
There follows a guest post by Daily Sceptic reader ‘Amanuensis’, as he is known in the comments section below the line. He is an ex-academic and senior Government researcher/scientist with experience in the field, who says he is “a bit cross about how science has been killed by Covid”. It was originally posted on his Substack page, but I thought it was such an excellent analysis of the UKHSA’s favoured test-negative case-control approach and its problems – especially why it seems consistently to exaggerate vaccine effectiveness – that Daily Sceptic readers should be treated to it too.
There has been much consideration in recent months about the effectiveness of the Covid vaccines, and this leads to thoughts about how vaccine effectiveness is calculated in the first place. The trouble with any attempt to calculate vaccine effectiveness is bias – that is, are the vaccinated and unvaccinated similar enough to make the calculation, or, rather, can we remove any bias to get an unbiased estimate.
As an example of bias, in the early days of the Covid vaccinations the majority of the vaccinated were old, and the unvaccinated were young – so if there was an effect of age then we’d get a biased result simply by comparing overall case rates (per 100,000) in the vaccinated versus the unvaccinated groups. In this case the bias might be resolved by splitting the analysis into different age groups, but what about other factors? Most of all, what is the bias associated with willingness to become vaccinated (maybe the vaccinated are in general more likely to be the healthy ones, say)?
Some time ago, statisticians came up with a really great way to remove rather a lot of the ‘difficult’ bias – it is called the Test Negative Case Control approach (TNCC). With this approach you don’t simply count infections, but compare the rates of infections amongst those who get tested – more specifically, you compare the ratio of positive to negative results in the vaccinated against the positive-to-negative ratio in the unvaccinated groups.
The great thing about this method is that it automatically compensates for many behavioural effects in the vaccinated compared with unvaccinated groups – so, say the unvaccinated are half as likely to go and get tested compared with the vaccinated, the TNCC should remove most of this effect. Of course, many demographic things are of interest (particularly the impact of age and gender), so you’ll usually separate out these variables, but the advantages of the TNCC method remain.
Anyway, pretty much every study on Covid vaccine effectiveness makes use of TNCC – it gives such a powerful and unbiased estimate. You can read more about it in this review article.
Oh, but what’s this I see in that paper?
A key characteristic of the test-negative design is the use of a control group with the same clinical presentation but testing negative for the pathogen of interest. This group of individuals may either be positive for alternative pathogens or negative for all pathogens (pan-negative or undiagnosed). As with any case–control study, the selection of controls should be made independently of exposure status to avoid selection bias. A situation where this assumption may be violated is the presence of viral interference, where vaccinated individuals may be more likely to be infected by alternative pathogens. (Emphasis added.)
Hmm. So it is vitally important that the vaccinated cohort don’t suffer from a different disease that might impact on testing in increased numbers compared to the unvaccinated – if they do then you’ll get a misleading estimate of vaccine effectiveness.
To explain further – the odds-ratio (which is then used to estimate vaccine effectiveness) is dependent on the calculation of (vaccinated testing positive) / (vaccinated testing negative). Thus it would be a problem if you had the same number of positive results but an increased number testing negative – such as if more people are going forwards for testing because of a different disease with similar symptoms.
What’s all that I keep hearing about the ‘worst cold ever’..?
Are we in a position where the vaccinated are getting some other viral infection causing symptoms similar to Covid, are getting tested because the symptoms are right but are then testing negative? If we are then any estimate using the TNCC approach will give a misleading result, and overestimate the vaccines’ effectiveness.
Note that this doesn’t mean that all ‘bad colds’ need to be in the vaccinated group – all that is needed is for the propensity to have a bad cold to be higher in the vaccinated group.
All we need to identify this happening is to look at the relative rates of those seeking testing, comparing vaccinated with unvaccinated (both per 100,000), and try to identify any trends in the data suggesting that the vaccinated are changing their test-seeking behaviour relative to the unvaccinated. Oh. Sorry. Those data are not available… The usual problem.
Hmm. Can we work with other data to try to identify if this particular problem is occurring?
