There follows a guest post from HART member and Lockdown Sceptics veteran Dr Clare Craig responding to the alarming reports today that, as the Express headline put it, “Kent Covid strain could be twice as deadly”.
Yesterday the BMJ published a new article comparing mortality rates in people with old variant Covid and new variant Covid from October through to the end of January. Their headline conclusion was that the risk of dying was 64% higher in people who had caught the new variant (and perhaps up to 104%, hence the headline that it “could be twice as deadly”).
Before worrying that this may be the case it is worth looking closer at their results. There are a number of odd things about this study:
- Each person with old Covid was matched for sex, age, ethnicity, deprivation, location and date of infection. There were over 214,000 pairs found. However, it turned out that there was extensive duplication in the data and many of these “cases” were the same people. After removing duplicates there were only 54,906 pairs left.
- The two groups were not matched for comorbidities, meaning the study did not control for them. This was unfortunate as many comorbidities increase the mortality rate significantly.
- Their main finding was that 227 people in the new variant group died compared with 141 in the old variant group. This equates to a 99.59% survival rate compared to a 99.74% survival rate. While the difference may – according to the authors’ methodology – have been statistically significant, this does not equate to it being of any practical relevance in terms of the threat of this virus to society.
- Only people testing positive in the community were included which may account for the high survival rates as care homes and hospitals were excluded. However, the CFR was as expected from studies that did include hospitals and care homes in the over-70s but much lower than other studies in the under-70s.
- Mortality rates in Covid are markedly age dependent so it is important to interpret these results in the context of the age of the people in the study. To get a picture, suppose 50,000 members of the public had been randomly selected as a control with no Covid at all. According to the data in this study, this group would have seen the same mortality as old Covid in the first 10 weeks of the year (just as the normal mortality risk of being alive) and the same mortality as new variant Covid within the first 17 weeks of the year. After spring, David Spiegelhalter published on the risk of death from Covid pointing out that the infection fatality rate for someone who caught Covid was the same as their risk of dying this year without Covid. The fact that the mortality risk in this study is only 20-33% of a year’s worth of mortality suggests that Covid, in this study, is less deadly. Case fatality rates (CFR) always overestimate mortality compared with infection fatality rates (IFR) as the latter are based on immune responses and include all the mild cases that may not have been diagnosed as a case. The fact that this was based on case fatalities not total infection fatalities, like the David Spiegelhalter data, suggests it is even less deadly again.
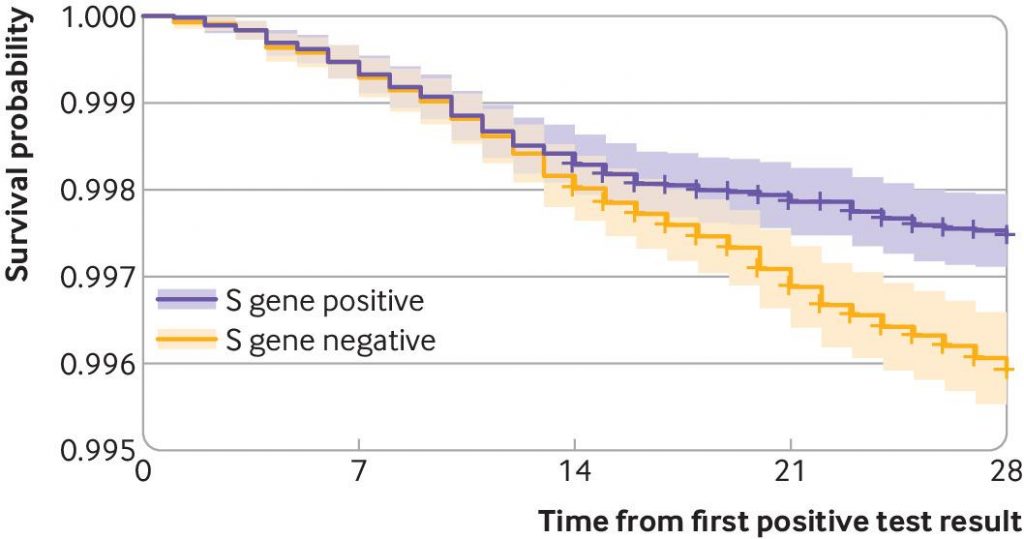
- The distribution of the deaths over time was also odd (see graph above). People with old variant Covid died mostly in the first two weeks and deaths after this time were fewer, reaching a plateau after the risk of the infection had passed. In contrast, deaths from the new variant continued linearly throughout the month of follow up. This is a very odd pattern for an infectious disease. The expected pattern would be that a more deadly variant would have a steeper gradient from the outset with both survival plots plateauing as the risk from the acute infection passed. Where the risk of death is the same the first day after infection as a month later it suggests there are other factors at play. Could a group with more comorbidities see a similar effect of the disease initially but a continuation of deaths from subsequent organ failure?
It should be noted that the difference in CFR reported in this study between new variant and other old variant is of a similar magnitude to that observed between regions for overall Covid CFR. Ultimately, a difference of only 0.15% between two groups where there has been no controlling for comorbidities should be ignored.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Is the original ‘Covid-19’ still supposed to be around, or are we allegedly dealing with mutants, strains and variants? The whole thing has become so ridiculous it exhausts me now.
Truth is, which ever strain/variant/thing is on the cards, they’ll make it as dangerous as they want it to be. It’s what ever suits the pace of their transition to Chinese-style communism.
I read this BMJ paper yesterday.
As soon as I got to the bit about comorbidities, unfortunately near the end of the paper, I realised it was total junk.
‘Some of the increased risk could be explained by comorbidities. Information was not available about comorbid conditions in the data we analysed’ (Ref. above)
Oh for heavens sake! Once you have understood dodgy death registration, you have understood pretty much everything about this global weird out.
But if you haven’t even bothered to look at comorbidities, then you are part of the problem, not the solution.
And this kind of paper, written about also in the Spectator, is indicative of the scale of the problem within the medical profession; the lack of balance, perspective, even within highly regarded medical and current affairs publications.
Medics won’t tend to have stats backgrounds. Most academics that use statistics wouldn’t have had any formal training. Most papers that contain statistical analysis are junk.
https://influentialpoints.com/Training/statistical_mistakes_in_research_use_and_misuse_of_statistics_in_biology.htm
“Statisticians suggest that at least half the published papers in biology contain serious statistical mistakes”
Just like the so-called vaccine trial results, the media ( and apparently the idiots writing this paper) have no comprehension of the difference between relative and absolute risk.
Even if we took the results on face value, which you can’t because of the way comorbidities have been omitted, the absolute risk could move from 0.23% to 0.38% IFR.
Are the incessant attempts to justify more restrictions not perfect evidence of a desire for power rather than any actual danger.
They also didn’t pair them based on symptoms. Everyone in the study started with a Pillar 2 positive test.
If we assume that B117 is basically the same (for the sake of argument) and its meteoric rise to fame and prominence was just founder effect then the people getting B117 more were the 10% doing 80% of the spreading.
These people are less likely to bother with the T&T program or to get tests in Pillar 2 unless they think they might actually have Covid. So they may have had more symptoms and worse symptoms when they entered the game. We know they were positive at lower cycle counts (the study said that). If you knew the true number of mild and asymptomatic B117 infections the IFR estimates might come much closer together.
A lot of sloppy work in academia doesn’t matter because its on esoteric subjects, but it certainly does here. Peer review should have picked up the errors, but obviously failed-an ever increasing tendency as more & more papers are published. Reviewers are anonymous. But I bet they came from the authors’ small circle, think like them, quote from each other’s research and generally don’t want to upset the variant cart.