
The latest Technical Briefing on the Variants of Concern, number 23, has been published by Public Health England (PHE), so we can update our (unadjusted) estimates of vaccine effectiveness against the Delta variant using the data it includes from sequenced Delta samples from positive PCR test results in England.
As before, we subtract the figures in the latest briefing from those in briefing 17 to give the figures for the period June 22nd to September 12th. This gives us a picture for the whole Delta surge, which allows for the fact that most of the early reported infections were in the unvaccinated and most of the later reported infections were in the vaccinated (see below). PHE has recently also published the most recent month’s data for all reported infections (not just sequenced Delta ones), which shows lower vaccine efficacy in the most recent four weeks (a new report released on Friday shows this has dropped even further in the most recent week). However, given the apparently delayed infections in the vaccinated, when estimating vaccine efficacy against Delta it seems most accurate to look at the figures for the whole surge, not just the last month.
We use figures for proportions of the population vaccinated by age derived from the PHE Covid surveillance reports.
Starting with the over-50s, for the period June 22nd to September 12th, PHE reports 68,445 Delta infections in the double vaccinated and 7,575 in the unvaccinated. PHE figures show that in this period the proportion of the over-50s double vaccinated increased from 87% to 89%, giving a mean of 88%, and the proportion unvaccinated was stable at 9%. Calculating the vaccine effectiveness against Delta infection in the over-50s (1-(68,445/88%)/(7,575/9%)) gives a figure of just 7.6%. This is down from 15% two weeks ago and 24% two weeks before that. This continues to be very different to the estimate in the recent Oxford University study using ONS survey data, a study which I criticised for numerous inconsistent and implausible findings.
With regard to deaths with Covid (within 28 days of a positive test), PHE reports 1,515 in the double vaccinated and 552 in the unvaccinated in the over-50s in this period. This works out (1-(1,515/88%)/(552/9%)) at a vaccine effectiveness against death of 72%, down slightly from 74% using data from the previous briefing. This is a 72% reduction in mortality including any reduced risk of infection, not in addition to it. It continues to be an encouraging figure, albeit lower than earlier studies have suggested, and dropping week on week.
For the under-50s, for the period June 22nd to September 12th, PHE reports 81,718 Delta infections in the double vaccinated and 195,957 in the unvaccinated. PHE figures show that in this period the proportion of under-50s double vaccinated increased from 18% to 42%, giving a mean of 30%, and the proportion unvaccinated decreased from 61% to 50%, giving a mean of 55%. Calculating the vaccine effectiveness against Delta infection in the under-50s (1-(81,718/30%)/(195,957/55%)) gives a figure of 24%. This is down from 27% two weeks ago and 37% two weeks before that. Though higher than in the over-50s, it is still very low and much lower than earlier studies (including the trial) indicated.
For deaths, PHE reports 48 in the double vaccinated and 126 in the unvaccinated in the under-50s in this period. This works out (1-(48/30%)/(126/55%)) at a vaccine effectiveness against death of 30%. This is up from 20% two weeks ago and 12% two weeks before that, but is still very low and much lower than in the over-50s. This may be because higher risk people are prioritised for vaccination, or are more likely to consent to it, in the younger age groups, and the rising efficacy may reflect the increase in lower risk people being vaccinated.
These figures are much lower than those commonly quoted and used in modelling, and if they are closer to the truth then they mean the official, self-congratulatory estimates of “100,000 deaths” and “24.4 million infections” prevented by the vaccines are huge overestimates.