I’d note first of all that it is no good just looking at ‘is there a lot of cold going around?’ While there does appear to be some increase in ‘coughs’, (for example, see figures 28 and 32 of the most recent Government influenza survey), you absolutely need to compare vaccinated with unvaccinated to identify the problem. Without this type of data we’re stuck.
But hold on – what about comparing those getting tested without symptoms? That way the data won’t be affected by any increase in Covid-like disease. Conveniently, there’s a nice paper out fairly recently that does provide these data, from Qatar. In this paper they provide data on both symptomatic disease (which would be affected by a worst cold ever effect if it was occurring more in the vaccinated) and asymptomatic infection (which wouldn’t).
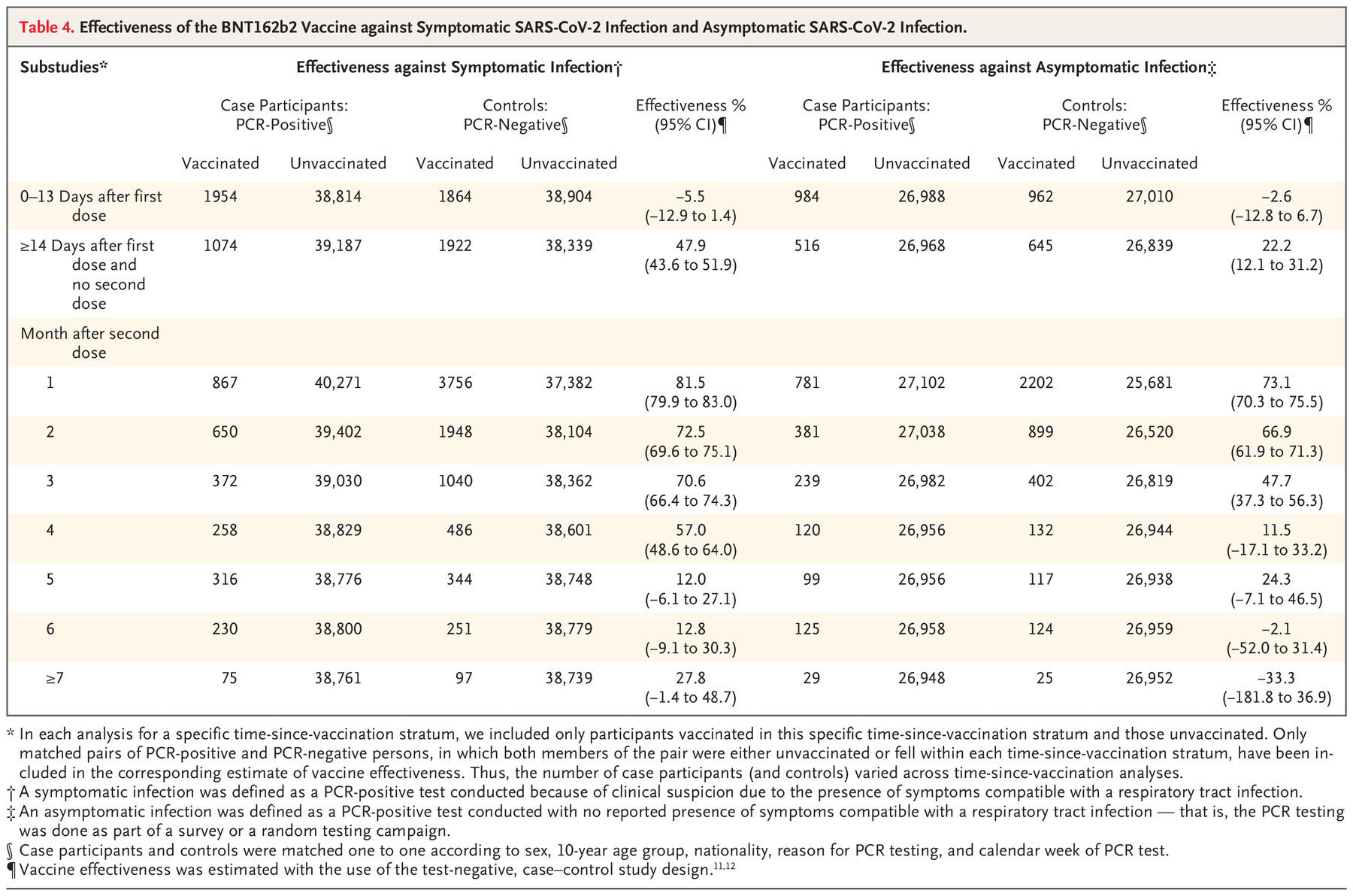
There it is – a significantly reduced (negative for six-plus months) vaccine effectiveness for asymptomatic infections. (The middle column gives the vaccine effectiveness for symptomatic disease, the rightmost column for asymptomatic disease. The rows give vaccine effectiveness by time, with the lowest row vaccine effectiveness after seven-plus months.)
