any of the studies that have examined the real world data rather than relying on models that bake-in assumptions of lockdown efficacy.
One of those studies, by eminent Stanford scientists Jay Bhattacharya (co-author of the Great Barrington Declaration), John Ioannidis and colleagues, published in the European Journal of Clinical Investigation, has come under criticism since it was published at the start of January. The authors have now responded to that criticism, defending their paper in the journal.
It includes some great quotations from these two pillars of the sceptic movement.
Some suggest that New Zealand’s effective control can be ascribed to its highly restrictive lockdowns. That opinion, unfortunately, has no evidence to support it beyond the anecdotal. As of March 2021, the highest death rates globally have occurred in countries that used prolonged and very restrictive measures, while the lowest death rates occurred in countries with more diverse responses. This is of course no proof of the futility of lockdowns, but it does call into question any claims of a much-worse counterfactual with less restrictive measures.
Experience from past pandemics has shown vast differences in disease spread across different locations, irrespective of measures taken, and we are seeing the same variability with COVID-19. Ignoring these plain-to-see epidemiologic patterns is a disservice to public health and society.
They did admit to one mistake – which actually made their case stronger.
We note that, by mistake, we cumulated the case counts for the Netherlands twice. Correcting this, the trend for the Netherlands points more strongly to enhanced case spread with more restrictive measures (0.08 (0.00-0.17) versus Sweden and 0.13 (-0.11-0.37) versus South Korea.
They do not think much of the models popular among lockdowners, which typically beg the question by assuming what they are trying to prove.
An underlying theme in the letters is that COVID-19’s epidemic trajectories have been difficult to characterise, and have traced trajectories that often seem disconnected from the policies aimed at modifying these trajectories. … The past year has revealed puzzling patterns of epidemic dynamics that have defied models that attribute much epidemic control to policies. At the time of this writing, cases and deaths are declining across most locations, despite models’ predictions to the contrary.
This points to a more generalised and pernicious challenge: how should NPI [non-pharmaceutical intervention] effects be studied? Simulation models are clearly problematic because their results are a direct function of input assumptions. Observational studies, especially using causal inference methods, have advantages. However, when the underlying dynamics are non-linear and the policies are deeply endogenous, as in this case, attribution is precarious. This limitation is shared by all observational assessments of NPI effects.
They conclude that the scientific literature does not support the use of lockdowns, the harms of which are known and large whereas the benefits are unproven and, on current evidence, weak-to-non-existent.
In all, we maintain that the science plausibly supports beneficial, null, or harmful impacts on epidemic outcomes of highly restrictive measures, such as mandatory stay-at-home and business closures. Given their many uncontestable harms to health and society, we believe that the extant literature does not provide strong support for their effectiveness at reducing case spread, and should be subjected to careful, critical, and rigorous evaluation. If the benefits of such measures are negligible (or worse), their perpetuation may be, on balance, detrimental to the health of the public.
Worth reading in full, as is Jeffrey Tucker’s piece in AIER on Texas and the open states.










