We’re publishing another guest post by our in-house doctor, formerly a senior NHS panjandrum, this one looking at the latest hospital data. Turns out, staff absences are the reason London hospitals are under pressure, not a surge in Covid admissions due to the Omicron variant.
How quickly things change. The Daily Sceptic has asked me to provide a brief update on the unfolding situation after the Christmas weekend. Less than two weeks ago at the Downing Street press conference, Professor Chris Whitty said “by the time we get to Christmas I expect the majority of people going to hospital to be Omicron cases”. In response to a journalist’s question about Omicron, he said: “This is a really serious threat. How big we don’t know but everything we do know is bad.”
So, how bad is it?
Hospital admissions are rising, but not necessarily due to Omicron, according to Chris Hopson, the CEO of NHS providers.
Talking to chief executives this morning, the sense is that admissions are rising but not precipitately so. What’s particularly interesting is how many chief executives are talking about the number of asymptomatic patients being admitted to hospital for other reasons and then testing positive for Covid.
Trusts are not, at the moment, reporting large numbers of patients with Covid type respiratory problems needing critical care or massively increased use of oxygen, both of which we saw in January’s Delta variant peak.
Hopson is in error on one point – the peak in January was the Alpha variant. But then attention to detail is optional for NHS executives. On the other points around the reduced number of admissions and the rising proportion of incidental Covid cases, the published data support his remarks.
In this brief update on the unfolding ‘nailed on’ Omicron catastrophe, I will present a few graphics illustrating what the public are permitted to know so far.
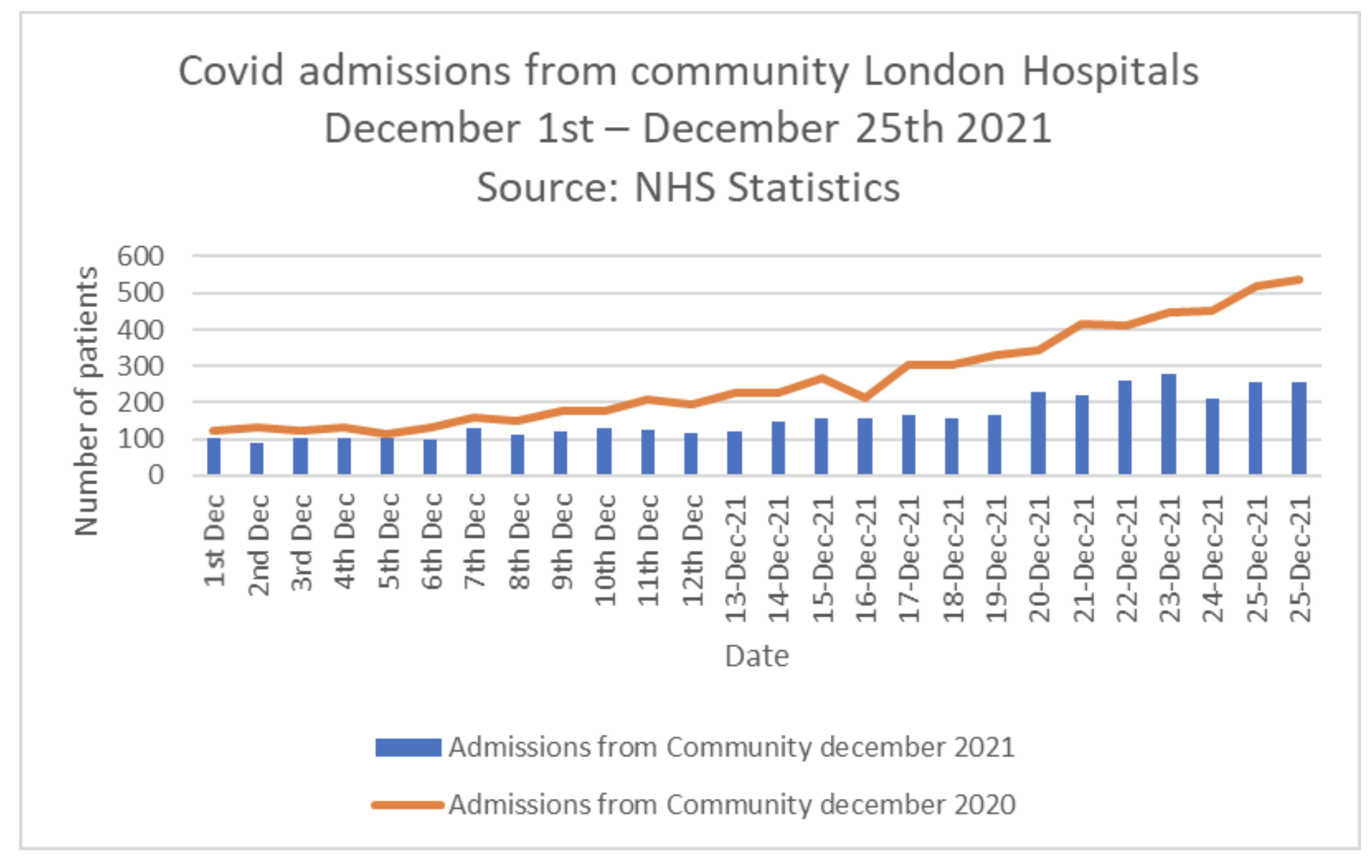
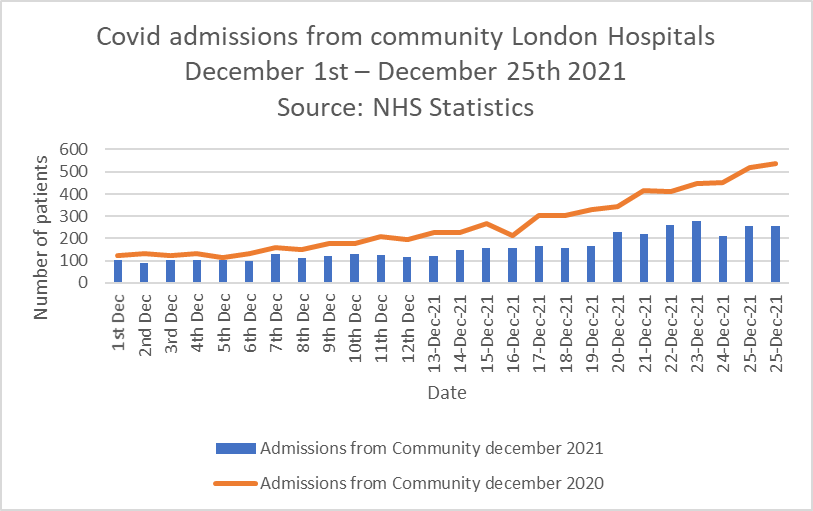
First, the figures for the Christmas weekend. Graph One shows the admissions from the community with Covid in London hospitals in December of this year and last. It compares figures from December 2020 (the brown line) with admissions for December 2021 (the blue bars). If the confident predictions about imminent catastrophe from SAGE are to come to pass, the Omicron variant really needs to up its game. So far, it is failing to deliver. The current admission rate is less than half that associated with the Alpha variant at this time last year.