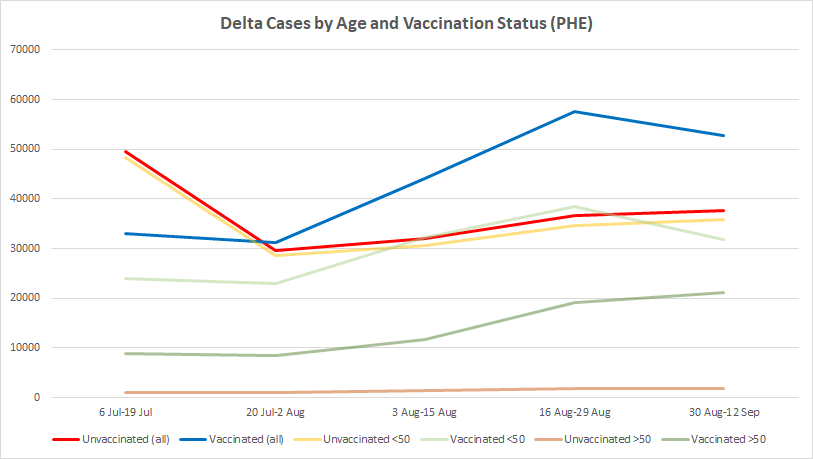
By plotting the differences between the reported total Delta cases in the last five briefings we can also get a picture of how they are changing over time in the different age and vaccine-status cohorts. The red and yellow lines in the chart below show that new reported Delta infections in the unvaccinated have continued gently to increase, as have reported infections in the vaccinated over-50s (dark green line). On the other hand, new reported Delta infections in the vaccinated under-50s dropped in the last two weeks, driving an overall drop in reported Delta infections in the vaccinated. This may mark the peak of the Delta surge in the vaccinated, and possibly overall, though the gentle rise in reported infections in the unvaccinated since the start of August adds a smidgen of doubt into that inference.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
It is my understanding that PHE class the ‘unvaccinated’ to include those who have only had one clotshot or those within 14 days of having the second.
Surely this has to be acknowledged otherwise reports like this are as meaningless as the reports produced by SAGE.
I would also like to see an analysis of the relative state of health of the vaxxed vs the unvaxxed as this is a huge factor in how covid affects people
The PHE report has separate categories for those who have only received one dose.
Which makes this report even more meaningless.
Why? There is a direct comparison between those who are vaccinated with 2 doses and those who are unvaccinated.
.
You have to go through one dose and compromised immunity before being protected. I think that is very important.
It would seem that the compromised immunity is a prolonged state in many people as evidenced by the 20 fold increase in cancers and increase in growth rates of these cancers found by a large lab in the US. People forget that most cancers are dealt with by the immune system and that in an increasingly teratogenic environment it is not a good thing to compromise your immune system.
This may well prove to be the biggest unintended consequence of the ‘vaccination’ program(me).
All true but this blog post only focuses on protection from Covid.
Ironic that pharmaceutical companies own Cancer Research UK
All leads to profit.
All “health charities” are fronts for Big Pharma.
Good point. I thought when I read a recent piece about two women who developed severe headaches, eye disturbances etc after the shot and turned out on scanning to have unknown brain tumours, that that might be because the jabs worsened inflammation and so had uncovered the problems. (The jabs didn’t cause the tumours.) But it could be that they accelerated due to the weakened immune system – or both.
It depend what you’re trying establish.
The 2 dose vaccinated v unvaccinated shows the efficacy of full vaccination.
Tracking the outcomes for every vaccinated person through to ‘full’ vaccination is important but it’s not the same endpoint.
You need to know what percentage in the two groups are naturally immune before any assumptions about efficacy can be made. As Rick says in a striking phrase, can’t plait…
It’s not the same endpoint, because it’s an endpoint that exists in the real world.
But is that actually a category for those 14 days after the first dose?
The problem with all of these articles that use official data is that, in the end, you can’t plait shite.
See my post further down for more detailed graphs folks.
Worth 30 minutes of anyone’s time! https://odysee.com/@Corona-Investigative-Committee:5/Reiner-Fuellmich-Introduction-English_BestCut:e?fbclid=IwAR17Y7l-6Y-ZMNaqwH6GvV74kcq-VfhCRrRIvMAgVJUWJyhS5qGq8t-jWVQ
Unfortunately Fuellmich’s case is weak. Too much of it relies on speculation.
David Martin provided the only real concrete evidence that might hold up in a court of law. The PCR test claims are valid but they can be easily brushed aside by the ‘globalists’ who can point to hospital numbers and even doctors on ‘our side’ acknowledge that Covid-19 is a real disease.
and what causes the “real disease”, how does this manifest itself?
So the FDA advisory panel has said no to boosters for the widespread population. It will be interesting to see if they go ahead with approval anyway
Yep – the ‘need’ to protect the mental health of boostees will, of course, over-ride any health concerns!
heres a 2 minute clip from the FDA panel meeting
may explain their decision…
https://gab.com/a/posts/106949903082365746
It’s good that the ‘effectiveness’ of the vaccines is ‘down’ because this means The Covid Show can roll on and on forever.
