
The following is a guest post from our in-house doctor, previously a senior NHS medic. In addition to looking at the latest Omicron data from the U.K. and South Africa, he touches upon the politicised and corrupted nature of SAGE and attempts to uncover why its models are so routinely incorrect and hysterical.
“Men, it has been well said, think in herds; it will be seen that they go mad in herds, while they only recover their senses slowly and one by one.” So wrote Charles MacKay in Extraordinary popular delusions and the Madness of Crowds (1841). MacKay’s classic analysis will require substantial revision if the Covid delusion ever subsides.
I’m coming to the view that my role as medical analyst for the Daily Sceptic is no longer relevant, because there is such a discordance between publicly available data and decision making that factors other than medicine must be at play. We have moved out of the realm of scientific rationality and squarely into the sphere of medical politics, a game at which I am atrociously inept and not qualified to comment on.
Here is an excerpt from a post I wrote exactly one year ago: “The NERVTAG meeting notes of December 18th which seem to have sparked off the latest panic are relatively muted about its significance, but do record ‘It was noted that VUI-202012/01 (later referred to as the Alpha variant) has demonstrated exponential growth during a period when national lockdown measures were in place.'”
This brings me back to my key point: ‘the illusion of control’. In the spring the rationale for lockdown was to ‘flatten the sombrero’ – a temporary measure to delay viral transmission and prevent the NHS from being overwhelmed by a sudden surge in cases. Since the autumn, that message has mutated to a new variant – the Government and their associated advisors have become obsessed with the need to ‘control the virus’ – yet the evidence shows that they have about as much chance of controlling the weather. So many of the ‘experts’ have invested their entire professional credibility on the premise that more stringent lockdowns are the only way to ‘beat the virus’ and to achieve ‘zero covid’. Yet both of these goals are manifestly unattainable.
Yet here we are again – on the verge of legally enforced societal restrictions which will have the predictable effects of damaging the economy and other areas of healthcare while having minimal effect on viral spread. Readers will remember that lockdown enforcements in January of 2021 were not lifted until mid July – and even then there was substantial opposition to removal of social curbs with hysterical predictions of imminent calamity, all of which failed to materialise.
Another point I have noted over the last year is measurement shift. At first, the reportage was on daily deaths. When these subsided, the quoted figures changed to hospitalisation rates. When those fell off, the focus shifted to ‘cases’ – positive community tests irrespective of whether these caused illness or not.
To quote one of the TV Dragons: “Turnover is vanity, profit is sanity”. In other words, positive tests in the community are irrelevant unless they cause sufficiently severe disease to put patients in hospital for extended periods. Further, as has already been recently exposed in these pages, the more testing is done, the greater the number of positive findings. It is instructive that the percentage of positive tests in the community has not changed over several months – so by increasing testing we are uncovering greater viral spread but this may well be irrelevant to the overall burden of disease.
Although I have substantial reservations about the accuracy of officially released figures, I will go through what we are permitted to see on the only metrics which are currently relevant: hospitalisations. I’m going to firstly look at the situation in London as the capital is regarded as the epicentre of the Omicron outbreak. Mayor Sadiq Khan has declared a ‘major incident’ because 4,900 London healthcare workers are off sick with Covid. It is unclear what proportion are actually sick and what percentage are completely asymptomatic but have been ordered to self-isolate due to contact tracing after staff Christmas parties.
I firstly present the data from the ‘primary diagnosis’ spreadsheet in graph one. Readers may recall this distinguishes between patients in hospital because of severe Covid (blue line) versus those in hospital for other reasons with co-incidentally positive tests (orange line). This data had to be forced out of the Department of Health by Mark Harper MP when he challenged the newly appointed Sajid Javid on the point in the summer. Up to that point the NHS had denied that there was any distinction between ‘with Covid’ and ‘because of Covid’. But for Harper’s intervention, we would probably not be aware of the distinction.
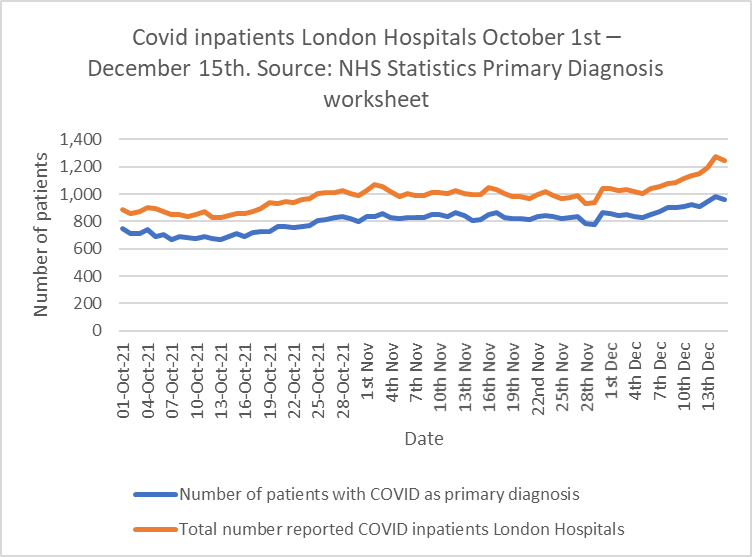
The ratio of genuine Covid patients to incidental Covid patients in London has reduced from 0.84 on October 1st to 0.77 on December 15th. My interpretation of this graph is that the modest rise in Covid inpatients to December 15th is more due to incidental tests than genuine Covid illness. This is important information but sadly only released on a weekly basis.
