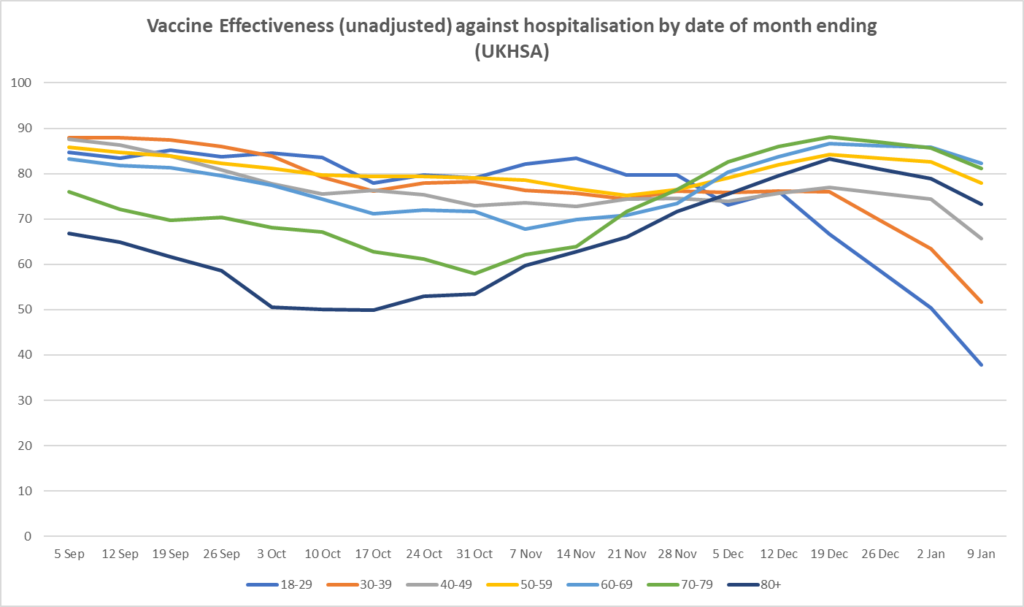
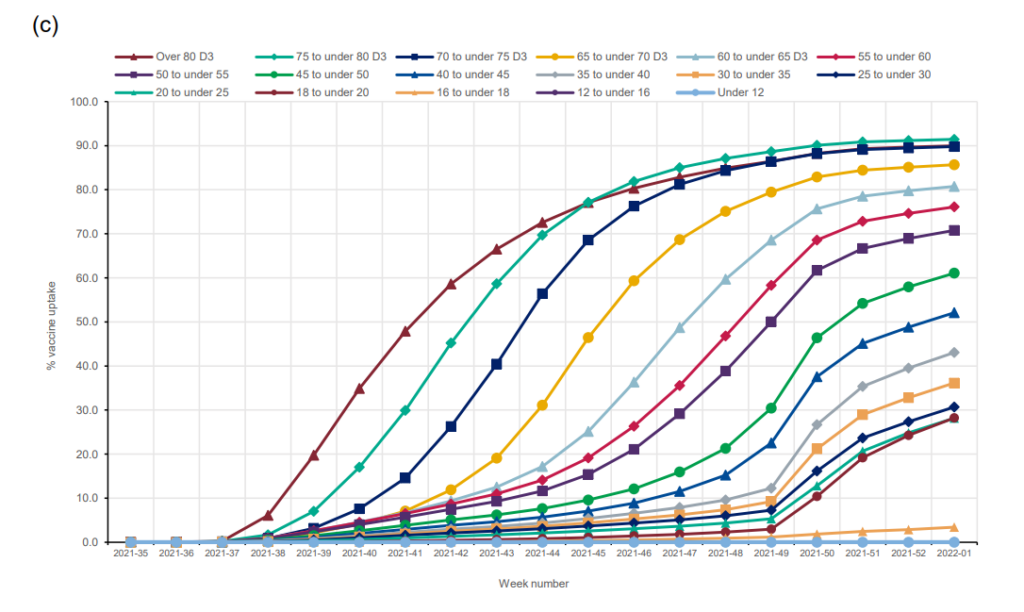
The most striking point from this week’s UKHSA Vaccine Surveillance report – with data for the four weeks ending January 9th – is the sharp decline in unadjusted vaccine effectiveness (calculated from raw data, so not adjusted for potential confounders such as risk factors and testing behaviour) against hospitalisation (see above). The decline is particularly sharp for under-50s, with 18-29 year-olds dropping to 38% (meaning the hospitalisation rate was 38% lower among the vaccinated (two or three doses) than the unvaccinated). The sharpness of the drops coincides with the age groups with the lowest third-dose coverage (see below), which suggests it may be a waning effect accelerated by Omicron and offset by boosters.