This might be the information we’re after. This would definitely occur if there were more people being tested for non-Covid (but Covid-like) disease in the vaccinated cohort.
Or alternatively it might simply indicate that the vaccines have a negative effectiveness against asymptomatic disease and a positive effectiveness against symptomatic disease. Sure, that’s a terrible result and indicative of problems to come, but it doesn’t prove that the TNCC approach is giving misleading results.
Is there anything else we can do? Let’s go back to that TNCC review paper I linked to early on in this post. In the introduction to that paper is the actual reason why we use TNCC:
Case–control studies present a particularly efficient approach for monitoring VE because they tend to be faster and cheaper than cohort studies.
Okay. What about slower and more expensive approaches? Well, the ‘old-fashioned’ way of doing this is to try to compensate for every potential bias (variable) – this is more complex and requires more data (takes more time/money), but does work well – and is the way it used to be done before TNCC came along. The best way to compensate for bias is using proper cohort studies, where you recruit a number of people, split into two groups with well understood characteristics, and investigate them fully for longer periods of time. Now, this method is expensive and time consuming, but it really does give an indication of how things are going. Even better, if you have enough participants you also get indications of the level of side effects.
I suggest that this should have been done with the Covid vaccine – the initial clinical trials were time limited for understandable reasons, but that didn’t mean we should have stopped looking. In fact, it is usual to have a period of extended pharmacovigilance for newly approved medical drugs/treatments (sometimes called ‘phase IV trials’) and it is rather strange that this wasn’t done for the Covid vaccines. However, it is too late for that now – we’ve vaccinated everyone without taking the effort of selecting a set of subgroups for longer term analysis of the vaccines’ safety and effectiveness.
Luckily, though, it isn’t too late to do anything at all, because there is a way of adjusting for bias in the data using other techniques. The most common way of doing this is the Multivariable Logistic Regression (MLR) using survey data in a retrospective study.
The important thing about MLR is that it does actually work. It could be argued that TNCC is better, but it should at least give similar results – the main advantage of TNCC is mainly that it is faster and cheaper. In particular, having a TNCC that gives markedly different results to a MLR should result in questions being asked, and not simply ‘TNCC is better. The End.’
Is there one? Or, even better – has anyone done an MLR and TNCC on the same data? Amazingly, the Qatar study also includes a MLR. Sure, it is tucked away in its supplementary materials, but it is there in Table S11.
