
Were there worrying levels of mortality in 2022? The consensus is there were, with different people blaming various factors for the elevated deaths – many of which were due to cardiovascular issues – since the spring, including missed treatment, the NHS crisis, Long Covid and the vaccines.
My colleague Dr. Noah Carl has been sounding a lonely note of calm, arguing in two recent posts that mortality in 2022 was not elevated once you take the ageing population into account.
He notes that “2022’s age-standardised mortality rate [ASMR] was the third lowest ever, and age-adjusted excess mortality was negative (fewer people died than normal, after taking account of ageing)”.
He allows that “the latter half of 2022 did see non-trivial excess mortality: the ASMR was about 5% higher than the five-year average”. However, he counters that “the first half of the year saw negative excess mortality: the ASMR was about 6% lower than the five-year average”. He suggest that this means “the positive excess mortality in the second half of the year could be due to ‘dry tinder’: fewer people died in the first half, so there were more at risk of dying in the second”.
The problem with Noah’s argument is that it rests entirely on the use of ASMR. ASMR is a modelled quantity that adjusts the raw data using the 2013 European Standard Population to “standardise rates“. The impact of these modelled adjustments on current excess death figures is huge. For instance, the ONS states that in 2022, the “second leading cause of excess death in 2022 was ischaemic heart diseases (2,383 excess deaths; 4.5% above average)”. However, once adjusted, the ASMR was “significantly lower than average (96.9 and 99.3 deaths per 100,000 people, respectively)”. Using the ASMR has more than wiped out a 4.5% excess in heart deaths – a concerning signal – and turned it into a below-average year where there is nothing to worry about.
The massive adjustments using the ASMR can be seen in the ONS chart of excess deaths for 2022 by month below, where the dark blue bars are the raw excess and the light blue bars are the ASMR excess.
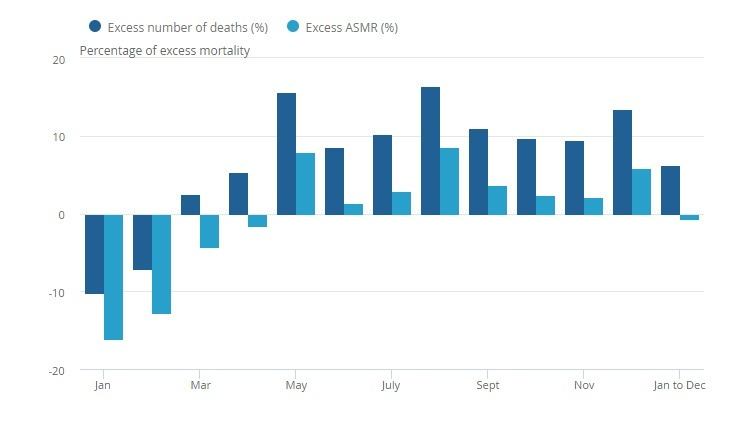
It’s clear from this chart that, firstly, raw excess has been running high since March, and the annual figure (the bar on the far right) is only lower because of the lower excess during the winter in January and February. As was noted at the time, this low winter excess was primarily a result of the mildness of Omicron and the absence of flu.
The second point is that the ASMR values are far below the raw data; the adjustments this model is making are immense, cutting excess figures to a fraction of their original value. So how confident can we be that such heavy adjustments are warranted?
It turns out, not very confident at all. The ASMR makes assumptions about how much older on average the population is getting each year and how frequently people are dying. Since the adjustments are large, this means the model assumes society is ageing very fast and this ageing is having a large impact on mortality rates that needs to be allowed for with heavy downward adjustments. So let’s check. Do crude annual mortality figures per 100,000 population show this claimed large impact of ageing?
Here are those figures for the past 30 years.