Another possible explanation is that it is an artefact of the high number of incidental hospital admissions in recent weeks, with more than half of Covid hospital admissions being treated primarily for something else. Given vaccines offer little to no protection (or worse) against infection, they will offer the same lack of protection against incidental hospital admission as Omicron spreads in hospitals or is found in those admitted for other reasons. The difference by age may arise because infection rates in those under 50 are currently much higher than in those over 50. In truth, it is likely to be a bit of both, but without data specifically on those being treated primarily for Covid it’s difficult to get to the bottom of which is making the biggest difference.
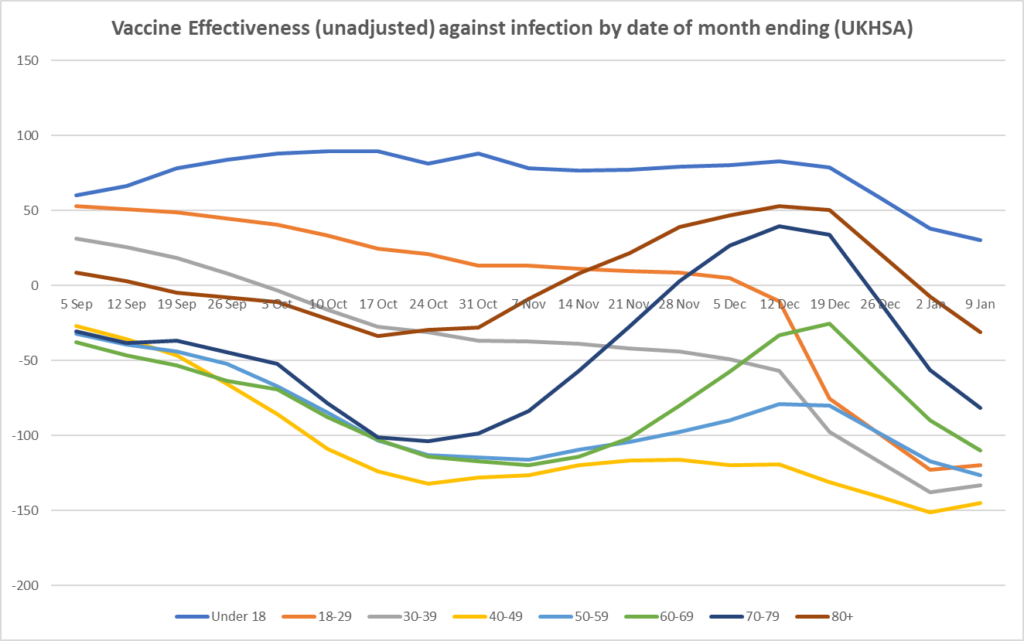
Unadjusted vaccine effectiveness against infection continued to decline in older age groups and in under-18s this week, presumably due to the waning of the third and second doses. It is negative in all over-18s, meaning the infection rate is higher in the vaccinated than the unvaccinated; in the 18-70s it is lower than minus-100%, meaning the vaccinated are more than twice as likely to have an infection. It did however rise slightly in the 18-50s this week, from a very low base. UKHSA continues to claim this extraordinary data is a result of confounders such as different risk factors and testing behaviour between vaccinated and unvaccinated. However, the agency still has not published any data on these confounders (e.g. testing behaviour and co-morbidities by vaccination status), despite being asked repeatedly, nor made any attempt to estimate adjusted vaccine effectiveness based on this data. If you would like to ask it to do this you can email its head Mary Ramsay here (Twitter here).