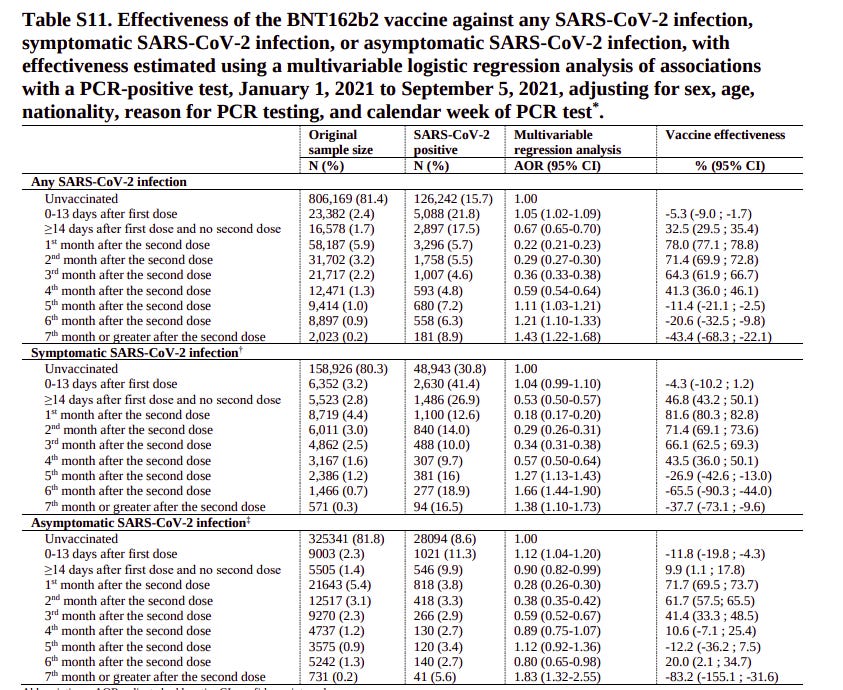
And there it is. Markedly worse vaccine performance for the MLR analysis than the TNCC analysis shown earlier. It is worth repeating that this is for the same data – all that is changed is the type of analysis used.
It is important to note that this isn’t simply ‘well, let’s just add all the numbers up’, as is being done with the UKHSA tables (albeit with age being taken out as a variable) – this is a proper analysis that takes into account age, sex, nationality, reason for testing and calendar week of test (i.e., it tries to remove Covid wave effects). Thus it counters the complaint about the simple analysis done on the UKHSA tables – that biases lead to misleading results.
What’s more, there’s a time effect. The vaccine effectiveness for the MLR is broadly similar to the TNCC estimate up to month four – that’s good, because really you want MLR to be similar to TNCC. This suggests that the residual biases in both types of analysis are low – the two very different methods give the same results, which is excellent. But differences do appear from month five; because the results were similar in earlier months this is less likely to be a simple behavioural (or similar) bias – and that leaves the question I started with – is the TNCC approach failing because of the worst cold ever effect?
I’d also note another aspect to all this. While it is true that we like to ‘do things properly’ to remove bias in important things like ‘estimate vaccine efficiency’, as a general rule it doesn’t make that much difference when you look at a population scale – the larger the numbers you look at the more likely it is that a simple approach will get you close to the truth (so long as the really important factors are considered – usually age). The problem being that population-wide estimates of vaccine effectiveness (e.g. the UKHSA tables) are just so very different from the official estimates from ONS. The MLR results given in the Qatar study suggest that the problem is with the TNCC approach that everyone is using, and that the truth is closer to the UKHSA estimate than the ONS estimate.
One more point. The risk of viral interference, that is, of the vaccine increasing the risk of infection with alternative pathogens, is just one mechanism whereby the TNCC method might give erroneous results. The basic concept of the TNCC method is that the vaccinated and unvaccinated groups are similar; as noted in the discussion of the original review paper I linked to at the start:
Simulation studies have shown that biases may arise under several circumstances, including if the study fails to adjust for calendar time, if vaccination affects the probability of non-<target disease> infections, if vaccination affects the probability of seeking care between cases and controls, if healthcare-seeking behavior differs substantially between cases and controls, and if misclassification bias is present.
And:
The test-negative design may be more appropriate for some vaccines and pathogens, but less appropriate in some scenarios for example if vaccination reduces disease severity in breakthrough infections.