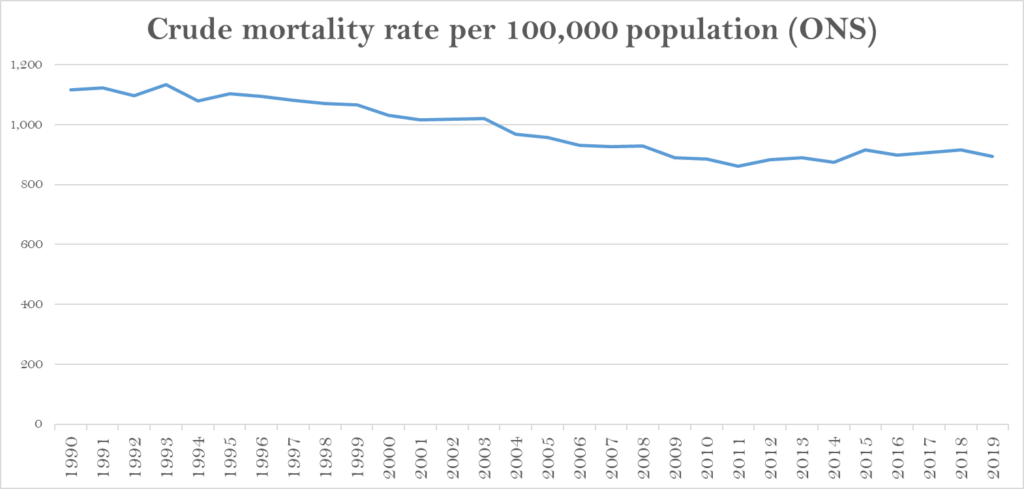
Clearly there is no evidence here of an ageing population causing a significant uplift in death rates, which have been flat since 2008 when the long-term declining trend ended. Further evidence that it is not due to an ageing population is that the cause of the deaths is not diseases of old age such as Alzheimer’s and Parkinson’s, which are running below average, but largely cardiovascular; it is also occurring in younger age groups. This means there is no clear justification for making severe downward adjustments to the raw data for 2022 based on the modelled effect of an ageing population, which appears here to be entirely hypothetical.
Professor Norman Fenton is similarly unimpressed with the move. He told me: “The ASMR is ultimately just an opaque ‘model’ that relies on multiple unverifiable assumptions about the true population and its age distribution.” He looks at some of the issues with ASMR in this video.
But could the high heart deaths just be a result of ‘dry tinder’ from the mild winter, as Noah suggests? If so, it would be a very fast effect. Is this what normally happens – does a period of negative excess tend to lead straight away to a period of high excess as deaths catch up? This would rest on the assumption that those who die of ‘winter flu’ typically would die within the next 12 months anyway, so any mildness in winter will normally be followed by a high number of deaths during the rest of the year. So is this the case – does a dip in winter typically lead to a large wave of deaths during the rest of the year?
It didn’t in New Zealand in 2020-21. During autumn and winter 2020, as pandemic restrictions were imposed and flu disappeared, excess deaths plummeted to minus-15%.
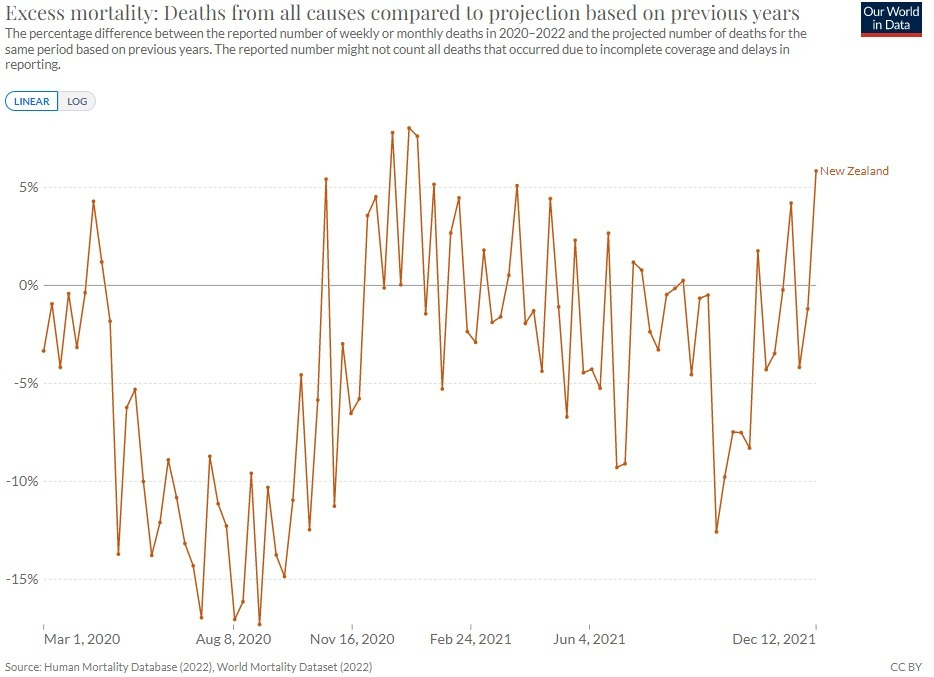
Clearly, many people survived the winter who normally would not. So did they all then die during the following year? While excess mortality during the summer reached around 5%, it then soon declined into negative territory again and remained there. This is a clear counterexample to the claim that mild winters are necessarily followed by waves of high mortality owing to an instant dry tinder effect, and thus that such an effect can be assumed to explain the excess deaths in 2022 in the U.K. It appears that dry tinder effects may not be so quick and dramatic – at least not when there is no novel pathogen involved.
It’s safe to say then that deaths were indeed worryingly high in 2022, particularly since the spring (and have continued high in January 2023). There is no reason to think that this is just because the population is ageing – a hypothetical effect which made no noticeable impact during the preceding decade, so cannot be assumed suddenly to have done so in 2022.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