They don’t want it to end, and it will never end.
Vaccine Passports for everyone – you know it’s coming.
TL;DR Version: The gene jabs don’t work. Gotcha.
Those in charge are measuring effectiveness by a different measure though, and it is nothing to do with reducing deaths or infections. Quite the opposite in fact.
A must watch from the FDA meeting today. We were right all along. People on Gab have been talking about this stuff for MONTHS:
https://media.gab.com/system/media_attachments/files/085/284/838/original/b77baae8ab60b848.mp4
can you post this in the next article too
These results are based not on infections but on a positive PCR tests. There is a distinct difference, especially since the PCR test can be “tuned” to give a desired result simply by varying the amplification factor.
Just about to post the same. We know its been dialled down in the US for vaxed so unlikely not to have happened everywhere else.
It only needs a little changed in these numbers to show absolutely no effect at all. Which is probably nearer the truth.
A minor irritation. The percentage of blacks in UK is 3.1%, the percentage of blacks in NHS is 6%. The odds of the photo being reflective of real life is very small. We have to put up with this ‘psyop’/nudge in TV, newspaper adverts, and company promotions all the time. Can the DS try not to join in?
Sorry, but I don’t see how a disorganisation like the NHS can possibly discriminate between samples taken from vaxed and unvaxed. They still send faxes FFS!!!
and so do loads of other organisations ( some, very “cleverly” via email….)
You beat me to it.
So, why the tests? Ramped-up fear, yes, but is there any other reason?
Pharma and ‘security’ agencies have wanted a global DNA database for years and PCR tests are done on blood samples.
Are any other analyses run on those samples? If so what and could they also be done on lateral flow samples?
The ‘good news’ is that because of the ineptitude referenced to by Will above many test result data ( most?) have not been processed for DNA.
Absolutely – How has the WHO adopted ( and since rowed back from , twice) Cormen-Drosten RT-PCR mass testing regime been “tuned? Reading the “ILLA” pdf, it was tuned before being adopted by reducing the triple gene extract methodology, very deliberately it appears from three segments down to 1; it is fundamentally flawed because as I understand it does not test for the whole sequence of SARS COV2 – initially it was to test for the beginning and end and a middle element of the gene sequence to increase the chance of it being “right” but it appears not to do that – only one nano fragment of genetic code is tested that can appear in other organisms – or so I understand.
Dr Fleming demonstrated that CT rates beyond 25 produce a flatline in outcomes; as long as this charade of “positive cases” is played out, you just know that either Johnson is too thick to understand, or SAGE/Witless/Unballanced & co demonstrably have another non health agenda – if it was about health, disease prevention, pre hospitilisation treatments would have been fast tracked ( at the same speed as the “miraculous” development of the massively under tested “vaccines”…….) prescribed on first symptoms a la McCullough and others, with hospitilisation only as a last resort. Instead the exact opposite has happened, Johnson & Co have finished the destruction of the capacity of the NHS to deal with emergencies – the rate of attritional reduction in clinical medics of all shades appears to be catastrophically high as a direct consequence meaning that this Winter will be the version from hell as Dr MY and others have predicted.
Forgot to add; there is the fundamentally difficult issue that Polymerase Chain reaction technology was not designed to test for RNA matter..and so has to undergo “conversion” ( a strictly non scientific description ) from RNA to DNA – presumably by reverse transcription, the process that people who refuse to acknowledge is entirely possible with these gene editing therapies (Pfizer’s terminology, not mine). What better example of bankrupt thinking – the acceptance of a process inherent in a process”A” deemed by some to be valid, but when the self same process deemed by the same flatearthers as impossible when related to process “B” – the – now clinically proven by autopsy – malign effects of the “vaccines” as they describe them.
Amongst other statements made by proponents of this fraudulent testing regime is this “Scientists use special software to interpret the signal as a positive test result.” ( eg Ref; myclevelandclinic ); Very inconveniently, Kary Mullis stated on camera that his Nobel Prize winning invention does not/cannot test for infection ( which this and other “support” and even Drosten is quoted in the “ILLA” pdf that HIS RT-PCR regime result should not be taken as accurate without further (medical/clinical) analysis and assessment – and he should know, he is the chief culprit in this charade!