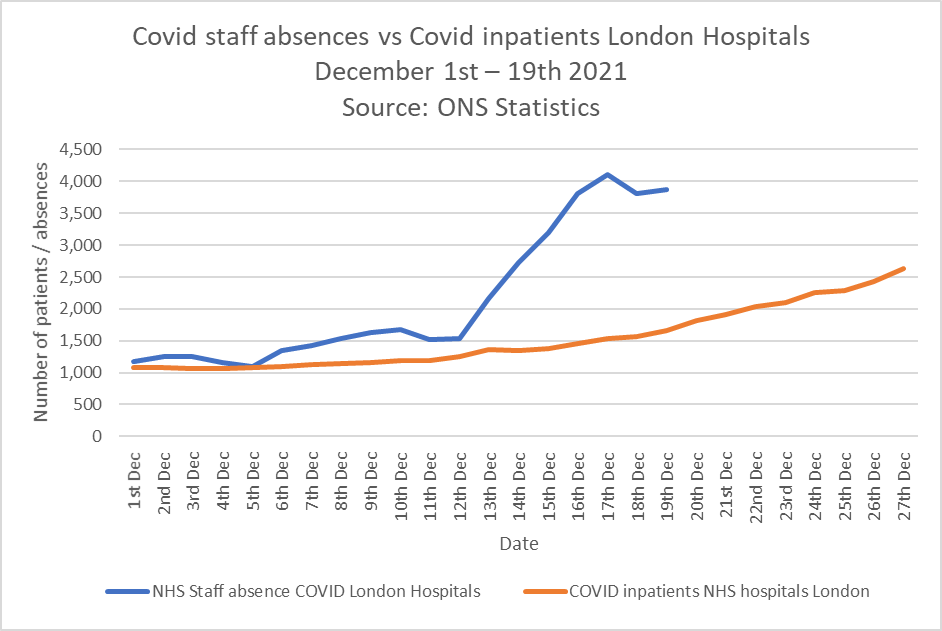
Graph Two shows the real problem in London. The blue line represents staff absences from London hospitals up to December 19th. This is the most up-to-date data we have. The NHS collects information about absenteeism on a daily basis, but will not be providing the next public update until January 13th. The brown line represents patients testing positive for Covid in London Hospitals (bear in mind, as Hopson points out, the brown line is a gross overestimate due to incidentally positive cases).
It can clearly be seen that there are far more staff off work ‘due to Covid’ than there are patients in hospital ‘with Covid’. How many have tested positive but are asymptomatic? How many have the sort of mild symptoms we’d usually associate with a cold, which in normal years would not require absence from work, nor any tests to confirm the presence of a seasonal upper respiratory tract infection? My central point is that the current pressure in London may be because we’re sending staff home for extended periods when they’re not unwell, rather than an influx of severely ill patients. Simply put, is it possible that an over reaction to a perceived threat is causing the problem rather than the Omicron variant per se.
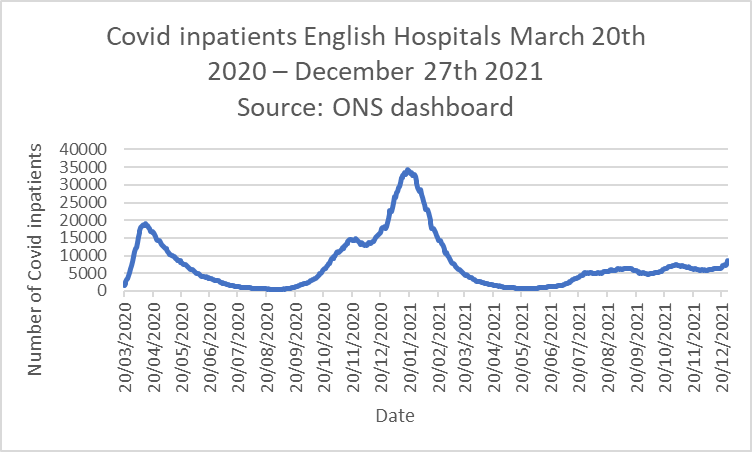
Graph Three provides further context in relation to the overall inpatient burden in English Hospitals across the whole pandemic episode. Even taking the figures at face value and discounting the known over estimations in relation to primary diagnosis, it is clear that the 8,474 patients currently in hospital with positive Covid tests is substantially lower than the 19,783 in hospital on the same day last year – this equates to a Pritchard ratio of 0.42.
