
There have been 16,631 excess non-Covid deaths registered in England and Wales in the 18 weeks since April 23rd, according to the latest official data from the Office for National Statistics, released on Tuesday. This is 9.8% more than expected, based on an average of the previous five years. Overall excess deaths, including Covid deaths, have been 13.4% higher than expected during the period.
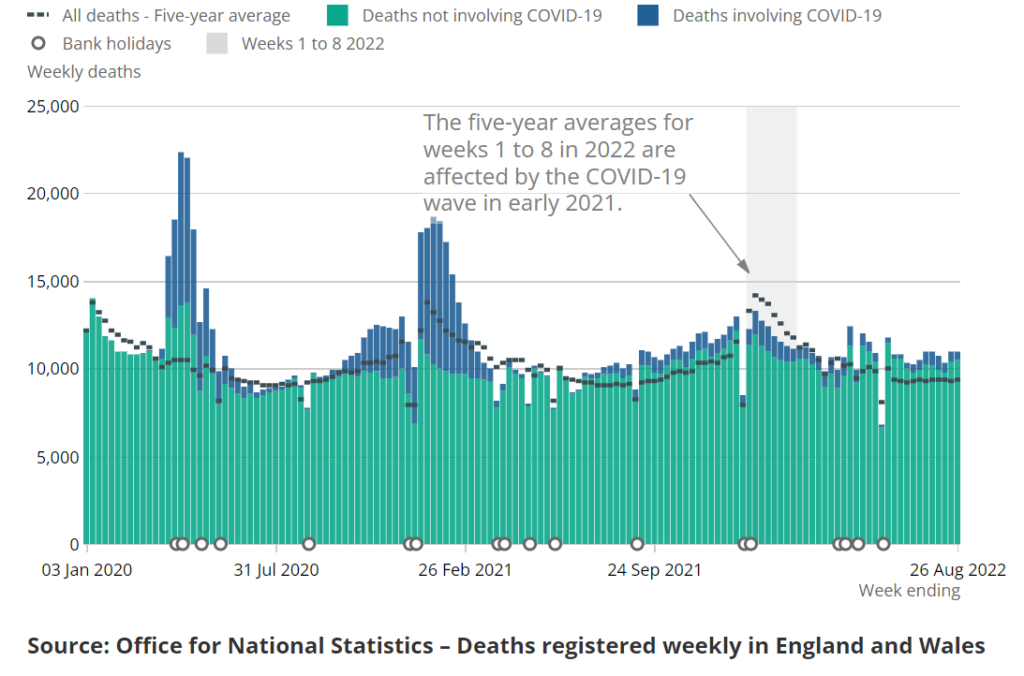
In the week ending August 26th, the most recent week for which data are available, 10,942 deaths were registered in England and Wales, which is 1,556 (16.6%) above the five-year average for the week. Of these, 453 mentioned COVID-19 on the death certificate as a contributory cause and 282 mentioned COVID-19 as underlying cause, leaving 1,274 deaths from a different underlying cause.