What should also be looked at is the age distribution of those excess deaths. In the same way the “quality years of life lost” are used to assess the cost/benefit of a proposed treatment, maybe the same strategy should be used regarding excess deaths.
Coldly logical it may seem, but 10 extra “died suddenly” events in school children (10 x 70 years lost) is far worse than 100 “died suddenly” events in octogenarians (100 x 5 years lost), for example.
Whether or not QUALYs lost is a measure of quality, it is useful as a measure of something badly wrong. You don’t have to put a figure on a child’s life to know that children dying is abnormal and bad.
See here
In addition to excess deaths since the summer of 2022, there’s this – posted here by ebygum a couple of weeks ago, which deserves repeating – it’s a recent report by the obviously highly reputable Institute for Fiscal Studies:
“In summer 2021, each month 15,000 or so working-age people started a PIP claim. That monthly figure had remained little changed for years. It then steadily increased, such that by July 2022 (the latest data) it had doubled to 30,000. This report investigates the increase.”
Why would this be happening?
https://ifs.org.uk/sites/default/files/2022-12/The-number-of-new-disability-claimants-has-doubled-in-a-year-IFS-report-R233.pdf?fbclid=IwAR1k-a8Om62k8oxzlRqcMbmBf9Rk-JKuIMNvnWST-i3VmnM8SnJtbenITyw
Yes…it seems to me that there is confirmation evidence to show that deaths and injuries are excessive…and it’s coming, not just from Government ONS or UKHSA, but from different data sets….like the PIP claims, and insurance claims for instance….
I’ve posted Dr John Campbells video below in my comment…for UK/insurance…
..this is from the USA insurance stats’…
https://www.zerohedge.com/markets/where-did-all-workers-go
Clearly prior to 2020 mortality was coming down and coming down at a rate greater than the effects of increasing population size and an ageing population, and so raw death numbers were numerically reducing too. That trend couldn’t continue for ever or else based on that existing trend we’d all be immortal at some time in the future, but at the same time an abrupt turnaround couldn’t be expected.
What has always surprised me is that people have been living for longer. I’ve never understood why that was in the context of a population of seemingly worsening health with higher metabolic illness. I’ve tentatively put it down to us being better at prolonging life at the very end of life rather than increasing healthy lifespan. But the honest answer is I don’t know.