All other observable metrics such as ICU occupancy, data from the ZOE app and, of course, the now negligible death rate from Covid points to a much better situation than at this time last year. Hospital admission rates expressed as a percentage of positive tests in the community continue to fall from a peak of 9.6% in February to 2.1% now. Patients testing positive for Covid occupy 6% of NHS beds, compared to 22% this time last year. The widely predicted re-emergence of winter flu has also failed to materialise – cases of flu are still 95% below the numbers seen in 2019-20.
Despite this stable looking picture across the piece, multiple expert commentators have yet again been quoted in the mainstream media forecasting imminent catastrophe and demanding complete societal lockdown. There have been some reasonable points made around the possibility that the data over the Christmas weekend may be subject to a reporting lag, and justifiable concerns about the possibility that intergenerational mixing over Christmas could lead to more cases occurring in vulnerable older people. The SAGE meeting notes from December 23rd make reference to these possibilities. However, the general tone and content of public remarks is at variance with the available public information.
For example, Professor Danny Altmann, an immunologist based at Imperial College London, told MailOnline that Boris’s decision not to impose any further restrictions seems to show the “greatest divergence between expert clinical/scientific advice and legislation”. I fail to understand this view. His remarks are congruent with the letter published in the Lancet earlier this year by 122 self-identified experts accusing the Government of conducting a “dangerous and unethical experiment” by lifting restrictions on July 19th, which of course turned out to be nothing of the sort.
Professor Altman knows far more about immunology than I do. It would be enlightening if he could explain to the Daily Sceptic why experts like himself are so constantly antagonistic towards the Government, given that over 85% of the U.K. population have now been vaccinated against Covid – rising to 95% among the over-60s – on top of substantial natural immunity generated by infections over the last 12 months.
Other self-identified experts from Independent SAGE are promoting a subtle rebrand of societal restrictions by referring to legalised social limitations as ‘health protections’. To my mind this is an overt politicisation of science – readers should be very concerned by such Orwellian language.
When I hear expert advice that does not correlate with observational experience I lean on the motto of the Royal Society – Nullius in verba, roughly translated as ‘take no man’s word for it’. To that end and to enable non-experts like myself to assess the data for ourselves, it would be helpful if the NHS could release daily updates on Covid discharges from hospital and details about the length of stay of Covid patients. This information is available and provided to all NHS chief executives in daily email briefings, so why are taxpayers not permitted to see it? If scientists and public health doctors are pressurising the Government to restrict citizens’ right to make their own choices around freedom of movement and association, isn’t there an onus on the NHS to provide all relevant information relating to that advice?
Further data packets should be released on Thursday. I will update readers later in the week.













To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
If I make a sandwich board, like the chap who used to walk up and down Oxford Street, and wander about shouting “The end is nigh”, will I be as qualified as Whitty apparently is, for a knighthood? He’s the Bodkin Adams of our times, but perhaps not as good-looking.
A PhD qualification is supposed to train the participant in critical thinking. Not sure what happened with this shower of shit
Carrots and sticks.
If Chris Whitty ever had any original thoughts, that was probably long before he finished his first bachelor’s degree. There’s no way he’d have had the guts to have any while he was doing his DSc.
Was his dad in MI6? His father was a British Council officer who was posted to various countries including Nigeria and Malawi. He was cultural attaché in Greece when he was knocked off by the Fatah Revolutionary Council apparently. I wonder what they had against him.
His mum’s brother Christopher MacRae looks like a strong MI6 possible too. Another Africa hand.
It was in Africa that Chris Whitty got a big grant from the Bill and Melinda Gates Foundation.
The January-peak this year was caused by the alpha- or Kent-variant. Like its successor omicron, the delta (Indian) variant was a statistics-only event causing a huge peak in positive test results of healthy pupils before the summer holidays.