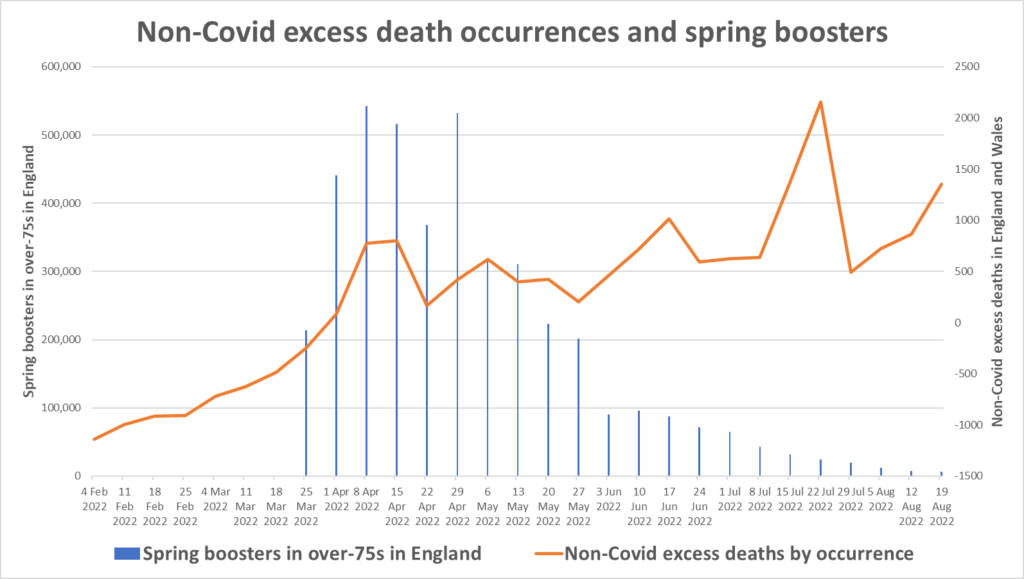
At the Daily Sceptic we have been following what appears to be a correlation between the spring fourth dose booster rollout among over-75s in England and a wave of now over 16,600 non-Covid excess deaths that are currently unexplained. Vaccine researcher Dr. Theo Schetters has highlighted a similar correlation in the Netherlands and raised concerns that the vaccines may be contributing to the deaths.

As noted last week, the correlation in England and Wales, which was strong during the spring and early summer, has not continued, as deaths have remained high while booster doses have tailed off, as depicted below in the chart showing deaths by date of occurrence. Deaths spiked once again during August, for reasons that are unclear. The continued high excess deaths may be an indication of ongoing vaccine injury, perhaps in conjunction with the effects of previous Covid infection, or the operation of another cause.
Freddie Sayers this week in UnHerd has interviewed actuary Stuart McDonald, Head of Demographic Assumptions and Methodology at Lloyds Banking Group, to get his insights into what’s going on. McDonald says it is an “undeniable fact” that more people are dying than we would expect. This means he agrees it isn’t just due to an ageing population. It’s also worth noting that the displaced mortality from the 150,000 excess deaths of the last two and a half years means we should be seeing fewer deaths right now, not more.
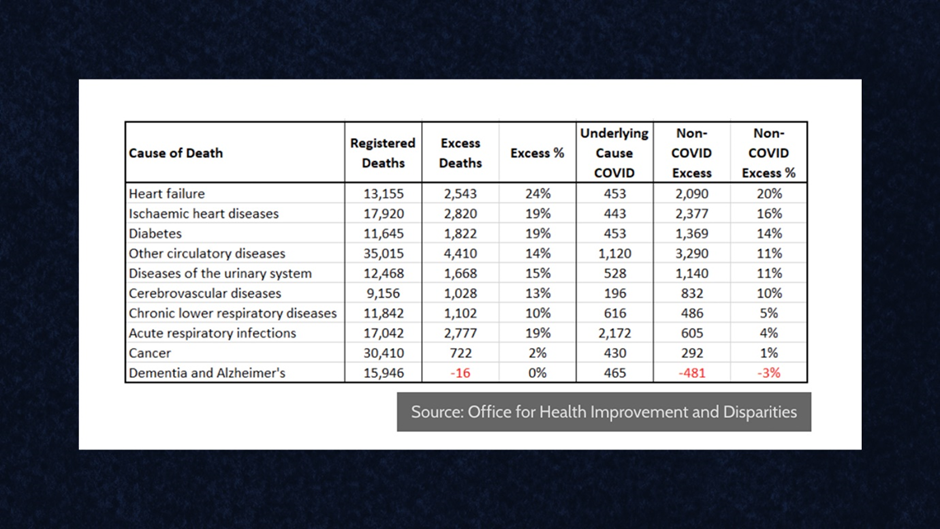
McDonald states that the cause in the majority of cases is “cardiovascular, circulatory, cerebrovascular”. He acknowledges that cancer deaths are not running above average, though stresses he believes that these are coming down the line.