Oh dear. Perhaps it isn’t simply the fault of the worst cold ever – perhaps any number of problems might be resulting in an erroneous estimate of vaccine effectiveness, some of which sound a little too familiar, such as the vaccines reducing disease severity…
Is this analysis enough to conclusively prove that the official estimates are wrong? No. But there are clear indications that something serious could be going wrong and that a much deeper analysis with more data, and perhaps a more appropriate method, is required. Until that is done I’d suggest that any estimates of Covid vaccine effectiveness using the TNCC method should be treated with caution.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
No jab, no job is an affront to a free society: How you can fight back
https://www.conservativewoman.co.uk/no-jab-no-job-is-an-affront-to-a-free-society-how-you-can-fight-back/
THIS week thousands of care workers said goodbye to their jobs, their financial security, their profession and their futures. They also said anguished goodbyes to the care home residents they’d been looking after in some instances for years, not knowing what would become of them or how they’d be treated in view of these mandated catastrophic staff shortages. By Kathy Gyngell
Here are some upcoming peaceful events: What makes this so easy for the Government is everybody is waiting for somebody else to do something……. …. join the friendly resistance …
Saturday 13th November 2pm – Reading
BERKSHIRE STAND FOR FREEDOM
Meeting place: Forbury Gardens Reading RG1 3BB
guest speaker Anna De Buisseret Senior Lawyer
****
Sunday 14th November 1pm to 2pm – Bracknell
Yellow Boards – Stand by the Road
A322 Downshire Way, Bracknell RG12 7AA , Near Twin Bridges Roundabout
***
Saturday 27th November 11am – Bracknell
Stand by the Road Yellow Board MEGA event
By the Peel Centre Skimped Hill Ln, Bracknell RG12 1EN
****
Saturday 11th December 2pm – Henley-on-Thames,
HENLEY, OXFORDSHIRE STAND FOR FREEDOM
Meet by the Town Hall, Market Place, Henley-on-Thames, Oxfordshire, RG9 2AQ by 2pm
***********************
Stand in the Park Sundays from 10am – make friends & keep sane
Wokingham – Howard Palmer Gardens Wokingham RG40 2HD
Where Sturges Rd/Denton Rd meet next to Cockpit Path car park
Bracknell South Hill Park, Rear Lawn, Bracknell RG12 7PA
(Also Wednesdays from 2pm)
Join TelegraM Group http://t.me/astandintheparkbracknell
“it is rather strange that this wasn’t done for the Covid vaccines”
Not strange at all. Entirely consistent with the everything else about the coronapanic. Evil and/or mad liars running the show.
I wonder what all-cause mortality looks like between vaxxed and unvaxxed.
We know that the all cause mortality figures can’t look good for the vaccine because, if they looked good for the vaccines, we would never hear the end of it.
Sod off.
Different name with the same post on a regular basis…
Wind back a bit – to before the snake oil. All-cause mortality was showing no extraordinary levels from the get-go for any group. It would have to have magical powers to alter the shape of a curve that showed only a slightly heightened real-world risk (similar to any quotidian infectious event).
Even the scary effect on the older population is actually largely a myth – the effects of the purported ‘pandemic’ simply mimics the trend of normal mortality throughout the age-range. i.e – in general, the older you are, the more likely you are to die. The similarity of the curves is what is striking – not the anomalies.
There must be some reason why the world lost their collective minds and locked down.
don’t forget healthy people caught Covid and died, Johnson was hospitalised by it. Governments the world over did the same collective actions.
covid 19 is not a myth, I think the conspiracy is still to be unearthed. China are still heavily locking down when a few people blow there nose & I suspect they know far more about this thing than anyone is letting on.
it’s important to ensure the science and statistics stands up to scrutiny, comprehension then needs attributing to the results.
government actions from China to the North Americans does not align to the statistics. I think that was obvious from the start.
I think the question is why take such actions when the data never supported it and those making the decisions and doing the calculations knew the data would not support it.
there must be something else to Covid that is not widely known that causes nations like China to lockdown because of a sore throat.
“don’t forget healthy people caught Covid and died”
… as happens with any transmissible disease. If there is anything to remark, it is how relatively few healthy people died. Most had co-morbidities.
When did I say that SARS and ‘Covid’ (which is actually something else) is a ‘myth’? The myth is the narrative about it – that is something exceptionally dangerous.
I suggest yo look into the pre-history of dodgy dealing over the political use of Corona health scares as a political weapon for your ‘something else’. Pay particular attention to the Council of Europe report on the Swine ‘Flu fiasco. It’s powerful, because it is couched in very moderate diplomatic language.