So I am very puzzled on a Sunday yet again – why are people on this DS blog continually dissecting the supposed nuances of the Cormen-Drosten/WHO mandated RT-PCR testing regime. It’s a fraud, was a fraud on day one of a 3 day process from “scientific” publication to compromised “peer review” ( involving at least one conflicted interest undisclosed ) on day 2 to WHO approval on day 3 with a WHO direction to all adherent countries that it is to be used as the “Gold Standard” mass testing regime worldwide ( only for the WHO to reign back hard, twice, reference the Bulletins in/around Dec 2020 – so inconvenient to Johnson/SAGE, they appear to have ignored them – “I wonder why?”) Tweaking or tuning a fraud is irrelevant – it remains a fraud; is it because people have short memories or are so assaulted by the continual government/SAGE/PHE driven rhetorical PCR test drivel that by osmosis this fraud becomes “accepted” fact?
FFS Wake up!!!
What does the Delta variant look like?..distinguished by it’s subtle differences?…and how do they find it?.. What new sorcery is this?
(I know, too many question marks)
apparently it looks like a syringe
“the whole Delta surge”
This adoption of a key propaganda meme is really irritating.
This is actually just a normal evolutionary replacement by a dominant minor variation – not some sudden unexpected increase of viral presence – a presence that has never been epidemic, in fact.
It is actually part of the normal process of a semi-novel virus becoming endemic and less virulent (see Gupta’s video on herd immunity).
The main worry is the possible disruption of this normal process by an absurd programme of ‘vaccination’.
The silver lining of the jabs being piss poor is that they probably aren’t disrupting that process after all.
This is a 72% reduction in mortality including any reduced risk of infection, not in addition to it. It continues to be an encouraging figure, albeit lower than earlier studies have suggested, and dropping week on week.
This is a key figure and one which will encourage a further push on vaccines. Although, the 72% figure appears to be part of a declining trend I’m not sure that is now the case. Figures for recent weeks suggest the decline has stopped – or slowed appreciably at least.
The AZ vaccine will not prevent infection but will probably reduce Covid deaths by about 70%. But is this any better than Ivermectin?
“It continues to be an encouraging figure” [72% RRR]
Not really. As pointed out earlier this week re. actual (alleged) differences in mortality from PHE data – the real life ARR advantage is minimal – in line with the early findings of real test data of around 1%. Certainly not enough to balance the risks and he unknowns.
A massive problem with these analyses is that the only attempt at taking into account confounding factors is dividing into over-50s and under-50s. It takes no account of factors such as ethnicity, deprivation and type of job – which are known to both be correlated with vaccine/no vaccine and to affect Covid susceptibility. Also stratifying into just two age groups is too crude – for example the most recent Zoe analysis shows that the infection trends in 20-29 are very different from trends in 30-39 which in turn are very different from 40-49. Perhaps the biggest confounder is that the unvaccinated are more likely to have had a prior infection and therefore natural immunity.
The data is not there so Will cannot be expected to allow for these confounders but that doesn’t make his analysis valid.
There isn’t a “massive problem”. If the PHE data is correct then Will’s numbers are likely to be in the right ball park.
It’s quite possible that there are confounding factors, but if you’re suggesting that protection from infection for over 50s is 75% rather than 7.6% because of a ‘confounder’ then that confounder would be so obvious it would jump up and bite you on the arse.
Also, if such a confounder exists then the fault lies with PHE who will have presented the data inappropriately. They should make it clear that any comparisons are not valid.
We get the same BS with the dozens of Ivermectin studies which all point in the same direction. Somehow, lead researchers from all around the world, despite having no possible financial gain, have all introduced ‘confounders’ which just happen to dramatically swing study results in favour of Ivermectin.
A confounder can make a massive difference. An example from my medical stats textbook is this study on the effectiveness of keyhole surgery versus open surgery on kidney stones . It appears to show a large benefit for keyhole surgery (Odds Ratio 1.34). But if you allow for the size of the kidney stone then this is completely reversed both for small and large kidney stones (OR 0.93, 0.81). The reason being that surgeons were more likely to use keyhole surgery on small kidney stones and operations on small kidney stones are more likely to succeed.
If there are one or more confounders then it could not possibly jump up and bite your arse because the data simply aren’t there. If you were shown data on surgery types and kidney stone outcomes there would be nothing jumping out of the data to tell you there was a massive confounder.