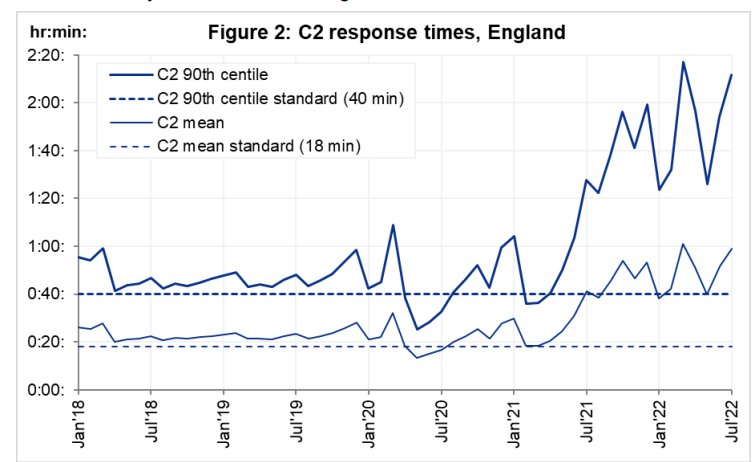
One of McDonald’s suggestions is that some additional deaths are being caused by the current ambulance delays, particularly when combined with the pent-up health problems of people unable to access medical care or avoiding doing so during the pandemic. He points to the fact that the target ambulance response time is 18 minutes whereas in July the average wait time was 59 minutes – a delay which, where strokes and heart attacks are concerned, may be a matter of life and death.
The problem with this explanation though is that it doesn’t engage with why there are long delays in the first place. There are long delays, in part, because there is high demand, as can be seen in the following two charts, where a sustained rise of around 20% in 999 calls from spring 2021 (coinciding with when the wave of excess non-Covid deaths began) matches the rise in waiting times.
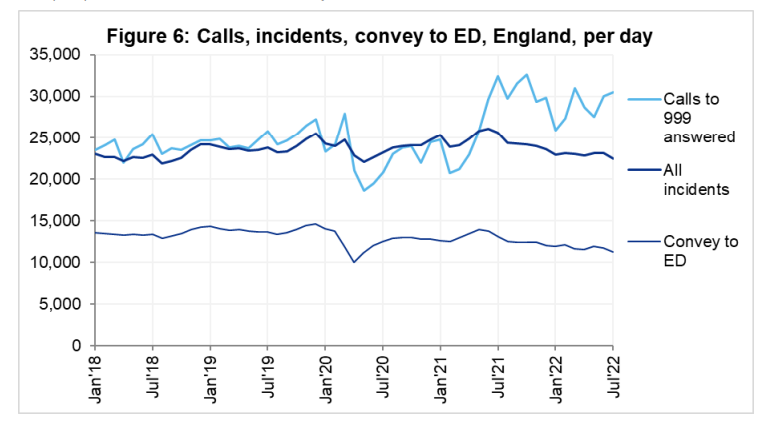
It seems reasonable to assume that whatever is driving the increased 999 calls is also driving the increased excess deaths during the same period, and that the increased waiting times, while they are likely exacerbating the situation, are not the underlying cause of one of the main things – increased demand – that is causing them.
It’s also worth bearing in mind that the survival rate for cardiac arrest at the best of times is under 10%, so, in that case at least, the impact of increased waits for ambulances on overall death figures will be marginal.
McDonald’s main suggestion is that it is COVID-19 itself that is driving additional heart deaths. He notes that post-viral cardiovascular issues are well-known and well-studied consequences of other viruses, adding: “We have historic evidence of elevated cardiovascular risks extending beyond the immediate acute infection, and we have pretty firm evidence that there are a sub-group of people who have had COVID-19 that will experience elevated cardiovascular risks.”
A difficulty with this theory is that the elevated heart deaths didn’t appear until mid-2021; they were not a feature of the first 16 months of the pandemic, during which there were two large Covid waves. This would suggest that Covid by itself is not a sufficient explanation. On the other hand, the wave of excess non-Covid deaths did broadly coincide initially with the Delta wave, which may indicate some relationship with the virus.