I suggest we abandon the term ‘conspiracy’ for ‘confluence of interests’ and ‘power’.
Indeed, not in the least strange that this wasn’t done for covid vaxxes.
What I find most horrific about this, is that mRNA vaccines now seem to be accepted for use in humans, because so many millions of people haven’t dropped dead yet. It is now clear there is no way, nor worse, any intention, of carrying out long-term checks on possible (serious) adverse effects of mRNA, something for which there would appear to be enough potential. There is no control group, there has been no follow-up. Cancers, MS, prion disease, auto-immune disease, should these arise over the next 5 to 10 years, how could it be traced back? Particularly when authorities are pulling out all the stops to get every man, woman, child and undoubtedly soon pets poked, removing any form of control group. I’m not saying such things will arise, but they are possibilities and real scientists and doctors who actually care about their patients should want to know.
It is clear that some scientists (look up Fraudci in a CSPAN conference end of October 2019, literally wishing for a major flu outbreak so they could try out mRNA vaxxes) have been drooling to get mRNA into people. Now, without any science to back up long term effects, it is clearly being geared up for deployment in other vaccines already, as many politicians and scientists have been happy to convince themselves that this outrageous mass experiement has been successful and safe – with no evidence to back that up.
They declare success based on their own views, but real world death and infection rates say otherwise. They declare safety without any long-term data and with disgraceful ignoring of adverse event reports.
Yes indeed – crass stupidity or evil to mass vaccinate with a poorly tested and experimental vaccine. The opposite of safety-first.
The vaxx roll-out was only ever about ‘money first’ for the pharma industry. No doubt part of that was based on a “winner takes all” approach. Even if one or 2 companies had wanted to wait a little longer, we have seen with Novavax and Valneva that that would simply mean losing out to the winner. Moderna is quietly being set aside, a few countries here and there, more to follow. Advised against first for the under-30s, now for pregnant women, I expect it to be abandoned entirely within a few months. Pfizer, which has shown exactly the same problems as those for which Moderna is being set aside, will at some time be retired as well. Who the hell will be willing to take any of this poison after this, even a traditional inactivated virus vaxx? Certainly not me.
I think Moderna is being eliminated for the same reason Astrazeneca was – for Pfizer to obtain a monopolistic position on the market. I guess Pfizer’s bribes were simply the highest, and the vaccination market is by design very prone to this “the winner takes it all” phenomenon (in order for a new vaccine to be admitted, during normal times, it must be at least as good as the already used vaccines).
As for the arguments that the world will end, these same arguments can be used for any new technology (e.g. also for the regular flu vaccines). They are nonsense because before the technology is introduced testing is done on animals to figure out long-term effects. This was no different for the mRNA vaccines (and yes, there have been some problems in animal models – which were fixed, and which is what allowed the human trials to begin in the first place).
As for the argument, if you do X, how do you know it won’t cause something terrible Y years down the road, it can be applied to any decision whatsoever. And even if you decide not to make no decisions in life “for safety”, it may turn out as the worst decision you’ve ever made. So I suggest you stop being more hypochondriac than the covidians, and get over it.
…if you do X, how do you know it won’t cause something terrible Y years down the road, it can be applied to any decision whatsoever. Normally you would carry out some cost-benefit analysis to try and answer that question. Robert Malone (one of the pioneers of mRNA vaccines) has pointed out there are reasons to suspect that injecting mRMA into people at regular intervals (every six months or so) may have potential long-term adverse effects. Balance this against the known facts that (1) healthy persons (especially the young) are at almost negligible risk of serious illness from Covid-19, and (2) that immunity acquired through infection is far superior to vaccine-induced immunity, then I would suggest the policy of injecting all healthy individuals is immoral.
Fortunately Robert Malone is not the only person in the world capable of doing cost-benefit analyses.
The morality of protecting one group by putting another group at (very small, but non-zero) risk is arguable. From an individual standpoint, it does seem unethical, from the standpoint of society it seems ethical enough. And what seems unethical for an individual in the short term may actually turn out as ethical in the longer term (e.g. by avoiding a wider social disruption which strikes back at the individuals like a boomerang).