To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
FA Youth Cup match abandoned after player ‘suffers suspected cardiac arrest’ on pitch | Sports Informer
This is evil and you all know it
Viganò: Considerations on the Great Reset and the New World Order
https://www.lifesitenews.com/opinion/vigano-considerations-on-the-great-reset-and-the-new-world-order/
Next Peaceful & Friendly events: Wokingham & Woking
– let’s join in with Worldwide backlash before it’s too late
5.30pm Friday 3rd September
Loddon Bridge, (Winnersh Garden Centre/Showcase Cinema)
Reading Rd, Winnersh,
Wokingham RG41 5HG
12pm Woking Saturday 4th September – Woking Town Centre- Jubilee square
Stand in South Hill Park Bracknell – Sundays from 10am & Wednesdays from 2pm
Make friends – keep sane
http://t.me/astandintheparkbracknell
21 09 02 Lottery winner 56 https://www.dailymail.co.uk/news/article-9951619/EuroMillions-winner-Margaret-Loughrey-said-27million-lucky-dip-destroyed-life-found.html
21 09 02 Bollywood star 40 Heart attack https://www.dailymail.co.uk/news/article-9950385/Indian-TV-film-star-Siddharth-Shukla-40-dies-heart-attack.html#reader-comments
Pilot mid air 49 https://www.newindianexpress.com/nation/2021/aug/30/biman-bangladesh-pilot-who-suffered-heart-attack-mid-air-dies-at-nagpur-hospital-2351922.html
NZ woman 50’s “first death” https://www.tvnz.co.nz/one-news/new-zealand/nz-woman-dies-after-suffering-rare-side-effect-pfizer-covid-19-vaccine
Australia sailor 29 stroke than death https://7news.com.au/sport/sailing/australian-sailor-jessica-watson-reveals-sudden-death-of-partner-cameron-dale-c-3845979
21 09 01 Sudden Death 25 year old mum Edinburgh https://www.mirror.co.uk/news/uk-news/tributes-paid-young-mum-beautiful-24888983
Yes, teenage player and the story was hidden well down the page in the dm. I suspect he’d been jabbed since it wasn’t menrioned in the story, had he not been I would imagine the headline would read ‘unvaccinated teenager suffers cardiac arrest during youth FA match’
Yes and if unvaccinated would have highlighted the poor kids last words as “I wish I got the jab and I urge others to do the same” or whatever claptrap they always come out with.
All from the past few days. My linked post didn’t get approved.
21 09 02 Lottery winner 56
21 09 02 Bollywood star 40 Heart attack
Pilot mid air 49 heart attack
NZ woman 50’s “first vaccine death
Australia sailor 29
21 09 01 Sudden Death 25 year old mum Edinburgh
I was watching a video on BitChute (it’s mirrored on odysee if you have problems with BitChute’s buffering of videos) of Dave Cullen (Computing Forever) interviewing a NI doctor Anne McCloskey who has had a campaign of censorship and blacklisting against her by the medical Establishment for highlighting a significant uptick in adverse reactions in the under 60s – especially the under 40s from the COVID vaccines, particularly serious blood clotting, stroke and heart problems.
She is alleging that it is being covered up by pretending these are just ‘normal’ occurrences, despite the NHS units covering these ailments being under severe pressure for months since younger people had been vaccinated. Even OAP deaths due to this have ‘flown under the radar’ and have not been investigated, some possibly being attributed to COVID.
She has been suspended apparently:
“Dr Anne McCloskey: GP suspended over Covid-19 vaccine comments”
https://www.bbc.com/news/uk-northern-ireland-foyle-west-58315530
Tragic levels of medical corruption.
Her original video is a tough watch of a lady who imho is evidently dedicated to her patients and the oath she assumed on qualifying as a doctor, but is struggling to hold her composure as she sets out what she has experienced. You have to be heartless not to feel similarly watching her, a very brave lady – my God how we need more of her ilk.
Covid: Prof Jonathan Van-Tam vaccinates Boston United players – BBC News The senior team were vaccinated by JVT. The youth team too?
A professor Shipman?
Well…..here’s a guy who has vaccinated children and he was so smart he decided to hold a snap election on the back of the popularity that his vaccination program would clearly bring him: ‘”Canadians need to choose how we finish the fight against Covid-19″
How’s that working out for him?
‘…an Angus Reid survey this week indicated a drop in popularity for the 49-year-old among voters of every age and gender, including women who have been his staunch supporters.’
Oops!
‘”Three weeks ago it felt like pretty common knowledge – at least with people I was talking to – that it was going to be a cakewalk for the Liberals,”
But now
‘National surveys suggest the Liberals, a left-of-centre party, have lost ground and are now in a statistical tie with the right-leaning Conservatives.’
https://www.bbc.co.uk/news/world-us-canada-58389802
Shame (not really)!
If Trudeau doesn’t make it, alarm bells here, already ringing after Chesham and Amersham, Batley and Spen, will get a great deal louder……..
Trudeau is amongst the worst. Did you see where he called a recession a “shecession”? What an utter moron.
It is still my opinion that he said “Xi-covery”.