McDonald is sceptical that the vaccines are playing any major role. He argues that “the data consistently shows that the fully vaccinated have a lower mortality rate than those that are unvaccinated”, though which data he is referring to here is unclear. It is very difficult to get hold of all-cause mortality data by vaccination status. The ONS has released some, but as Professor Norman Fenton has pointed out, they are missing missing thousands of deaths and apparently misclassifying them, so cannot be relied on. Other official data suggest that the vaccinated are being hospitalised for non-Covid reasons at five times the rate of the unvaccinated.
McDonald insists that any elevated risk from the vaccines is “rare”, and states that “the vaccine has been very carefully monitored since its rollout”. Is that really the case, though? Certainly in Israel it’s recently been revealed that the Government only commissioned active monitoring and analysis of safety data a year into the rollout; and when it did look into it what it found was very alarming and it proceeded to cover it up. There is no indication the U.K. has done any better on this score.
How rare vaccine heart injuries are is also matter of debate. A Thai preprint of a prospective cohort study in adolescents found cardiovascular adverse effects in almost one in three teenagers and suspected or confirmed heart inflammation in one in 29 young males. Such a frequency of side-effects is usually defined as common or very common, not rare.
In truth, the vaccines remain a major contender as a contributor to a wave of heart deaths. Studies have shown that the coronavirus spike protein by itself damages the heart and that the spike protein can persist in the body for months following vaccination, causing immune system inflammation and debilitating symptoms.
Danish scientist Professor Christine Stabell-Benn analysed the vaccine trial data in a Lancet preprint and concluded that the data show a “potential danger signal” for heart-related deaths connected to the mRNA vaccines. Dr. Peter Doshi, a senior editor of the BMJ, also analysed the trial data and concluded the vaccines appear to be more likely to cause serious injury than prevent it. A concerned heart surgeon in Japan wrote to Virology Journal with a call for all Covid booster vaccinations to be stopped for safety reasons, citing in particular the impact on the heart.
To my mind, the only serious alternative explanation for a wave of specifically cardiovascular excess deaths in the past 18 months is some under-appreciated (and delayed) effect of the virus itself.
I don’t think these explanations are mutually exclusive; the impact of vaccination could exacerbate or be exacerbated by the effects of the virus. Either way, the question becomes which is playing the larger role: is it mainly the virus or mainly the vaccines?
My feeling is that this is the central question that needs to be answered by any investigation into the excess deaths, and that increased ambulance waits and delayed access to treatment, while having some impact, will not be the main drivers.
This means the investigation needs to get to the bottom of the vaccination status and Covid history of the deceased, and dig down into which of these is the major culprit. Are we looking at a virus that covertly kills thousands more than we think by attacking the cardiovascular system, or are we looking at a vaccine that does so? Unless an investigation examines this question fully and properly, it will not be worth the paper – or software – it’s written on.













To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
There will never be any sort of acknowledgement by the government/TRPTB that any investigation is taking, or will ever take place.
The reason why is simple, – because to do so would adversely affect confidence in the jab and give ammunition to lawyers.
This has been the stance of bigpharma re all vaccines for the last 40 plus years. You have no idea as to the amount of power and influence the criminal element amongst them hold.
And, I use the word “criminal” deliberately and accurately –
Pfizer – Bextra.
Merck – Vioxx
Johnson and Johnson – Risperdal.
In winter 2017/18 there were 50,000 plus excess deaths and no investigation, just a whoops, picked the wrong vaccine.
Stuart McDonald seems to be part of the vaxapologist cadre. It’s a shame Freddie didn’t challenge him on his brazen misuse of statistics and standard use of indefinite descriptors like “rare” and “unlikely” and “the data (unreferenced) clearly…”
These people are either stuck in mass formation or financial beneficiaries of Pharma/state/globalist funding.