To put this rise in admissions into context, we can examine graph two. This shows daily admissions in London since the start of the pandemic.
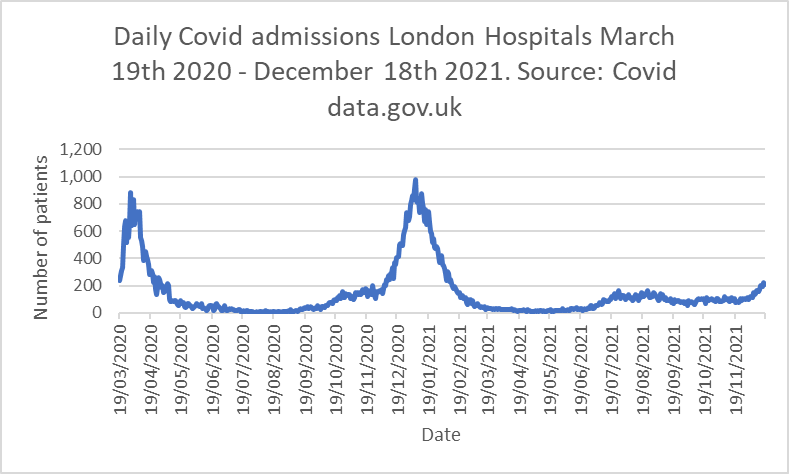
SAGE hypothesise that due to the lag effect between infection and hospitalisation, the blue line on the right hand side (currently 210 admissions per day in London) will shortly exceed the second wave peak of 977 admissions.
SAGE minutes from the 99th meeting on December 16th predict a peak of 3,000 hospital admissions per day in England as a whole by the end of December. As things stand at the moment, across England as a whole, daily admissions have been flat or falling for two months. They have increased recently in London but have fallen off in other parts of the country.
Is this really a plausible analysis given the huge difference in vaccination rates between December 2020 and December 2021? I note that the December 19th Omicron daily overview from the U.K. Health Security Agency gives a figure of 104 hospitalisations in the entire U.K. due to Omicron as of 17th December, although SAGE think that this is about 10% of the real figure due to reporting lags.
It is observable that London has a higher percentage of unvaccinated people than the rest of the U.K. – official estimates suggest that up to 30% of Londoners are not vaccinated.
Lack of vaccination is particularly high in specific ethnic groupings which form a larger proportion of London’s population than in the wider country. Could this be a possible reason why cases are rising more rapidly in London than the rest of the kingdom? Given this disparity, is it reasonable to assume data from London is applicable to the whole of the U.K.?
Fortunately, we do have some real world data from South Africa, which in Omicron terms is about a month ahead of the U.K.
The insurer Discovery Health examined 211,000 positive Covid tests and followed up their clinical course between November 15th and December 7th. Of these tests, 78,000 were from the Omicron variant, the remainder being Delta. About 41% of the tested patients had had two doses of the Pfizer vaccine.
After adjusting for vaccination status, the risk of hospital admission for newly diagnosed adults is 29% lower than in the first wave, said Shirley Collie, a statistician at Discovery Health, presenting the findings. “Furthermore,” she said, “adults admitted to hospital currently have a lower propensity to be admitted to high care and intensive care units, relative to prior waves”.
More recent data published by the South African institute for communicable diseases suggests that the Omicron peak has already passed in Gauteng, and there has been no surge in deaths.
Naturally there are differences between the South African and British population. Their median population age is 27.6 years-old. Ours is 40.5 years-old. They have a lower vaccination rate (26.3% double vaccinated versus close to 90% in the U.K. and over 40% of our population have had booster doses). So, this study does not directly read across into what will happen in the U.K. Nevertheless, it is an important piece of information and I’m puzzled as to why SAGE apparently have not referred to this in their recent meetings, nor have they referred to recent data from Denmark suggesting that hospital admissions from Omicron are about 60% of those from Delta.