Unadjusted vaccine effectiveness against death continues to hold up at high levels on this data. This suggests the data is not highly confounded by risk factors, as the UKHSA claims, as then we would see low effectiveness against death too. Note that effectiveness against death did decline until November, suggesting the third doses have helped here.

One curiosity this week is that initially the UKHSA published a mistaken version with missing data. Although it’s not clear which data was missing, Daily Sceptic reader ‘Amanuensis’ (as he’s known in the comments) has analysed it on his Substack page and thinks it may have included data just for two doses with the data for third doses missing. If so, it shows 50% more deaths in the two-dose-only group compared to the unvaccinated, which would be alarming. However, one explanation is that boosters may not be given to those at highest risk of death owing to their health condition, which would concentrate deaths in the two-dose group, artificially both lowering the effectiveness of two doses and raising the effectiveness of three doses. This is all quite speculative, however.
It’s also worth noting here the latest data from Public Health Scotland, which for two-doses-only shows negative unadjusted vaccine effectiveness (i.e., higher rates in the vaccinated than the unvaccinated) not only for reported infections but also hospitalisations and deaths. The data is so remarkable that even Herald Scotland reported on it.
Double-jabbed Scots are now more likely to be admitted to hospital with Covid than the unvaccinated amid an increase in elderly people falling ill due to waning immunity.
It comes amid “weird” data showing that case rates have been lower in unvaccinated individuals than the single, double, or even triple-jabbed since Omicron became the dominant variant in Scotland.
The counterintuitive data from Public Health Scotland (PHS) contradicts previous pandemic trends which have consistently shown infection, hospitalisation and death rates to be highest among the unvaccinated. …
According to the latest PHS report, the Covid death rate has been consistently higher since December 4th in the double-jabbed compared to the unvaccinated – but much lower in the triple-jabbed. …
In the final week of December, the death rate was 7.06 per 100,000 among the double-jabbed compared to 4.79 per 100,000 in the unvaccinated, and 0.21 per 100,000 in the triple-vaccinated.
In the week ending January 7th, the hospitalisation rate was also twice as high in the double-jabbed compared to the unvaccinated – 130 admissions per 100,000 versus 59 per 100,000 – but fell to just 15 per 100,000 in the triple-jabbed.
The admissions data does not differentiate between patients in hospital ‘because of’ Covid and those who tested positive while being treated for other ailments, but PHS said the high hospitalisation rate for double-vaccinated individuals is being driven by increasing admissions among over-70s who are not yet boosted and whose immunity is waning.
It added: “In other age groups the rates remain lower for those with two doses compared to those with one dose or unvaccinated.
“This group of individuals aged 70-plus who have had two doses of vaccine but have not yet had a booster may include some very vulnerable individuals.”
It’s interesting that PHS is pinning it on waning immunity, a stratagem which may be intended to encourage booster take-up. Though they don’t mention it, as noted above, it’s possible that the non-boosted over-70s are a higher risk group and not being boosted for that reason.
Lastly, with all this immune-evasion, there is the question of how similar Omicron really is to other variants, and whether with its reduced virulence and changed clinical profile it ought really to be deemed a new strain rather than a new variant. A recent pre-print found natural immunity down to 56% effective against re-infection, which while no worse than the reported protection from boosters (and more resilient), is still lower than you’d expect for natural immunity. The SIREN study of healthcare workers also saw a leap in reported re-infections.