The data Prof Norman Fenton analyses and that is unclear, shows an inexplicably elevated level of non covid deaths in any given age group, in the unvaccinated as compared with the vaccinated, when you would expect to see at the very least the same baseline level (at least that was the case when he did his analysis). For this reason he, rightly, mistrusts the data. It is pretty sure the Vaccines aren’t improving outcomes for non Covid causes, so what explains this? This indicates either the data is being massaged by the ONS or there is something fundamentally wrong with the underlying data categories.
I’m pretty sure I know that problem is and it relates to the overall UK population figure. The ONS has (quietly) revised immigration figures no less than three times now (doubling them two out of the three), indicating they were probably lying to us in the past about the true picture, or, being charitable, avoiding investigating the truth until it became unavoidable. So the overall UK population figure is shaky at best.
Vaccination rates are based on a definite or positive data, whereas rates for the unvaccinated are based on the figure for overall UK population minus that definite positive data. If you don’t know (or won’t admit) what the overall UK population is you don’t know what the numerator is for the unvaccinated. If the numerator is higher than you are admitting, then the “rate of x occurring per 1,000” will be correspondingly falsely high because the numerator is lower than it should be. So the “inexplicable” difference in baseline isn’t actually so inexplicable at all and actually corresponds with a matter the ONS already has form for “mis-analysing.”
I think Norman Fenton probably knows this, but is also aware that as an academic he has already taken as big a bite out of matter outside the Overton window, as any academic can chew without being treated like he is the next Enoch Powell.
Don’t forget that vaccinated as a status only occurs two weeks after the second injection. As far as I’m aware that definition has not changed and would therefore sweep jabbed as unvaxxed deaths for anywhere from 5 to 12 weeks after the first jab.
Im not sure wether the booster 3&4 have affected this miscatagorisation.
Are you using numerator to mean denominator?
No. But yes I should have analysed the numerator and denominator the other way round as then the calculation would be clearer.
As I have analysed it I’ve made the numerator the overall population of unvaccinated. The ONS figure is I suspect artificially lower than the real figure.If the real figure is bigger, the denominator as a proportion of the real population will also be correspondingly bigger (in this case absolute number of non covid deaths). So then you have a denominator that is out of proportion and disproportionately large compared with the numerator (unvaccinated population) the ONS are using. The result actually gives the frequency of deaths which when expressed as per 1000 of the population will be artificially high.
Sorry for expressing it this way as I now realise it isn’t the easiest to follow.
‘It is pretty sure the Vaccines aren’t improving outcomes for non Covid causes, so what explains this?’
Vaccinated people were being included in non-vaccinated. Anyone second dose who became infected within 14 days post-injection was considered unvaccinated. That means anyone who died within 28 days of day 14 was an ‘unvaccinated death’.
Further: the same deceit was used on boosted people, so that even hitherto ‘fully vaccinated’ individuals were counted as unvaccinated if death occurred within 28 days of day 14 post-booster.
This therefore increased unvaccinated deaths and decreased vaccinated deaths.
It is also the case that during the 14 day period post-injection and individual is more susceptible to infection, serious disease and death because of the stress on the immune system caused by the product.
What was deemed a non-covid death during the Delta wave? When Delta hit, it became apparent that the vaxx had failed entirely. It is not unreasonable to assume that whereas before there was no hesitation to attribute any possible death whatsoever to covid in order to scare people into submission, when (at that time) 2x vaxxed were dying during the Delta wave, to attribute most deaths of 2x vaxxed to covid would have damaged the vaxx push, which at that time was still going strong – let’s face it, they still managed to fool a large number of people into getting the 3rd pointless vaxx.
In other words, maybe a lot of excess deaths during Delta were in fact due to covid after all, it was just covered up as much as possible until they could find a way of explaining why as many if not more vaxxed were dying as unvaxxed. That excuse turned out to be that the vaxx was not as good against Delta and then Omicron, and many people bought that cop-out, even after they had initially said it did still provide full protection against serious illness and death for all variants.