That the Opposition ‘Tories’ (I suspect they’ll just be like Boris’ lot – just a bit less authoritarian than the left wingers) in Canada are not up well into the 40%s means that they won’t be able to form a majority government (never mind a landslide). They could find themselves in the same position Mrs May did after 2017 hamstrung over getting laws passed, etc.
It shows how stupid and left wing so many Canadians (like NZers) are that they still favour Trudeau in such large numbers after his many failings and scandals.
Maybe someone should sue his party over the use of the world ‘Liberal’. Someone should do the same in Australia too (their ‘Liberal’ party – the supposed equivalent of our Tories, is rapidly taking that country back to the days of the penal colony).
What worries me is that he wins! Another rigged election perhaps.
If he loses, perhaps this will make leaders around the world take notice and realise that their vicious policies are not as popular as they think they are…
You know things are failing when those in power believe their own PR.
Just like Brexit, the quiet man has been nudged into never voting for these fugging muppets ever again, in fact I’ll go WAY OUT OF MY WAY to make sure they never get to run more than a bath ever again.
Typical Hunt. Politician who once had a job with “Health” in the name is now a vaccine expert, epidemiologist etc. Just can’t bear to be out of the limelight, and no doubt money comes into it somewhere. Too blinkered to look at the Israeli experience.
He wants to keep the spotlight off his negligent spell as Health Minister.
He and Lansley are held in similar regard by medics, clinicians and career NHS employees …..
Hunt: rhymes with ****.
Of course it is a “Religious Mania”, it has always been so. Hence the ever louder drumbeat to persecute the ‘unvaccinated’.
This is nothing to do with science, it is all about control and domination; of body, spirit and mind.
That sentence seems to imply that each booster is only really useful for a particular variant, in which case as soon as another variant emerges – bang – they are going to be telling the vaccinated they need yet another booster.
They said that only one jab was being recommended for children, but THAT narrative no longer makes sense in the light of the claims about boosters being needed to “target” variants, and the growing admission that the effectiveness declines over time. Soon they will be wanting to jab the children over and over again, in spite of the fact that children are not at significant risk. Surely parents are going to react against this eventually?
“Don’t Jab The Children”
http://participator.online/articles/2021/08/dont_jab_the_children_20210805.php
The establishment/Ofcom-censored truth is that the UK Covid epidemic was over by June 2020 and has only been dragged out by the government in order to get the entire population needlessly vaccinated as a Trojan horse to imposing vaccine passports which will morph into coercive social credit digital identity cards, all because they see these as an essential prerequisite to the Davos/WEF/UN “Great Reset”.
Hopefully they will fail because they didn’t bargain on the Covid vaccines being worse than useless. The swine flu vaccine was pulled after causing around 50 deaths while the Covid vaccines have already caused 1,600 UK deaths, perhaps a ten-fold under-reporting, yet still they press ahead. The political ringleaders should all be sent to prison.
I would consider myself quite red pilled but I have always been sceptical about this clot shot being a death shot that was intended to cull the population by the billions.
But with the rabid enthusiasm to administer this now on kids, when we know it can harm them, and know they don’t get hurt by Covid, and know that these shots don’t stop infection or transmission, and whatever they do, if anything, doesn’t last, makes me think, this is indeed a drive to decimate the masses, not just tag and trace us, but devastate us.
Pure Evil.
My husband is exactly like this, exactly. Which got me to thinking, what if, because we all have our eyes open and can see what is happening with these shots, the only logical conclusion we come to, (because they are hell bent on getting it in every arm) is that it must be about de-population.
However, if we were blue pilled then our mind set would, like them, blind us to any ill effects (like death), we would cling to the mirage that the vaccines are 100% safe and will free us from this deadly pandemic. It is their religious fervour that blinds them to the truth, they have built a narrative and they cling to it to their ultimate demise..
That’s where Delingpole’s white pill comes in. When you see this as unadulterated evil, you realise that this is confirmation of God.
Those who refuse to see it and fear death instead of damnation are in effect dooming themselves. They are Godless and irredeemably faithless.
Ive always been spiritual and believed in a higher power, sceptical of atheists, but now I’m certain that God exists and only through him will this be bearable.