Without understanding why mortality has been coming down to 2019, it’s hard to say how long we would have expected the trend to continue. But to assume a future trend of no improvement after such a long period of mortality improvement seems a strange starting assumption for Noah Carl to be using, but that ultimately is the assumption he’s using in claiming 2022 was a normal year.
We have significantly high mortality in working ages even after adjusting for population and looking at age stratified data.
Given that, what is most likely that the excess mortality caused by experimental vaccines and lack of access to healthcare etc only affects those of working ages and not those over say 75 or that there is some effect like a lack of ‘dry timber’ in the oldest ages because of the ravages of the last few years. I think the latter is the obvious starting assumption.
‘ I’ve never understood why that was in the context of a population of seemingly worsening health with higher metabolic illness. I’ve tentatively put it down to us being better at prolonging life…’
i have.
Propaganda from the experts and vested interests misleading us into believing the situation is worse than it is to serve their own interests, just like all the propaganda about masks, lockdowns, protecting granny, vaccines that aren’t, climate change, lies about cholesterol, eating meat, sugar, salt, saturated fats – quite a list.
I just wonder how many more lies do people have to hear before the penny drops and they stop listening.
Where is the Matrix Cat? Are we in a parallel universe? LOL!
Just put this on the ‘other side’ Dr John Campbell and the worrying rise in excess deaths in the 20-44 age cohort in comparison with 2019…using insurance actuary data…something that Ed Dowd in the USA has used to show massive increases in death and disability…..
There seems to be more than one source of data confirming a rise in all cause mortality!?
https://www.youtube.com/watch?v=OD0na_NZaLM
I’ve got a great idea.
Why don’t we just differentiate vaxxed v. unvaxxed re the apparent increase in deat rate.
But the ‘vaccines’ was going to ‘save lives’ particularly of the ‘most vulnerable’.
Never mind the age-adjusted malarkey and percentages, it still doesn’t explain why so many more ‘saved lives’ died in the vaccinated group when we were categorically assured they would not.
If people are going to die anyway, what’s the point of the ju-ju medicine?
It is a grim picture from an economic point of view. The workforce is going to become severely diminished and incapcitated, at least terms of quality whilst at the same time less pressure on housing and employment will bring no relief in terms of inflation which is now essentially a perfectly calibrated extract and control mechanism. We are being funnelled into this reality at an alarming speed and yet we fail to understand the urgency and we are so dependent on these systems that we struggle to formulate a path of resistance.
The work force has been diminished and incapacitated gradually since the British Socialist Party took over in 1945 with the promise of Utopia.
Borriwing from the apocryphal reply attributed to Pope John… how many people work in Britain? About half of them.
We now have nearly 50% of the work-able getting a wage fir jobs that create no wealth, in jobs of such low productive output they need State welfare top up, peopke who just don’t work at all and get benefits.
It’s called Socialism – that Faustian pact where people stupidly sell their Souls – delayed payment – for the instant gratification of a life of State provision, safety and security.
If you have a heart problem there are three herbs that you might want to consider: hawthorn and Arjuna and danshen or red sage. All of these are being investigated by big pharma but it is worth investigating these substances.
And what’s going on in Scotland? Just in December 2022 they saw a 10% rise in excess deaths and 15.6% decrease in births. England and Wales have an excess death rate of 23.1% in week 1 this year.
https://nakedemperor.substack.com/p/scottish-excess-deaths-reach-29
And add into all the comments below Ed Dowd’s reporting of a global average of 29 deaths on the field of sports people before 2021 and now it’s huge numbers every month. (See James Delingpole’s podcast with Edward Dowd, 22/1/23).
‘… this means the model assumes society is ageing very fast and this ageing is having a large impact on mortality rates…’
But if all the ‘dry tinder’ got used up in 2020 & 2021, the population would be on average be younger having lost a significant portion of its ageing people.
‘He told me: “The ASMR is ultimately just an opaque ‘model’ that relies on multiple unverifiable assumptions…’
Isn’t this what is now called: The Science™️
It certainly was the basis for the ‘pandemic response’ and underpins the climate change scam.