As another example, allowing people to work in a hazardous environment for modest pay, may seem unethical, and yet the society tolerates it and demands more of it for its own benefit.
Overall, the world is neither just nor safe, and the more powerful often make decisions to detriment of the less powerful. That’s also the main reason why adults can decide to vaccinate kids and not vice versa, and why the unvaxxed will not be able to override whatever laws are passed to discriminate against them.
Blimey, if you have to spout bs can you at least do it in a brief manner.
I assume you are aware that all animal tests on previous mrna therapy jabs ended because the animals died and there were no animal trials carried out on the clotshots they’re currently administering.
That’s of course one of the lies spread by the antivaxxers. (Brief enough for your mental capacity?)
Nope. Not a lie. The prior tests all failed because of ADE
“They also discuss the lack of proper animal studies for the new mRNA vaccines, and the theory, espoused by virologist Geert Vanden Bossche, Ph.D., that mass vaccination with the mRNA vaccines could produce ever more transmissible and potentially deadly variants.”
https://www.theburningplatform.com/2021/06/18/inventor-of-mrna-technology-vaccine-causes-lipid-nanoparticles-to-accumulate-in-high-concentrations-in-ovaries/
“Emerging data have shown that the S protein itself is a crucial element responsible for the vascular pathology of SARS-CoV-2 virus infection (8). Therefore, C-19 vaccines that induce human cells to produce the very same protein that is involved in viral pathogenicity should be carefully tested to make sure that such protein is not expressed systemically in the body after vaccination, or the effects of vaccination could result in a pathology similar to C-19 disease itself. However, data on the biodistribution in the human body of de novo synthesized S protein after vaccination are, for example, lacking and there were no pre-clinical animal studies done to evaluate this either.”
https://www.geertvandenbossche.org/post/why-are-the-current-covid-19-mass-vaccinations-to-be-considered-a-public-health-experiment
To be clear, rayc, Gerd know more about viruses, pandemics and vaccines than you will ever even begin to know.
I guess he’s lying too?
“Geert Vanden Bossche received his DVM from the University of Ghent, Belgium, and his PhD degree in Virology from the University of Hohenheim, Germany. He held adjunct faculty appointments at universities in Belgium and Germany. After his career in Academia, Geert joined several vaccine companies (GSK Biologicals, Novartis Vaccines, Solvay Biologicals) to serve various roles in vaccine R&D as well as in late vaccine development. Geert then moved on to join the Bill & Melinda Gates Foundation’s Global Health Discovery team in Seattle (USA) as Senior Program Officer; he then worked with the Global Alliance for Vaccines and Immunization (GAVI) in Geneva as Senior Ebola Program Manager. At GAVI he tracked efforts to develop an Ebola vaccine. He also represented GAVI in fora with other partners, including WHO, to review progress on the fight against Ebola and to build plans for global pandemic preparedness. Back in 2015, Geert scrutinized and questioned the safety of the Ebola vaccine that was used in ring vaccination trials conducted by WHO in Guinea. His critical scientific analysis and report on the data published by WHO in the Lancet in 2015 was sent to all international health and regulatory authorities involved in the Ebola vaccination program. After working for GAVI, Geert joined the German Center for Infection Research in Cologne as Head of the Vaccine Development Office. He is at present primarily serving as a Biotech/ Vaccine consultant while also conducting his own research on Natural Killer cell-based vaccines.”
And who is going to decide what is in the greater good? You might be happy to live in an authoritarian nanny state, but many of us do not want to have every aspect of our lives controlled by a corrupt, do-as-I-say-and-not-as-I-do arrogant elite. So, matey, my message to you is quite simple – FOD.
“And who is going to decide what is in the greater good?” Fortunately not you.
There were no pre-clinical animal tests of the mRNA vaccines for safety, at least none that were published. There were some tests for efficacy.
What a very strange argument, not up to your usual standards. I suppose when you put being abrasive over being informative that can happen.