Also, if such a confounder exists then the fault lies with PHE who will have presented the data inappropriately. They should make it clear that any comparisons are not valid.
These are technical briefings. They are made available to the public for transparency reasons but the intended audience is the technically competent not the general public.
We get the same BS with the dozens of Ivermectin studies which all point in the same direction. Somehow, lead researchers from all around the world, despite having no possible financial gain, have all introduced ‘confounders’ which just happen to dramatically swing study results in favour of Ivermectin.
If you think the papers are wrong then explain why. Anyway the bigger problem with Ivermectin studies is that some of the high profile positive studies are turning out to be highly dubious.
An OR of 1.34 isn’t particularly large and there is a clinical reason why the result could reverse.
There was an initial claim of 80% plus protection from infection from the vaccines. This is a simple unambiguous endpoint. What’s more the early data (Briefings 14 & 15) suggested that high levels of protection were being achieved.
Same data – same methodology – shows infection protection waning.
They are technical briefings which can be accessed by anyone. PHE would have anticipated how data might be used.
Which ones are turning out to be dubious – and why would anyone bother? I can understand why there are some who would like to make dubious claims in order to debunk the success of Ivermectin. Have you read Pierre Kory’s response to the critics. P
Anyway, Uttar Pradesh (Pop ~240 million; Fully vaccinated 6%) seem to be happy enough with Ivermectin. Over the past 7 days
New Cases average; 17 per day
New Deaths : 3 per day.
90% of regions now Covid-free.
An OR of 1.34 isn’t particularly large
Whether an OR of 1.34 is large or not depends on the context – but the point is the change in OR – the confounding factor reversed the implication of the evidence from suggesting keyhole surgery was better than open surgery to the opposite.
and there is a clinical reason why the result could reverse.
So what? There is usually a reason for a confounding factor. The trick is to spot it and allow for it – which Will has not done (and cannot do with the available data).
There was an initial claim of 80% plus protection from infection from the vaccines. This is a simple unambiguous endpoint. What’s more the early data (Briefings 14 & 15) suggested that high levels of protection were being achieved.
Same data – same methodology – shows infection protection waning.
I don’t dispute the effectiveness of the vaccines is waning – neither do the PHE – if you look at the most recent vaccine effectiveness report (still in preprint) it explicitly makes this point. It is just the waning is not nearly as strong as Will concludes. Note that the vaccine effectiveness reports do allow for a wide range of confounding variables.
Which ones are turning out to be dubious
These are the two examples I know about.
1) https://www.medpagetoday.com/special-reports/exclusives/93658
I expect you know about this one. It was even covered here (and accepted as fraudulent).
2) https://www.isglobal.org/documents/10179/6022921/Patel+et+al.+2020+version+1.pdf/fab19388-dc3e-4593-a075-db96f4536e9d#:~:text=In%20COVID%2D19%20illness%2C%20critically,in%20those%20treated%20with%20ivermectin.
retracted because of implausible data. (Patel has a bit of a track record of publishing dubious research.) Tim Spector gives an explanation here.
– and why would anyone bother?
I don’t know – fame and professional advancement, political commitment?
Have you read Pierre Kory’s response to the critics.
No. Please give me a link.
Anyway, Uttar Pradesh (Pop ~240 million; Fully vaccinated 6%) seem to be happy enough with Ivermectin. Over the past 7 days
New Cases average; 17 per day
New Deaths : 3 per day.
90% of regions now Covid-free.
Which is great – but that doesn’t have to be down to Ivermectin. Lots of countries and states are getting low figures without using Ivermectin and UP introduced extensive lockdown measures at the same time.
I am not ruling out Ivermectin as either prophylatic or cure.. However, the evidence at the moment is inconclusive and clouded by fraudulent/dubious research. As I am sure you know, there is a professional large-scale trial underway. Let’s see the results. I really hope it works
I’ve noticed that comments are sometimes downvoted because they are appear complicated at first reading – ie the downvoter thinks the poster is saying something in support of the “other side”
“the most recent Zoe analysis“
… yet more unvalidated data, on top of the unreliability of PHE data.
You are right that the issue of confounding variables are central to any analysis. But that cuts right through the question of validity both ways. As I’ve said – you can’t plait shite.