The masters of COVID testing have presumably gotten their act together somewhat better now, hence, a huge, spontaneous decline of positive test results because pupils were pulled out of the machinery hasn’t happened since.
COVID has been running on bullshit and waiting for a deus ex machine to come to the rescue since the Kent-peak went away in January. Certainly entirely coincidentally, mass testing of healthy people for want of sick ones started soon afterwards.
I love a “deus ex machina”, but prefer a Chekhov’s Gun.
They’re something different: Deus ex machina is a plot device where an otherwise insoluble problem is resolved by the unexpected (by the audience) appearance of a saviour. Sort-of, solution — a miracle happens. In the COVID case, this would be the virus (presumably intentionally) misnamed Sars-CoV2 suddenly living up the the reputation of its name and turning into the SARS virus. Hopes for that (in the form of it could happen, couldn’t it?) have already been expressed by the experts months ago.
Please can you explain what you mean when you say that SARSCoV2 was misnamed and also that it turned into SARS, meaningly presumably into what is now called SARSCoV1.
We can be absolutely certain that there has been at least 19 years of research into the biowar use of SARS variants. None of it is public.
Christian Drosten, they guy who invented the COVID PCR test and is thus responsible for much of this entirely avoidable misery is a SARS specialist. He’s on record for stating SARS is back! – presumably with a sigh of relief – when the current awful virus started to make waves.
I think it was intentionally named Sars-CoV2 to conjure up a connection with its distant and much more lethal relative.
Yes indeed! Drosten faked his qualifications – he is a fraud – nothing he says can be believed – he follows the WEF Globalist Reset Agenda not science..
Is it not more accurate to say that Drosten devised the mass testing regime by adapting swab derived RNA to DNA by conversion, then appending cycle threshold amplification to the Kary Mullis PCR testing technology, with software which “determines”, ultimately, what is a “positive” test?…I am not a scientist..evident to some.
How did you escape the gorilla suit? Wondered since I watched the film a few years ago.
Isn’t life at least partially about quality not quantity? I certainly don’t want to live until 90+ in Covid world.
It’s been one of the more obvious points from Day 1 that life (as in breathing) at all costs cannot be the overriding consideration. People seem to have forgotten what it means to be alive. Perhaps they never knew.
Qualified disagreement: Corona politics are about prohibiting other people to do stuff the Corona politicians wouldn’t want to do, anyway, because they believe it’ll prolong their lives.
Nice, recent example: There’s currently an 8pm hospitality curfew in Ireland. The people behind this were originally pushing for a 5pm one. This was shot down because it would stop 9 – 5 office workers from having a few after work. People working other hours obviously matter a lot less.
Well, I guess I was thinking more about how ordinary people have been hoodwinked into being deprived of a quality life. Of course I agree that Corona politicians don’t care about anyone or anything but themselves and their own power.
Little chance of that now!
85% of the UK “vaccinated”?
You’re ‘avin a giraffe.
Just got back from the IMAX at the Science Museum to watch some educational film with my kids
Before it started there was an advert with Whitty bleating on about Omicron and boosters.
Other than the nauseating sight of the ugliest man on the planet looming at you on a screen 4 times higher than a double decker bus what was great was the whole cinema booing.
Gives you a bit of hope.
Honestly, most of the trailers at the cinema deserve to be booed thoroughly now. When they aren’t showing that ghoul’s horrific mug they almost entirely constitute climate change lies and corporate virtue signalling. Good to hear about the booing actually occuring. All of the film’s I have been to see recently had empty auditoriums so there was no point booing. I’m looking forward to triggering some booing when I go to see the Matrix film.
Horror film ?
“what was great was the whole cinema booing”
That’s beautiful! You have made my day!!
Ever since this Covid farce started NHS workers (and many others) have been told to self isolate when it was totally unnecessary.
Just because you test positive doesn’t mean you are infectious.
The whole testing regime needs to be scrapped.
But as it won’t the least the government can do is reduce the testing and be much more nuanced for those that are tested.