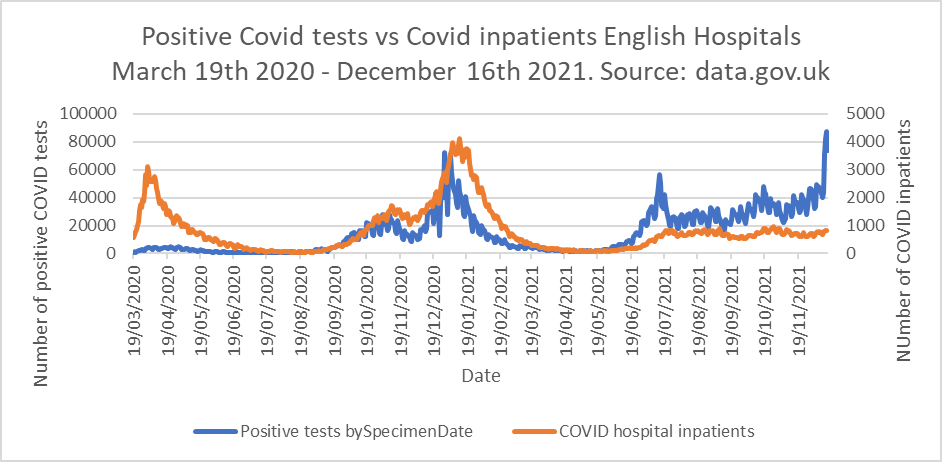
Another anomaly caught my eye this week in graph three. This maps positive community tests (blue) against Covid inpatients in England (orange) since the beginning of the pandemic. Note there are two separate ‘y’ axes – test numbers on the left of the graph and hospital inpatients on the right.
On the left hand side of the graph we can see in March 2020, there was virtually no testing going on but plenty of admissions in the first wave. By the end of 2020 testing was happening but still not highly developed, so inpatients were front running testing until the end of December 2020 (Zoe app data was much more predictive).
The interesting point is in July 2021. There is a clear peak of positive tests in mid-July, widely attributed to increased mixing at summer sporting events which was not followed by a hospital admission peak. A second smaller testing peak in October similarly failed to cause a surge in hospital admissions. We believe this demonstrates protective natural immunity due to prior infections and vaccine effects.
SAGE now predict that the right hand peak in tests will be followed by a surge in hospitalisations on the basis that Omicron will both evade both vaccine protection and natural immunity and cause illness severity at least as bad as Delta. I don’t understand this assumption, given that all the open-source real world data available suggests the opposite. Neither by the way do analysts from JP Morgan who have commented publicly on this specific point.
Even if SAGE are correct in their apocalyptic predictions, as Professor Heneghan observed this morning on Radio 4: “this is as good as it gets”. If we can’t manage to live with Covid with the vast majority of the population double or triple vaccinated plus substantial natural immunity from prior infections, then we are destined to repeat the cycle of lockdowns for the foreseeable future – possibly running into decades. Do any readers want to live like that?
An insight into why this consistent extrapolation to catastrophe may be occurring can be gleaned from Fraser Nelson’s twitter exchange with Professor Graham Medley, the chair of the SAGE modelling committee. It is an astonishing conversation in which Medley appears to say that SAGE only consider the worst case scenarios because presenting more plausible real-world assumptions would not “help” decision makers. I urge readers to follow the link for themselves. As Nelson puts it, this is “policy led evidence making”.
I can provide no better comment than a contribution to the discussion by ‘Reg@ratboy101203’: “This entire exchange has left me open mouthed. To think of all the livelihoods at stake here, mainly because they don’t see the need to model accurate outcomes as it will not make the Government take any action. Scandalous.” Reg is right. It is scandalous.
Finally, today, I turn to the subject of the politicisation of medicine. We have seen this occur in a number of critical areas in the last 18 months – from a complete inversion of our understanding around informed consent, to blatant biases and selective referencing of data. Professor Mark Woolhouse a member of SPI-M said on the Radio 4 Today programme on December 20th “we are not starting from a baseline of zero, we are starting from a considerable burden of illness due to Delta… so there is less headroom than there was”.
A casual examination of the Office for National Statistics data shows that there are 60% fewer Covid cases in hospitals than at this time last year – a Pritchard ratio of 0.4. (15,741 vs 6,321). Doesn’t this mean that there is actually more ‘headroom’ than this time last year – not to mention the 12 month lead time to prepare for a predictable winter surge of a respiratory pathogen? Woolhouse’s remark supports an assertion I have made previously – that the medical establishment is not urging politicians to cage citizens in their own homes to protect the population, but to conceal the inability of the NHS to function correctly. What do you make of that, Reg?











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.