The massive confounder here is the confusion of vaccine effects with the evolution of the virus and herd immunity. It alone renders any conclusion invalid – especially when you start with invalid data!
This mess is what you get when you bugger what should be a serious, controlled test process.
One thing we do know, however, from the brief days of proper trialing however : ARR ~1%.
Another thing we know is that adverse events exceed those in any vaccine program.
And another : Covid is not a major problem.
‘Nuff said, I think, to draw only one conclusion.
A quick reminder. ARR depends on the absolute risk which varies dramatically according to the situation.
I wonder what is behind the downvotes? It is not as though my comment is open to dispute. You can’t work out the ARR without knowing the absolute risk and the absolute risk varies a great deal – particularly depending on the prevalence but also the R value etc.
I’ve got graphs which are a little bit more informative to way things are going. These are using the same data (Technical Briefings 17-23) as Will and includes the single jabbed and ‘unlinked’ cases.
The graphs on the left are cumulative whilst the ones on the right are for every 14 day period , ie the delta between the current data and the previous set.
Under 50’s Cases
Under 50’s Deaths.
Only 204 deaths here so I’m not sure what is signal and what is just noise really.
Over 50’s Deaths
Under 50’s Case Fatality Rate and Absolute Risk Reduction which looks like a big fat ZERO to me.
50 and over Case Fatality Rate and Absolute Risk Reduction. I don’t think the ARR is as high as double jabbed Joe Public probably thinks it is.
I wonder how many of 70+ years unvaccinated dead were in very poor health and too week to take the vaccine?
There does appear to be small benefit here.
The 0-50 and 50+ cohorts are not ideal really but they are all we have at the moment.
… and all hinges on the validity of the base data. And that’s before you get to the minimal size of purported effects. Again – ’nuff said.
We are back to all-cause mortality as the only reasonably reliable indicator of worth. And that isn’t implying any worth in the snake-oil.
Thank you for these graphs. Is there any indication, from these reports, as to the underlying health conditions amongst those under 50 who have “sadlydied”? They must know, if they know their vaccination status so, if they aren’t telling us, why aren’t they telling us? I suspect the answer is that nearly every person under 50 who has “sadlydied” had at least one comorbiditiy on their death certificate and, quite probably, more than one.
Hi Will. Screenshot of the deaths for the last 12 weeks by health condtion. The 40-59 overlaps unfortunately but it’s better than nothing I guess.
So 0-19 With a Condition is first, then 0-19 healthy 2nd. It then follows for 20-39, 40-59, 60-79, 80+
I make it
0-19 10 with underlying conditions, 2 without
20-39 80 with underlying condtions, 34 without
40-59 503 with underlying conditions, 106 without
The ratio of Healthy vs Underlying Conditions is interesting as it’s almost 2:1 whereas the cohorts either side of it are closer to 5:1.
I noticed 20-39’s seemed to be getting hit more recently and I was wondering if it was Vaccine related given the younger people have been the target of the vax campaign over the summer.
Thanks for this analysis, Will. This is probably the only site in the world where such an analysis can be published. It goes without saying that no reporter at a mainstream news organization would perform such an analysis. Or if such a journalist proposed doing such an analysis to his editors, he would be told he can’t.
By any measure, the effectiveness of the vaccines is far, far lower than had been previously advertised.
So now we are removing posts bit like facecunt
The wheels are seriously coming off now. I have even started to get through to my parents about boosters etc. They are finally coming round to the fact that they have been duped.
So not only are these vaccines completely useless but those who have followed government orders and had their jabs now have probably the next couple years waiting anxiously for the very real possibilty of serious mid-long term side-affects to surface.
I hope that two weeks in Mallorca was worth it.
I don’t think I can be the only person who thinks this, so while I appreciate Wills
statistical analysis, and I know that we need the truth behind the statistics, the fact is that the Median IFR for the age group 50-59 is 0.27 and the survival rate estimate is 99.7300….obviously it’s even better in the younger cohorts. With great respect, no one under the age of 60 needed any kind of vaccination in the first place…no one. And it seems to be a bit irrelevant to discuss effectiveness of 10% or 90% for something that most people didn’t need in the first place?
Can anyone clarify please? I seem to remember reading somewhere (so much to read!) that, for example, if two people fell into a Combine Harvester (say) and acquired Covid in hospital before dying, the fully jabbed guy’s death would be “death by combine harvester” whilst the un-jabbed guy’s death would be ” death with Covid” and used in the propaganda.