No symptoms, carry on working.
Slight sniffle carry on working with a proper mask.
Feeling unwell take a short time off work until you feel better.
Common sense was never this governments strong point.
Slight sniffle carry on working with a proper mask.
Chinese mummery is not effective against respiratory diseases and even it it was, this would be no reason to mandate it. Respiratory diseases are usually harmless for everyone. Possible complications have to be dealt with by the health system, that’s why it exists. People who are afraid of them nevertheless are free to take whatever precautions they deem sensible.
That’s how our society has worked since ever and people who absolutely don’t want to cope with that are hereby impolitely requested to move to or stay in the country of their dreams, namely, China. Force-exporting Chinese cultural backwardness to the rest of the word is not a public health innovation.
I was talking about NHS staff wearing a proper medical N95 mask or equivalent to protect vulnerable patients.
You’re talking about Chinese mummery to protect against respiratory diseases. No amount of just in case COVID-BS is acceptable. If it wasn’t already being done prior to 2020, say, something I know for certain, care home staff being forced to wear FFP2 respirators just in case to protect vulnerable care home residents (whose quality of life is certainly much improved by having to deal with faceless aliens all the time), it’s not needed now.
Every millimeter given way in this direction is a slippery slope towards mask mandates and other restrictions for general public health reasons.
A nurse on critical care with a sniffle wearing a proper medical face mask whilst treating a vulnerable patient is preferable to that highly qualified and valuable nurse taking time off work just because she has a positive test or similar symptoms to a common cold and is well enough to work.
This is a much more limited statement than the Slight sniffle carry on working with a proper mask you originally made. However, I’m not going to address to modified version specially. All already said.
I was clearly referring to “NHS workers” in my original post that’s why I put (and many others) in brackets.
I keep my posts concise for brevity.
Perhaps you should read posts more carefully before you jump in with your knee-jerk reply.
Assuming you are trying to maintain that you’re something other than a guy not so covertly arguing in favour of Corona policies, you should stop climbing the ladder you’re presently on, namely, start with a general statement. When being called out on that, twist that into a much more specific statement. When being called out on that, claim that you didn’t make the general statement and start to become abusive.
You’re not gaining any ground here, just accidentally peeling off your own protective camouflage.
Have you always been an arrogant twat?
He’s spent a long time as also an arsehole.
From what exactly?
I don’t understand your question.
All the billions they spent on one thing and another and they can’t tell if the person is infectious. That should have been a priority imho.
The Drosten PCR test has been a fraud from the start- it cannot identify an infected person – with Covid or anything else.
They wanted to wreck the crumbling NHS and have done an excellent job – they have made a bogus excuse to sack half the staff- would never have got that past the Unions!
I see some Doctors’ surgeries are ‘closed’ again today another case of “Note for Surgery door ‘Please stay away if you feel unwell”?
Should the “Untreated” form a Twitter pressure group?
They still shouldn’t have got it past the unions! NHS staff are joining Workers of Britain.
The Nudge Unit and the Propaganda have worked well
Still ar it – expect another onslaught soon.
Wow this guys quick. Bovid has had a 99.97 percent survival rate in the under 70s from natural immunity from day one. This whole rotten episode is nothing but an over reaction to an engineered deliberate raping of public perception. Its a scam and always has been. Even if the NHS is overwhelmed, its not a valid reason to destroy our lives.
I think they call flu “covid” now, hence the drop. They need the numbers to terrorise well meaning people with so they have to use whatever is available to achieve this. Youre dealing with deceivers and criminals, so to not suspect trickery and fiddling of the details to achieve the desired outcome is naive in the extreme. Hasnt it been established that these bent unvalidated tests cross react with influenza.
That’s right, that age-old principle of health care, treat the symptoms, if there isn’t sufficient capacity, increase it! That’s all that was required.
The problem was politicians & technocrats got involved instead of letting Dr.s & nurses do their jobs.