Sorry to my fellow atheists. Nothing against you. It’s a personal thing.
I’m not a believer but tend to think one lives better if one fears damnation more than death.
This is very interesting, the white pill, I must listen to Delingpole’s podcast more.
I was brought up in an atheist home, which didn’t bother me at the time, but now as an adult with children of my own, I do feel an enormous spiritual hole as it were. I have always strived to be very ethical and moral person and I have cobbled together a sort of spiritual belief of my own.
This part where Delingpole says that when you see the evil it is confirmation of God, I struggle with this, has God intentionally brought on or allowed the evil to exist, or does God have no control over it?
I try and frame it as the normal rise and fall of the “universe” we are all intricately bound together, in some larger tapestry, like threads ( I know it sounds airy fairy but it makes sense in my mind) and we rise and fall, we make choices good or bad. I don’t think this life is it, we must live well in this life, karma and all that.
I do agree that this horrendous period will lead to a spiritual re-awakening. Lately having never prayed before I have found an urge to pray, for my family and humanity! I even bought books on prayer having never done anything like it before. I find it does help me at least. I have to hope for the future for my children!
“has God intentionally brought on or allowed the evil to exist, or does God have no control over it?”
This is indeed, in part, a huge question – The only thing I do know from my reading of scripture is that God does have control over it. There are 365 exhortations not to worry throughout scripture – thankfully one to contemplate per day. Despite this, in the face of relentlessly negative news and reporting of the utterly evil machinations of some, I have to take up my courage anew each day.
I do not claim to understand the depths of the depravity we face but for my part I will look to live as three young men did when faced with certain death & declare: “There is no need for us to defend ourselves before you in this matter. If our God, whom we serve, can save us from the white-hot furnace and from your hands, O king, may he save us! But even if he will not, you should know, O king, that we will not serve your god or worship the golden statue which you set up.”[the book of Daniel]
This does not mean I will lie down and allow myself, or others, be trampled on – there are plenty of biblical examples of how we should be fighting tyranny – and It is my intention to be a thorn in their side wherever and whenever I may.
Thank you for this Debra, I also will be a thorn
Good and Evil are opposites, so if Evil exists so does Goodness.
I have never been particularly religious but I have woken up to the real evil that surrounds up, that has always surrounded us but has remained somewhat hidden until now. My beliefs have been totally shaken up, I’m feel that God does exist in many forms. It’s been an incredibly personal journey, and it’s given me the strength and faith to fight in some way, everyday.
I used to be a regular churchgoer but as time went on I grew disenchanted with religion. However recently I have found myself praying once again asking God to deliver us from this Evil. Whether he will listen to one who abandoned the faith, I can only pray He does.
Sorry much as I’ve tried I really can’t get into this religious thing. I suppose a Public School education didn’t help as you were shoved into it everyday and with twice weekly Chapel it all rather put me off. Don’t get me wrong I love churches and the aura they give off and a good warble. Just can’t get into the praying bit, never have. Perhaps God doesn’t like me.
PS I’ve always tried to lead a good life and to know good from evil and what’s going on is definitely evil.
There is no profit whatsoever for the elite in “decimating the masses”. The goal here is to convert them into obedient, easy to control, gullible slaves, not decimate them (which would create an uprising).
The profit is in extending (by orders of magnitude) the length of time finite resources will last.
They’re certainly very careless about causing death though, aren’t they? That’s clearly acceptable collateral damage at the least.
If you Google some phrases like “population decrease needed…climate change” a number of hair raising papers arise discussing how much the reproduction rate and population numbers must decrease.
A mandatory contraceptive vaccination programme seems not implausible down the line. After the climate fear porn.
I have had similar quandaries to deal with over time, and the putative forced vaccination of children, parents being sidelined, is the game changer for me. Info streaming from Stew Peters ( most of it, not all ) Del Bigtree, AFLDoctors, McCullough, Fleming, Cole, Ardis, Martin, Iaonnides, Bhakdi, vd Bossche, Yeadon – the list grows – all of these medics/scientists are risking personal relationships, careers and financial security by speaking out and I do not see too many UK politicians/SAGE illuminati doing similarly.