In addition, there was always the risk of ADE. Last time I looked at the EMA list of potential risks, there was at that time (some months ago) insufficient information to determine whether the real risk of ADE would materialise or not. When Delta hit Europe, most people were 9 months or more from their last jab, with minimal antibodies. The vast majority of people have no idea about ADE; we know they have little information about the vaxx in general, about the serious AEs. Just think how they’d feel about the knowledge that the stabbers knew full well there was genuine risk that the vaxx would in fact make them more susceptible to infection and serious illness if ADE were to occur. I mentioned ADE to a neighbour, he didn’t believe the concept, even though I told him it was a known phenomenon, hardly something I had managed to dream up.
Either the excess deaths were due to covid, which was obfuscated due to unwillingness to admit complete vaxx failure (and absolute reluctance to give up the fab cash cow), or the excess deaths are related in some way to the vaxx – ADE, immune overreaction due to excess antibodies from vaxx combined with previous or subsequent infection, or the vaxx itself is simply toxic sludge.
I’m going to try to post my own graphs of this phenomenon. First, 10 years of England and Wales deaths, adjusted for both growing and aging population. The dark blue line skimming above all the others mid year, is this year
(I made this a couple of weeks ago but pattern hasn’t normalised since)
And the excess compared to pre covid. I think you can clearly see how the death displacement effect after a peak lasts only 3 or 4 months, reminding us how old and sick most were that succumbed to the pandemic.
Hope this helps. A third way to look at this year is the standard deviation from normal range. This makes what’s happening look most alarming
No, folks – we’ve been barking up the wrong tree all this time.
It’s nothing to do with the vaccines at all; (and let’s give a resounding cheer that clever scientists – no doubt with very generous funding from some saintly philanthropic people – have developed another wonderful vaccine for those poor souls in Africa against malaria) it’s been artificial sweeteners all along!
Just seen it on Talk radio so it must be true.
Tsk! All our cardiovascular and cerebrovascular problems must now be attributed to this obvious cause. How did we miss that one?
I think they’re really scraping the barrel with regards to what they can blame these excess deaths on! It would be farcical if it weren’t so tragic and outright desperate to divert our attention to other causes. The absolute codswallop we are expected to swallow is just mindblowingly insulting. It just stinks of lies and corruption. How many are burying loved ones with no firmly established cause of death, having to make do with a mere “cause unknown” on the certificates? So you can test positive for Covid within 28 days of being ran over by a bus and your cause of death is put down as “Covid” ( because ‘with’ and ‘from’ were never distinguished ) but if you die within 28 days of being jabbed it’s labelled as ‘SADS’ or reported as a ”coincidence”?! The crazy double standards never cease to amaze. Peter McCullough is always relaying the information that most people die within 3 days of being jabbed, but a causal link is never considered or investigated.
See the graph here on the bottom right and how it compares to the flu shot. A massive difference in deaths immediately after the shot vs 1 week later;
https://www.openvaers.com/covid-data/mortality
Yes, referee whistles being my favourite. If that was true, Vinny Jones would be long gone!
OMG ref’s whistles? I haven’t heard of that one. From the not so sublime to the incredibly ridiculous..Basically a total piss-take then!
Not climate change then?
If the culprit is the spike protein, then most of the excess deaths will be caused by the ‘vaccine’ rather than the virus itself. This would be because the ‘vaccine’ has been shown to spread throughout the body. Also, with the arrival of Omicron, I thought the spike protein has changed significantly from the original virus.
I think paramedics will know whether there is a correlation between patients with cardiac problems and ‘vaccine’ status and if the ambulance services are collecting the data, they will know as well.
The virus is mostly active in the mucosal cells of the nasopharynx or if unlucky the lungs. Virus that become systemic are attacked and destroyed by antibodies. The protein spike attracts T Cells whose function is to destroy the cells invaded by the virus to prevent reproduction, but these T Cells do not attack the virus or the protein spike.