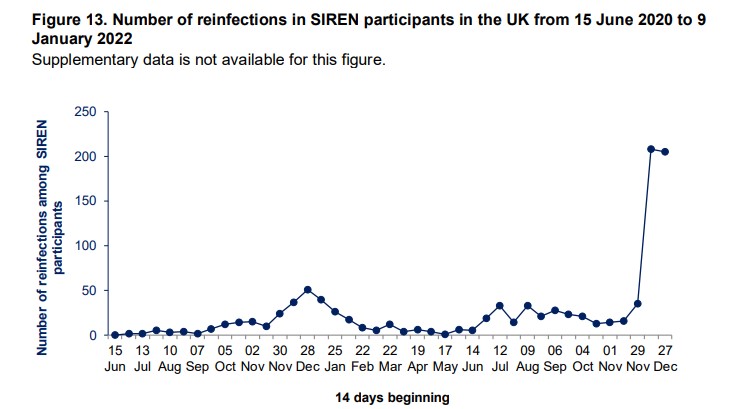
One to think about.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Its high time the people of Wales gave Dripford his marching orders.
In the recent council elections, he was in the north and mid-Wales. Unfortunately, in the urban south, they’d vote in an orang-utan with monkeypox if it wore a red rosette – and there’s much more of them than us mountainfolk.
What the hell do the Welsh urbanites see in him? Doesn’t drink, doesn’t smoke, too wimpy to even watch the match.
You guys need some George North!
His greatest triumphs came around Christmas 2020. First, pubs were forbidden to serve alcohol. Then the Dung waited until they’d all accepted bookings for Christmas meals, and got the food in – and then closed them, so thousands of tons of food had to be thrown away.
Purposeful destruction for the sake of destruction, the evil bastard.
You could stick a red rosette on a burning bag of sh*t and they would vote for it. Being Welsh is to constantly wonder what the hell is wrong with the rest of your countryman.
I got the impression he was getting his own back at society for his son being in jail.
Drakeford is the worst kind of petty tyrant, drunk on power. Google ‘Jonathan Drakeford’ and find out about his admission of a child sexual offence, two counts of rape and one count of assault causing serious bodily harm.
[Mr. Drakeford] warned measures were in reality “on hold” in case of another wave – with two new variants already being monitored by health officials.
Dickford is going to have to have his power-crazed claws prized off the levers of power.
If he gets ousted he’ll only be replaced by another Covidian.
Labour has an endless supply.
Dungford.
Will they be ”cold, dead fingers”?
And of course there’s monkeypox, which now means pets may have to be put down….
https://www.bbc.co.uk/news/health-61608384
Ramping it up, as expected.
What the doomsters have failed to explain is why, if Moneypox is the threat they are trying to portray it as, it’s not spread widely around the world well before now, given that in some areas it’s been endemic for years.
It appears that certain people with certain proclivities are those most likely to get it. Worth adding that until a few days ago the NHS were saying that the majority of cases need no treatment at all.
Although the article admits that no pets in Britain are showing signs of. the pox, and none ever has.
Reality is not something which concerns the doomsters (or the modellers).
Really?
But better safe than sorry!
Just heard on the news that even hamsters have to be put in quarantine for three weeks if someone in the household has monkeypox. Honestly you couldn’t make this shit up
A Hamster cull is the only solution.
Save the National Hamster Service!
Yet the poor little blighters won’t have autoimmune blisters as a side effect of the toxic bioweapon covid injection! Link to p2 of Pfizer’s own list of side effects….
https://t.me/AnnadeBuisseretUKLawyer/1822
It’s important to keep in mind that the Worst Health Organization (aka World Hate Organization) will try a rerun of this within the next 10 years. Especially considering that they’re planning to become responsible for a so-called one hate approach, based on them equally hating humans, animals and the planet.
[The one health approach making them responsible for the holisitic health of humans, animals and the planet in their new pandemic treaty. Anybody even talking about the health of a planet is obviously either a megalomanic crackpot or a devious political schemer.]
I fear that they won’t ‘try’ but it will happen. The ordinary citizen the world over has demonstrated they will swallow whatever our leaders feed them. The majority will undoubtedly do absolutely everything again.