I don’t think they’ll get the take-up for these ‘boosters’ that they think. I know a few people who have been double jabbed and are having regrets. No way are they having ‘boosters’. I also know people who haven’t been jabbed but who’ve told their employers that they have just so they don’t get hassle at work. I don’t believe that they have the numbers jabbed that they say they have either, they lie about everything. I don’t believe anything these tossers say!
My sister is a hypochondriac and a regular pill popper so I fully expected her to get the jab, which she did. I asked if she was going for the booster but she said she wouldn’t. So there is hope yet!
BBC News (on in the background so I can keep up with The Enemy) states 6 million have “not yet” had their jabs. That’s quite a lot really. Doesn’t really tie up with the vaccie claims.
What we don’t want to do is boost people and then find we have a new variant and we can’t boost them again because we’ve boosted them too soon – and those people might not have needed the booster in the first place. So there’s a lot of very complicated modelling and data analysis that is going on about this at the moment.
If this doesn’t red pill you, turn you off and tells you that they are flying blind, making it up as they go along and will jab you at least twice a year for the rest of your likely short life if you succumb, you can’t be helped and fully deserve what’s coming.
Yes I agree, had this conversation with my neighbour (a believer)…where I pointed out it wasn’t a booster, it was exactly the same vaccination that she’d already had and which had already failed…twice! Her face was a Picture!
I’m not disagreeing with you but I like the comment that the booster shot is the same as the other 2 “vaccines”. Do you have a link to this as my Google search came up with the usual “why you should have the booster” clap trap.
Is a third dose the same thing as a booster dose?The dosages are the same, but there’s a small medical distinction. The term is used differently based on who is receiving it. Boosters are offered to people who got the full course of a vaccine and developed a good response initially, but it waned over time. Third doses are given to people whose immune systems weren’t able to fully respond to the initial vaccines. That’s why the FDA and CDC first recommended an additional dose for immunocompromised individuals.
Will the boosters be different from the jabs administered so far?The Guardian understands the booster doses will not be specifically tweaked to tackle the Delta variant, which has become the UK’s dominant variant.
Looking at the USA and UK, and in Israel it’s just another dose. I think the term booster is being used to make it sound less invasive somehow. As in the statement from the USA above…it’s a booster dear not a third go at a failed vaccine!….
The government have invested billions of taxpayers money into these jabs and they have to get rid of them before their sell by date.
Meanwhile, there are those that have not been ill, not had the Vs, not having the boosters, not had side effects, still not been ill…
People have been brainwashed by the media, I don’t think they deserve it. The media, the academics and the politicians do deserve to face consequences in a court of law however, there has been a gigantic abuse of power and influence here.
Really great article Will, all be it in a holy fck what the hell is going on kind of way.
Thank you to who posted this Highwire yesterday, can’t remember who, but please all watch and share it.
https://rumble.com/vlve7n-are-we-starting-to-see-a.d.e..html
To vaccinate children, if they know this is starting to happen is criminal, no if’s, no buts, it’s criminal.
I’m not a science person, but I’m going to email Prof Harnden and basically beg him to hold his nerve, he sounds like a man who knows what is right and what is wrong, but must be facing insurmountable pressure.
May good win out in the end.
Good call.
Just done
Dear Professor Harnden,
Please forgive my impudence in emailing you, I can only imagine this is one of many hundreds of emails languishing in your inbox, but I feel compelled to send it anyway.
I wish to beg you to hold your nerve, and not submit to the insurmountable pressure you must be under to agree to the vaccination of young children.
I am not a scientist, or expert in anything, I don’t know about any of the issues you have to deal with, and would never import to. I am simply a terrified and overwhelmed mother who can’t quite believe the direction we are travelling, it feels like a runaway train that is about to come off the tracks, and I do not wish any child to be injured when that happens.
I implore you to stand your ground. Again, I have no other reason for saying so other than genuine fear and concern for the welfare of our most precious children.
Kind regards
I think they listened to you. Perhaps the final straw?
BRAVO!!
Oh, well, if the committee held a long meeting followed by a vote on Thursday, everything should be ok then!