We used to have “Fever Hospitals” for emergencies and isolation -scrapped in the 1980s-90s
Has there been a SINGLE confirmed omicron death yet?
If anyone’s got a source for one, can they post it please. And since “science” is fashionable at the moment, I’ll add that if you want to say omicron caused something, you have to rule out that delta or “original” was present. (Obviously you also have to rule out a lot of other stuff, but I’ll leave that aside.) What I’m asking for is a reliable reference to a SINGLE DEATH “with omicron”, where the person has tested NEGATIVE for delta and “original”.
Listen. OMICRON DOESN’T CAUSE COVID. Omicron only affects the upper respiratory tract, especially if a person is already chronically ill. I doubt it even touches your lungs. Pneumonia is a lung disease. Pneumonia has to be present for a diagnosis of “Covid”. No, a person hasn’t “got Covid” if they feel a bit under the weather or they’ve got a runny nose. If they think that means they’ve got Covid, they’re a hypochondriac arsehole.
All upper respiratory tract infections, even the common cold, have pneumonia as possible serious complication.
We need an age limit on this question. Over a certain age, I think it’s safe to say any infection could have bumped them off, including a common cold. And of course it’s worth remembering people die from complications of contracting SARS-CoV-2 not of it.
From what I can work out (happy to be corrected) nobody dies from the initial respiratory problems caused by early covid symptoms. Secondary disease becomes more of a vascular issue migrating to other organs and or severe disease is caused by your bodies autoimmune response.
Either way, there’s good evidence to show this can be easily treated with cheap effective, safe pre-existing drugs. People die for two reasons, old age/comorbidity or health care negligence. The latter likely the greater cause of death.
The Great Ivermectin scandal needs more attention
Why would a Health Department concerned with saving lives ban a safe effective and cheap treament for early Covid – and instead smear it with talk of ‘horse dewormers’ fed to the media by the 77?
People died who could have been easily saved. Johnson, Hancock and Javid are all involved in banning this effective treatment to push the vax.
See this ONS data. Comorbidity is the biggest determinant of death with Covid.
Whitty
We don’t know
We don’t know
We don’t know
But we do know it’s going to be bad
The very definition of hysteria
But surely the right question to ask is, was covid ever a serious threat? No i’m not claiming it never existed or even that for the exceptional minority that contracted severe disease & died it wasn’t serious.
We all know there was a complex web of deceit, obfuscation, statistical manipulation & absolute dishonesty during the first “wave”. We also know many who died in April 2020 died from maladministration.
Never let go of the facts from the start this was a psychological operation to sell a pandemic threat to the masses, it was state sponsored terrorism. Never let go of the fact due to criminal conspiracy between politicians & big pharma orchestrated by Gavi & WHO, cheap safe effective medicine could have & should have saved many lives, instead the use of treatments were suppressed by politicians & technocrats in favour of big pharma shareholders.
Never forget the millions, perhaps billions of lives ruined by neoliberal globalist propaganda & NGO censorship!
Next question. How do you isolate a DNA sequence for a virus you have never purified?
Help me understand what you mean by this. “How do you isolate a DNA sequence for a virus you have never purified”?
I’m new to this site and it’s refreshing being able to see comments from people not following the same narrative that’s been vomited out the past two years. However, I am aware of my ignorance so I’m trying to make myself as well-versed about this stuff as possible as I currently know very little.
Read this and see the web of deceit being woven at full velocity, by all levels of the system, from Government to care home worker.
https://dailyexpose.uk/2021/08/29/midazolam-was-used-to-prematurely-end-the-lives-of-thousands-who-you-were-told-had-died-of-covid-19/
“given that over 85% of the U.K. population have now been vaccinated against Covid – rising to 95% among the over-60s – on top of substantial natural immunity generated by infections over the last 12 months.”