They’ve tried this three times since 2000 and failed twice. Hence, I’m cautiously optimistic.
I’m duckin not optimistic and so far I ain’t wrong.
There’s nothing like a pissed off Brit to put paid to global domination ambitions.
Covid was credible in the first few weeks.
Monkey Pox credibility lasted all of 5 minutes.
Give or take 4 minutes 59 seconds.
Brilliant! (From another sceptic Scot)
Or is Scot just his Christian name?
He spoke of knowing an area of Scotland well anyway.
“within 10 years?”
FFS the target date is 2030. Get a grip.
More like the World Homicide Organisation.
Covvie took a wrinkled little nonentity and turned it into a big bullying bogey. Of course the horrid creature doesn’t want covvie to end.
I think the messianic delusions of the so-called progressive left are genuine, ie, that they really do believe that they’re the universe’s chosen people on a holy mission to save Absolutely Everyhing[tm] from mortal dangers only they themselves are capable of recognizing early enough.
You could be talking about Danfuhrer or Masky Mark there.
Wretched creature.
Wales desperately needs ‘Drakeford level zero’ but he’ll be giving 12 year olds the vote soon to keep his juvenile politics going
If that be so, perhaps 12 year olds don’t want to be locked up with rags over their faces forever? On the other hand, many are Welsh.
Now all Wales needs is the electorate to give Nanny Ap Drakefford the boot.
Welsh numpties would elect a block of wood if it had the Labour label. Come to think of it, that’s exactly what they have done.
Sturgeon is as bad, but at least has a bit of spunk about her (metaphorically).
Drakeford is just a miserable, wet pillow. No self respecting Welshman would vote for a snivelling teetotaller as Welsh minister.
I reckon the polls were as bent as the 2020 US elections.
I really wish you hadn’t said that first sentence, very challenging as it were.
How can anybody with any semblance of a brain invest any credence in anything these people say about ‘The deadly virus’.
It’s surely now abundantly clear, even to NHS worshippers, that none of those in charge gave a flying F*** about it if it interfered with their own drinking, pish ups or disporting themselves with their mistresses.
Here in my part of north-east Wales, as soon as the mask mandates were lifted everybody stopped wearing one, apart from a few sorry wretches and the Chinese.
Likewise, hardly anybody was wearing one in 2020 when the mandates were in force in England, but not in Wales.
It made me wonder whether the reason mandates lasted longer and were harder in Wales is because the Welsh were less likely to voluntarily adopt them – so they had to be forced.
Unfortunately compliance was 95% when the masks were made ‘mandatory’.
What’s it like now elsewhere in the UK?
The number of people wearing one (excluding Chinese) in the Reading pedestrian zone shopping mall has fallen from 15 – 20 (when I started counting them) to solidly below ten. Today was actually first day where I didn’t see anyone with a mask while passing through once.
I like to entertain the thought of waiting until there’s routinely only one mask wearer and then throw him into the canal so that he’s gone as well.
Just give them a card with the telephone number for.a mental health helpline.]
Anyone wearing a mask, especially outdoors, has serious mental health issues.
I’d rather hit them with a standard-sized supermarket sunday roast. Preferably unpacked.
NB: That’s about 53 ounces of raw beef which is going to pack a punch. Minus blood smears, it’s not going to leave visible traces, though.
Frozen.
Any traces can be blamed on monkeypox.
The very idea behind this is to hit someone with something sufficiently soft that all the force of the impact is transferred and of enough mass that there will be an impact. When it’s as hard the skull, it’ll either break it (not desired) or skull and blunt instrument will bounce off each other.
The ‘classic’ weapon for this would be an old-style A4 sized phone book but these have fallen into disuse.