“Religious mania” Indeed, the religion in question being Satanism.
gee, nobody saw that coming.
But what does it mean? Let’s say you’re insane and decide to vaccinate your kid today. Will they really need to take all 3 shots before their passport is valid?
By the time everyone has had their third shot, it will be time for the fourth
There will never be a time when the population as a whole is “fully vaccinated” – this is excellent news for those who want to keep using covid as an excuse to grab more power
How many times do you need to be spiked to be “fully vaccinated”?
The answer is of course always one more than you have currently had (unless you are one of us filthy unvaccinated, where soon we’ll probably need a double-digit number of stabbings in order to be “fully vaccinated” because we are getting so far behind on the expected number…)
… and profits.
I suggest grab more money instead: A mandatory, patented medicine which has to be taken ad infinitum in order to chase an effect it was never meant to have is the ultimate money maker for the pharma industry. They’ll just keep on vaxxing until everybody has died of some side effect (statistically, the chance to survive a COVID vaccination decreases with each shot).
It’s going to be interesting to watch this escalate to a point where people can only travel in a short window after one or more (for each variant) recent booster shot. Madness.
Great article Will. Its what I have been waiting for from DailySceptic.
It’s not approaching it, it’s already there. Have you seen how many people walk on the street, by themselves, with no one else around, with masks on? I saw a couple out for a walk with their kid, and even the kid had a mask on! Or people wearing masks while in alone in their cars. How scared do you have to be of this thing to wear a mask with no one around? It’s beyond reason. There’s no one around you to give it to you or for you to give it to them, you are most likely already vaccinated, cause I can’t imagine you refused to, but you still wear a mask. Why? This has reached religious levels, with fear of an imaginary bogeyman requiring you to take irrational, ritual methods to ward off the bad juju.
I figured all those people are just preparing for their holiday in Australia. Maybe not.
Irrational devotion by definition is disconnected from facts or logic. Last year Ivor Cummings mentioned the British town that bought a tiger horn, and then rings it every day, and lo and behold, no tigers. It’s lunacy. I don’t believe masks provide much (if any) reduction and no where to the level to afford it’s many costs, but there is negative proof wearing masks outside provides any benefit. It’s actually a harm. If this government wanted to prove itself honest it would run a campaign telling people, “masks outside are for superstitious numpties.” But somehow I can’t see this government ever being honest with people. Makes me wish I was Swedish for the first and only time.
fixed that for you.
Went round our town on Friday and was amazed how few masks there were.
It’s getting better, but just wait a bit until the winter flu season starts…
Any booster should be reserved for those few in the immuno suppressed community (cancer patients, Lupus, etc). The article pushing it from an Israeli doctor saying we had just weeks or to avoid their fate not only failed to realise we had Delta first or that the dip in cases among over 50s was both temporary and could be traced potentially to other factors. To say nothing or how those doses could help others globally.
As for 12-15 (really 12-17), here is what the government should do, regardless of JCVI decision. Send to every parent the actual known risk from Covid for their child, and then compare that risk to seasonal flu, traffic accidents, falls, lightning, swimming and so forth. Then provide proven data on vaccine issues with 18 and under from US, Canada and EU (where it’s been happening all year), so parents can know just how “reassuring” the vaccines are. If we give us these old fashioned things called facts, in context, and not fear, parents would see they either need to wrap their kids in bubble wrap and make them live 24/7 at home in a bubble or that, surprise, they should not be jabbing their children. Facts not fear.
I’m vaccinated. There is a risk-reward crossover point where vaccination, freely chosen, makes sense. It certainly doesn’t go down below 18, or truthfully under 25. So why this push? It’s either, given most under 25s have had Covid and thus already provide herd immunity benefit (94% of all adults), to make them be able to show highest vaccine rates globally or some other, non-medical motivation. Perhaps…unions?
You say deal in facts then say there is a risk/reward cross-over point. Prove it, where are the facts?
I looked in the past and the crossover point for healthy males was ~50 years old, older for females.
I used the oxford covid risk calculator and then compared against the jab risks (using the massively understated figures).
BTW After i did this i realised what an utter con the whole COVID circus was.