Then Covid deaths of the un-jabbed, already inflated with deaths of single-jabbed being immuno-compromised, is further “improved” by the deaths with Covid.
I don’t think that is true in the UK, but PHE are at great pains to remind people that vaccinated people dying by/with/from covid have underlying health conditions. They don’t seem so inclined to inform us how many of the unvaccinated have similar conditions. They must know so their silence is telling.
I simply don’t understand why people get herded into taking vaccines which don’t work, according to my betters, however this is the Covid Crusher which would stop this Covid Pandemic dead, if everyone practiced it and it is free, from me:
The Achilles Heel of Coronavirus, is while it is still in the developing stage as Coronavirus/Covid in the warm, wet areas inside the nasal passages of your head (nose) and before it gets to become Covid in your head and lungs, 10 to 14 days later. If Coronavirus is not treated with my free iodine salt clean water cure to flush out your nasal passages, as soon as possible, or during self isolation, it becomes Covid, which is where the money is. You cannot catch Covid! Always breathe through your nose and keep your mouth shut, because you really don’t want the Coronavirus to seed itself in your lungs!! My free salt water cure has “absolutely nothing” to do with mRNA test vaccines. Treating Coronavirus with my free iodine salt clean water cure, flushes out the nasal cavity and kills Coronavirus, before it gets to be Covid, irrespective of if you have had mRNA vaccines or not. Mix one heaped teaspoon of iodine salt in a mug of warm or cold clean water, cup a hand and pour some of the solution in, then sniff or snort that mugful up into your nose, spitting out everything which comes down into your mouth, by so doing, you flush out your nasal cavity, where Coronavirus lives. If you get a burning sensation (which lasts for 2-3 minutes) then you have a Coronavirus infection.When the soreness goes away, blow out your head with toilet paper and flush away, washing your hands afterwards and continue doing my salt clean water nasal cavity flush cure, morning, noon and night, or more often, if you want, until, when you do my free salt water cure, you don’t experience any soreness at all in your nasal cavity. While you are at it, swallow a couple of mouthfulls and if you get a burning sensation in your chest, then you are killing the Covid/Bronchitis there too, so keep it up, each time you do a salt water sniffle, until the soreness in your head and lungs goes away – job done. Pour some of the solution on a flat surface and allow to dry and see what you have then. This is what coats the nasal passages in your head and kills Coronavirus/Covid off. You can see why it is so effective. This is what I have done for the past 27 years and I am NEVER ill, nor do you need to be either.
Please pass it around to everyone who wants to give it a try.
“Even so, a key issue is that the current vaccines block severe disease but do not prevent infection, said Dr. Gregory Poland, a vaccine scientist at the Mayo Clinic. That is because the virus is still capable of replicating in the nose, even among vaccinated people, who can then transmit the disease through tiny, aerosolized droplets”
Reuters – what my free salt water cure stops.
He added that “Current vaccines are great at preventing [CO1] serious infection deep in the lungs, but not at blocking infection in the upper airways. What’s needed is a nasal-spray (vaccine) that would stop the coronavirus from taking hold at all.” – what my free salt water cure does and stops.
No soreness when you do it, it feels like you are flushing your head with water, if you get sore reaction, you have a virus so deal with it, exactly as I have described above – did a sniffle today – Me, all OK!!
We all need a cure which works instead of these vaccines, when you get a Coronavirus infection – now you have one.
Do not use saline water bought online, use iodine based kitchen or sea salt, it is the iodine in the salt which kills Coronavirus dead
More to the point, try it on anyone with a Coronavirus infection and see what happens to the virus and how quickly it is killed in the nasal passages of the head. No Coronavirus, no Covid it would otherwise become. – Simple
Keep safe – Richard (smile)
I use a neti pot with sea salt a couple of times a week
Why would we expect the shots to show efficacy? None of the “treatments” so far adopted have shown efficacy: lockdown, masks, denial of early outpatient treatment, denial of known effective drugs, delivery in hospitals of toxic drugs and counterproductive interventions. The shots fit right in, doing more harm than good.
What Delta variant? Antibody Dependent Enhancement variant!!