The mRNA ju-ju is active in muscle cells in the upper arm – it is not a virus – so if it escapes as apparently it does and can remain active at least up to 60 days, it is not attacked by antibodies but will invade cells throughput the body which then attract T cells to destroy them.
So consider the mRNA gets into your heart muscle, for example, your own immune system is now going to destroy those invaded cells and thus destroy your heart muscle dependent on to what degree the muscle has been invaded by the mRNA.
The effectiveness of the mRNA is measured by antibody production, yet there is no measure of T Cell production which is front line defence.
T cells are preventative to stop viral load building, antibodies are mop-up, if you will, to kill virus that reproduced before the T Cells got control.
If the T Cells fail, it is unlikely antibodies will be of much use. For every one virus the antibodies miss, 100 000 copies will be made, likely to be a losing battle.
The whole way the so-called science of this is presented is questionable and seemingly calculated to mislead.
Thanks. Are T Cells the same as lymphocytes? If understand Dr Bhakti correctly another place in the body the mRNA products are likely to accumulate is in the cells that line blood vessels, which might be the cause of blood clots. So for people injected there could be damage created by spike proteins and immune reactions to previously healthy cells producing the spike proteins. In addition there is a suggestion the lipid nano-particles element of the injections could be adversely affecting fertility (Dr Malone) and any damage accumulates with each successive dose. I’m a lay person, but you seem to know you stuff. I’d be happy for any correction to anything I’ve got wrong.
Vaccine or virus?
I’d rather lay the blame on lockdowns; both the direct effects on people’s health (mental, physical, it’s all connected), and the indirect effects on their health from things like GP closures, interruptions to established prescriptions, cancelled surgeries and then the wider economic impact on people’s lives… the list goes on and on.
I know a lot of people who have become seriously depressed by the realisation of how authorities and their experts have ridden (and continue to ride) roughshod all over our basic human rights. This plays havoc with our health.
https://www.ohchr.org/en/human-rights/universal-declaration/translations/english
No doubt the effect of lockdowns is a cause of very many deaths, directly or indirectly. However, the harmful physiological effects of the LNPs and spike produced by having had the vax are indisputable, as evidenced by many scientific studies. I would stick my neck out to say that now we are in Omicron times, the likelihood of dying directly from a virus which is on a par in severity with the common cold, ( so not even flu. That was the original or Delta. ) is highly unlikely. If people were going to succumb then they would have done so way before now due to the increased pathogenicity of previous variants. And this is taking account of the fact that everyone ( and how could this not be the case, unless you were living like a hermit and avoided ALL contact with fellow humans and animals? ) has had Covid in one of its forms by now, therefore people will have some form of natural immunity to varying degrees ( because we know that in fast-mutating viruses such as the cold, you cannot build up immunity to just one strain then expect to not catch another cold, hence we can catch several colds within a 1 year period ). I think I’ve read that seroprevalence is >90% in the UK, if not other countries by now too. One could hardly call Omicron and its offshoots lethal.
There is also the question of just how damaged vaxxed people’s immune systems have become due to an onslaught of billions of LNPs over the course of several injections, which does presumably put them at a disadvantage when compared to an unvaxxed person who’s encountered the virus in the wild and generated a much more robust immunological response to the whole virus, not just the toxic spike part, therefore their body reacts to the repeat exposure as nature intended. So perhaps some of these disadvantaged multi-vaxxed will now be killed off by something as benign as a cold that they would never have been threatened by had they not had any mRNA injected, because their immune system cannot even cope with a mild exposure of pathogen and is now rendered dysfunctional. No doubt they will go down on the books as having died *of* Covid, when the jab was the culprit all along, because the symptoms will just be the same and nobody will be interested in reporting their vax status, thereby inflating so-called ‘Covid deaths’ and confounding the data.