Still a lot in branches of Waitrose, for some reason
Here in the North-East it is mainly old people wearing them still, I think they have been terrorised basically. The other group is young Chinks at the uni in Durham, I would say 90% if not more are nappied up. Some people say this is part of their culture but I definitely did not see a single example of a person in Durham wearing a face mask prior to March 2020 and there were just as many Chinese students then
I went to the supermarket yesterday here in Wales. I am in a Welsh nationalist area of Snowdonia. Only one couple were wearing masks, so clearly except for a couple of retards people have wised up. Nevertheless Drakeford and Labour will be re-elected to the Senedd in exactly the same way that Sturgeon and the SNP have a monopoly on power in Scotland. This is not healthy for politics – these Poundland Parliaments need to be abolished.
Agreed. It would get rid of a lot of poxy monkeys.
This is Blairs idea of a joke.
Yep, that about sums it up.
Blair was extremely sceptical about devolution.
He implemented it because it was longstanding Labour party policy and because he believed he’d be unpopular without it.
My experience too in nationalist Snowdonia. A different story on the North coast tourist trail.
Surely there’s only so long the likes of the BBC can continue to report the death of young healthy people with a eulogy and no explanation for how the person died.
Yes.
Mark Crispin Miller’s website describes many of these unexplained deaths in much detail, complete with links to the local news reports…..
It appears that perhaps Mr Drakeford isn’t fully appraised regarding the available Covid data and consequently lacks a fully evidence-based appreciation of the issues.
I should translate from Physician-speak. What it actually means is ‘What a thick as pig sh*t f**g witless arsewipe’.
Did you say “What a thick as pig shit fucking witless arsewipe”?
My hearings a bit dodgy these days.
Your restraint does you credit.
the way these people carry on is if we are all now dead and this so called virus was the worst ever in history, last time I checked the population numbers have not shrank by millions and millions.
I read somewhere that birth rates in the UK haven’t been affected at all by covid, and the average life expectancy has risen.
Thousands more illegal immigrants may have influenced that, other than the national census came and went some time ago.
Two politicians that haunt the public psyche:
Thatcher – hated by the left for improving the country.
Blair – hated by the left for not completely destroying the country.
One politician memorable for nothing – Mark Drakepenis, First Minister of, that part of England which hasn’t the dignity of at one time actually being independent from England.
I love my Welsh Celtic cousins but, really guys?
And now Johnson, hated equally by the left and the right for destroying the country.
This Drakeford will inevitably, and sooner than we think, be charged with criminal conspiracy in regard to his commission of egregious Crimes Against Humanity. If found guilty, sentencing will be proportionate and in accordance with Nuremberg precedent.
ZZZZzzzzzz…. this sort of thing is said all the time by people who are too afraid to go round and ring Drakeford’s doorbell.
Do you really believe what you’ve written?
When found guilty he can join his rapist son in chokey!!
As with Westminster,Wales is governed by scientifically Ignorant arts graduates who are scared to question Public Heath, a reservoir of medical school failures who suddenly have been given a spotlight from their years of irrelevance. It is time for the harm caused by lockdowns,adverse reactions and mental harm to the young be litigated. Drakeford remains a menace – he was elected because we are a one party state.
The sad thing there are hundreds of MPs in England who are just as cuckoo as this man
An interesting read. https://expose-news.com/2022/05/28/19million-unvaccinated-31milllion-vaccine-refuseniks-england/
Drakeford is clearly mentally ill and needs sectioning.
He’s already sectioned, in the mental asylum called ‘Wales’.
Tell me something. Despite the extra and far longer restrictions operating in Scotland and Wales, have their Covid health outcomes been materially any different to England?
They’ve been worse
Daffy Duckford.
Do people actually VOTE for these drips?
These people need to be careful no one actually assassinates them. This is ridiculous abuse of power. This is the guy they caught lying and saying oh shit did they here that on his supposedly unmiked conversation about rolling the people that it wasn’t actually illegal to go out.
Who cares what a Marxist, who evidently gets dressed in the dark, says?
So any future jabbing will be confined to the ‘vulnerable’ – there won’t be many of those left in a couple of years time then. Mengele would be envious of this plan.