If so, why does the latest UKHSA COVID-19 vaccine surveillance report for Week 51 state:
“Vaccine coverage tells us about the proportion of the population that have received 1, 2 and 3 doses of COVID-19 vaccines. By 19 December 2021, the overall vaccine uptake in England for dose 1 was 68.2% and for dose 2 was 62.6%. Overall vaccine uptake in England in people with at least 3 doses was 38.9%. In line with the programme rollout, coverage is highest in the oldest age groups”
“at least 3 doses”
I hadn’t realised some people were already on their 4th, or eve3n fifth, doses.
Some people, perhaps, but not on any large, systematic scale yet, I don’t think. Even Israel – “vaccine”-central – is only just warming up for it:
“An Israeli hospital on Monday began a study to test the safety and effectiveness of a fourth dose of a Covid-19 vaccine, as health officials continued to deliberate over rolling out fourth shots for vulnerable people nationwide.”
Israel begins studying the effectiveness of a 4th vaccine dose.
The orthodox way to handle the phenomenon that the present crop of Sars-CoV2 vaccines neither do what they were never meant to do (prevent transmission) nor what no vaccine can ever accomplish (prevent infections) is inject everyone once more.
This a pretty transparent Pfizer (mostly) revenue boosting scheme (they could develop updated vaccines easily, or so they keep claiming, but why do that when the original product is still selling well?) married with the Corona politics staple The pandemic isn’t over. We need to vaccinate more people! which has been employed since 15 million shots to freedom! were accomplished but they weren’t willing to allow the freedom bit to happen.
From personal experience Omicron is definitely not a serious threat.
My whole family have had it over Xmas.
Worst affected is mid 50s overweight and heart issues, unvaxxed. He’s been rough for 5 days. Headache sore throat, flu like symptoms.
Least affected is 21 unvaxxed and healthy. Sore throat and headache for 48 hours.
The only vaxxed person is 73 and had similar to the 21 year old but added tiredness.
“Everything we do know is bad” (Sir Witless).
Was there any sort of a rationale at all for this claim, or did he just flat out lie?
“Why are taxpayers not permitted to see it”?
Because nationalised services treat the customer with contempt.
And if they saw all the data then the lies would become even more apparent and that would never fo
Put them on SSP …. this will end
Whitty obviously got his Knighthood for saying it was and pleasing his ‘Master”.
Is it time for some fresh faces on the sage gang. It sure seems like it.
To that end and to enable non-experts like myself to assess the data for ourselves, it would be helpful if the NHS could release daily updates on Covid discharges from hospital and details about the length of stay of Covid patients. This information is available and provided to all NHS chief executives in daily email briefings, so why are taxpayers not permitted to see it?
Hear bloody Hear!!! How refreshing to read this! I have been gnashing my teeth over this gap in data for a long time. Admissions data without discharge data giving length of stay data, is meaningless and being used as part of the “scare the shit out of them” agenda.
“…it would be helpful if the NHS could release daily updates on Covid discharges from hospital and details about the length of stay of Covid patients. This information is available and provided to all NHS chief executives in daily email briefings, so why are taxpayers not permitted to see it? If scientists and public health doctors are pressurising the Government to restrict citizens’ right to make their own choices around freedom of movement and association, isn’t there an onus on the NHS to provide all relevant information relating to that advice?”
Indeed it would be helpful. There are huge gaps in what we are allowed to know, ranging from lengths of stay through “with” or “from” to the real positivity of tests. I am still waiting for the answer to my FoI request on lab Ct thresholds for the PCR test – which I made just over a year ago. The failure of “The Science” and/or the Department of Health to engage with informed questioners is appalling.
It would be interesting to have the numbers of staff off due to or with/from covid who have been jabbed, compared to those resistant to the jab, sorry, unjabbed.
Chris Hopson used to be on the board of HMRC when I had the misfortune to be an employee. He is a prime example of one of Mark Higgie’s ‘shonky retreads’.