I think the most frustrating thing is that we may never know just what, in terms of %, was the cause of these excess deaths. I mean, if you could produce a pie chart for excess mortality, what would it look like, in terms of our best guess? I don’t think we’ll ever truly know. The vast majority of excess deaths will always be blamed on the virus because that gets the authorities off the hook in terms of restrictions and coercion to get jabbed being a massive factor. They will always feel justified in their diabolical and hugely damaging public health proclamations because they’d just fall back on the old “It would have been so much worse had we not….”. Great we have Sweden as a handy control for the restrictions but pity we don’t have an equally handy country which never injected anyone, thereby acting as the ultimate control group in this global experiment, still ongoing. Now that would have been interesting.
The “vaccines” certainly have a lot to answer for, agreed.
It’s the variety of pathologies which tells me that, for a vast array of reasons (e.g. fear of “the virus”, fear of the rise of a totalitarian state) people have become terribly depressed, frustrated and anxious. This has a very detrimental effect on the immune system, resulting in an enormous range of new and exacerbated health problems.
I’ve said this before, but the key question is pretty simple: has there been a change in the age profile of the people who are dying from cardiovascular and other related conditions? If the age of death is unusually young relative to the last few years (i.e. the share of cardiovascular deaths is greater than it should be in the young), then we pretty much have our answer. It could just about be plausible that the virus would result in heart damage that we would then see playing out in deaths later on, but highly implausible that this would result in proportionally more young people succumbing.
Latest NSW data showing only 10 percent of Covid deaths in the past week being unvaccinated, and 80 percent having had 1 or 2 booster shots.
These figures change little week by week. Being an actuary (or doctor) doesn’t automatically mean one is immune to propaganda.
https://www.health.nsw.gov.au/Infectious/covid-19/Documents/weekly-covid-overview-20220903.pdf
Thanks. Perhaps I’m missing something here, but 10% deaths being unvaccinated plus just one unvaccinated patient admitted to hospital and zero admitted to ICU doesn’t seem to square with the statement ‘However, people who are not vaccinated remain far more likely to suffer severe COVID-19’.
40 years in medicine and I can’t figure that one out either!
all data relating to ‘covid’ are suspect. there are no pathognomonic clinical features of ‘covid’ – it cannot be differentiated at the bedside from many other respiratory infectious illnesses. the fundamental diagnostic fraud is that ‘Covid’ is medically diagnosed on the basis of a fraudulently upcycled PCR test, the ‘positive’ results of which are overwhelmingly false. the rare genuine positive PCR results cannot give any information about the origin of the amplified nucleotide sequences, which can come from any old fragment of goat or papaya (R.I.P. John Magafuli, Hero of The Resistance). while all cause mortality appears to be the single most reliable statistic, we must remember that with our British government and their venal World Economic Forum friends worldwide, we are dealing with egregious criminal psychopath fraudsters. the placing of all data relating to ‘covid’ under suspicion of criminal falsification accords with Lord Denning’s famous 1956 judgement that fraud vitiates everything it touches.
Can you imagine a “Scientific” process, by the same people who imposed the Lockdowns and coerced an experimental jab on millions of people who didn’t need it, admitting that the jabs are not as “safe and effective” as they continually told us they were?
No – neither can I.
Prof Bhakdi and other virologists, who weren’t bought and paid for by Big Pharma, warned them that the jabs were dangerous and predicted precisely the outcome we are now seeing. Prof Bhakdi specifically said that the jabs would cause blood clotting and said if you have one, don’t have a second. And for goodness sake, don’t have a third. HE has been proven right.
But Fauci, Ferrar, Whitty, Vallance and all the rest of the evil people will never admit it. And neither will the politicians who empowered them.
Lloyds Banking man eh? You can bet your bottom dollar that somewhere along the line there’s something fishy going on. Any connection to B&MGF, vaccine investment anyone?
Sorry don’t trust this guy he’s too near the establishment.
It’s only the five year average. Are there any excess deaths if you look at the 10 year average or the 20 year average?
There is another potential explanation for the excess deaths of course, which is that they resulted from the lockdowns. Possible mechanisms could be reduced exercise levels and increased loneliness.
Let’s say “best” case scenario, it’s not the jibby jabs. Do I now want one of those in my body? Hell no.