I don’t know how an immune system ends up repressed, so I welcome any and all clarification. But… if the immune system is supressed, how are you going to get a vaccine reaction from it?
The vaxxine directs the immune system to look for specific virus strains leaving the immune system open to infections it would naturally have fought off. That is my understanding.
Yes, but if you have no immune system to speak of, what will the vaccine direct? Also, if you do have an immune system but it cannot recognize the viral particles and fight them, how will a vaccine get the immune system to recognize the viral particles and fight them?
we don’t really know the cross-over point until we have long term vaccine safety data, we just know the long term safety data is less important for the elderly
“As” for 12-15 (really 12-17), here is what the government should do…”
It’s too late for that. A lot of parents would not read it, or would read it and get their kids vaxxed anyway. People are not thinking straight. The mass vaccination program is simply evil and must be stopped now.
Prof Sunetra Gupta’s (her of The Great Barrington Declaration) article in the Telegraph is going down well with readers.
TBH, I’m surprised the Telegraph even published it, let alone allowed comments, given who ‘finances’ their ‘Global Health Security’ section. Maybe one got through the cracks.
On the other side, (IMHO) creepy globalist elite ex-Health Sec (no, not Hancock) Jezza Hunt has been putting forward his ‘amazing plan’ for social care (presumably we now get to pay more to be infected with COVID and dumped back in a nursing home and left to die when we’re older).
Of course, the esteemed Telegraph editorial and moderator team has decreed no reader comments allowed on that one, and are seemingly deleting reader comments about the article from the BTL on today’s Letters Page.
I think that Gupta still “passes” because she’s still at the “same table”, still discussing pros and cons for vaccines for certain age groups, conditions etc, ie. her arguments are “relative” and continue to give ( some/enough ) credence to the establishment’s narrative/”reality”.
It’s sheer insanity. “Okay, the vaccines do exactly what the manufacturers told us when they were developing them: they are not intended to prevent catching or passing on Covid. Right, so, what we will do is we will give people more of this and see if it does prevent them catching or passing on Covid. Sounds like a plan to me”. A voice at the back of the room says “What happens in 50 years when the boosters still aren’t preventing people catching or transmitting Covid?”.
Not insanity. Evil.
Humanity won’t exist in 50 years.
Luciferian mania.
I’m not sure how the tests work, so I might be about to write a load of rubbish, but:
If the vaccine mimics the virus enough to stimulate an appropriate immune system response, then wouldn’t the vaccine similarly cause a positive response to the test? If so, we would expect to see rising case numbers.
If the test is able to discriminate between the real virus and the vaccine, then presumably the immune system would differentiate between them too, reducing the effectiveness of the vaccine, leading to the evolution of more virus variants.
I’m more than happy if someone can put ne right on this!
The test looks for RNA strands from dead viruses. The vaccine uses a spike protein mimic to stimulate the immune system.
Since the test isn’t looking for the spike protein, vaccine cell remnants don’t trigger the test.
In dead cow terms, the test looks for the tail whereas the immune system is stimulated by a load of ears.
That’s clear – thank you!
This is unfortunately not true: The claim-to-fame for the so-called Kent variant was that S gene avoidance: A particular genetic something associated with the spike protein didn’t show up in tests anymore and it was conjectured that this spike protein mutation could enable immune escape.
Hence, tests do test for spike protein somethings.
NB: I’m absolutely not a subject matter expert, I’m just repeating this as it was published at that time.
Breaking news: not enough evidence to justify vaccinating younger teens
https://www.bbc.co.uk/news/health-58438669
According to that the JCVI seems to be leaving open the possibility the govt could go ahead anyway on the basis of “wider issues”:
It also says those 12-15 with underlying conditions will now be eligible for two doses – that’s one in 10 according to the numbers quoted.
Yes, guess that you are right, didn’t spot that! My attention was taken with the headline.
It is still good news though I think in that the fact that there’s no benefit for the children is plain for all to see, it might make more parents object, and maybe that will make the govt. more nervous about pressing ahead with the insanity.
Agree, let’s hope so!
The reprehensible Spector raising his head again. Where does he get his funding from I wonder?