Will, you mention that the results in the younger age groups may have been skewed by the less healthy people being vaccinated first. Is it possible the over 70’s results may have the opposite bias with the healthiest people most likely to be unvaccinated?
Thanks Will again for your articles. These are now quoted all over the world. Your articles are the main attractions for many now using DS worldwide.
In essence, this data shows that selected high risk vaccination from this new vaccine was the most prudent way to take and at the same time intensive vaccine safety monitoring. They instead opted for mass vaccination in the ludicrous belief that herd immunity could be achieved. We have now a monumental problem with risk benefit negative for healthy people and a coercive vaccine mandate sending further healthy people to an unacceptable risk.
The vaccinating doctors had earlier the concept “relative contraindication” for vaccines ie each individual was assessed due to health background and a decision to vaccinate or not was due to risk benefit. Difficult to find a vaccine more in need of that approach then the covid vaccines.
Coming in late to comments I want to add that treatment protocols for vulnerable people are nuanced and tailored – listen to Dr Zelenco describe how Ivermectin et al. are only used at certain stages of illness to maximise effects. He’s had zero deaths and his protocol is widely used – among many other proven effective treatments – my point is the jab is and always was entirely unnecessary and it’s use has killed millions more people (aside from side affects) by stopping such nuanced cheap safe treatments- so to me all of this fighting over unreliable statistics about a poisonous jab based on an unreliable test is entirely missing the point.
I would ask that DS be a little more careful with headlines because this one can IMO be labelled as clickbait. Sure the word infection is mentioned at the end but when I saw this headline first, I assumed that effectiveness against death was down to just 7.6%. Would have been better to read:
“New PHE Data Shows Vaccine Effectiveness Against Delta Infection Down…”
Now you may counter this saying I needed to spend the time reading the text and usually, I do pour over this long data heavy DS articles. But not always.
But can I also remind DS of the epiphany that they had sometime in the autumn last year that you’ll never win hearts and minds by trying to counter with pages of facts and numbers when the other side have the moral high ground and are arguing emotionally. I agreed 100% with this observation but it doesn’t have seemed to have made much difference. I’ve read DS nearly ever day but maybe step back and consider if this data-heavy approach is helping.
This one really would have benefited from an executive summary
Let’s not kid ourselves, there is no benefit to be expected from any of the ‘vaccines’ because they were only developed to cause harm, not to help.
No evidence of that yet.
Cockup and regulatory capture (aka corruption), yes.
The pharma industry profits from chronically ill people who spend their last 50 years or so (say from age 25 to age 75) drugged up to the eyeballs. Dead or healthy people are very bad news because drug sales drop to … shock horror … *zero*.
Confounding factors:
The ‘cases’ comparison assumes vaxed/unvaxed are equally likely to take a test and report a case. However surely the vaxed are more likely to be hypochondriacs who test every time they feel slightly funny whereas unvaxed are less likely to test every sniffle. Hence vaxed ‘cases’ will be over represented and unvaxed cases under represented.
Another factor is PHE assumption about the total UK population: Their count of vaxed people is accurate but their estimate of the number of unvaxed is likely way off by 10 million or more due to an underestimate of the UK population. This will further diluting the vax effectiveness against infection.
When you take these factors into account the vax ‘effectiveness against infection’ likely drops to zero.
There are similar confounding factors against the ‘effectiveness against death’. eg. In my family 2 people have chosen to skip the vax because of other health issues which put them at higher risk of a bad reaction to the vax. ie. the older unvaxed may generally have a higher % of co-morbidities than those that choose to take the vax – and this will lead to a higher number of deaths in this group – regardless of Covid.
Split this out to include part vaxed sep esp the deaths – a new picture emerges
Typical rubbish data. How many vaccinated people are getting tested. I would say less than 10%. I don’t know anybody who has had a recent test that has been logged by NHS or any other body that feeds into this data. Quite a few may have taken a home lateral flow test, but if it’s negative, as almost all are, there is nothing to report. The only people who present for a test already feel they may have Covid-19 symptoms, so the result of infection is bound to be high. I’m disappointed that DS presents this rubbish data without this caveat. I’m not a fan of these big pharma companies who presented highly optimistic results of their vaccines, but I would still expect them to be in the 70% range similar to flue vaccines and I expect any accurate data would show they are and even if it’s a bit less than that they are still having an important effect on outcomes.