In any event, you are being very sloppy. I am aware of the fact that mRNA has been trialled for quite a long time in animals. Besides the fact that that in itself does not constitute sufficient reason to say it’s okay to inject it into half the world’s population in a matter of months, none of these trials were for a vaxx for this Corona-Sars2 – unless there’s something you know and would like to share with the rest of us. You may as well say “we know the polio virus works, so all new vaxxes work, we know this without trying them out”.
This isn’t even necessarily about mRNA itself, but how the immune system interacts with the virus – there are studies that indicate the antibody response to the spike protein causes problems, so any vaxx would be a problem, the same applies to the possibility of ADE with coronaviruses, known to be the case for SARS1 and Mers. For that reason alone there should have been longer research.
As for your remaining point. First and foremost, I base my decisions on whether I wish to do X or Y in the first place, then I weigh up pros and cons. At no point did I wish to take this vaxx, in the same way that I do not wish to take the flu vaxx, I think neither one, whether safe or not, will provide me with any benefit, so why would I bother? If I were a hypochondriac I would have taken the chemicals and be lining up for shot 3 and booking no. 4.
These “rushed development” concerns may have sounded (somewhat) reasonable at the beginning of the vaccinations (which is also why people were allowed to hold out for a long time), but they have not proved as valid with passing time and with the increasing number of (then voluntary) test subjects. The main reason why these vaccines were introduced in such a rush was of course the pandemic itself – which did not give the luxury to wait and see (from a public health perspective).
The whole vaccination campaign was screwed up big time by portraying the vaccines as candy. I suppose it was done to appeal to the dumb majority. The actual rationale was to choose the lesser evil – better use a well-working vaccine (even if there might be some shadow of doubt about safety) than let unvaccinated people get infected with the virus, leading to much worse consequences such as a health system crisis.
The major mistake that those who reject the vaccine make is to ignore the (relative) risk of catching the virus itself. The safety and natural immunity argument collapses because if you pretend that you are so healthy and young to be able to cope with the virus while unvaccinated, then you should also deem yourself healthy and young enough to cope with the vaccine (which after all is a less intense simulation of the virus).
As you are aware, the ADE problem was well-known prior to the development of the current vaccines and addressed before they were brought to market. After more than one year of use, there is no evidence whatsoever of ADE occurring with these vaccines. If you claim otherwise, do point me to some solid research/data on it – not just some anti-vaxxer speculations.
The issue is not whether or not you “wish to” take this vaxx, the issue is whether or not your decision is reasonable or harmful to society. You may not “wish to” avoid driving under influence, but the society, based on available statistics concerning drunk driver accidents, has decided that it is better to keep you from acting so. Sometimes your wishes and benefits are overridden by others’ wishes and benefits. A minimal risk of problems may justify a much larger risk of someone else dying after you infect them (and yes, the vaccines do reduce transmission rates, if only temporarily).
You may also not wish to pay taxes, but yet you must, and will be forced violently if you don’t. I know this sucks, but such is the price for living in a modern society.
Good evening rayc,
Can you provide measurements or studies that prove this? I’ve looked several times and been unable to find any.
There are quite some problems involved with proving that this statement is true. You would need to be able to measure the impact of both vaccine and the range of possible viral infections in comparable units, ideally, units with some sort of biological grounding. Comparing symptoms is fraught with difficulty because the vaccine enters the body in a different place and via different mechanisms. For example, COVID is primarily a disease of the lungs, but the vaccine doesn’t enter via the lungs, so even if it was equally as intense as an infection the symptoms would be different.
The ideal would be a comparison in terms of number of cells destroyed. The mRNA vaccines cause the body to attack itself, thus some cells are recruited into the process and end up being collateral damage. A viral infection also destroys cells, so it seems like a natural methodology to compare. But no such comparison is possible, of course.
Another approach is to look at how dosages were calculated. Unfortunately there we also mostly draw a blank. Because the vaccines are proprietary technology, information on the exact methodology is scarce. It appears they may have simply started with doses known to not be immediately toxic from animal studies, and then increased it until tolerance become too problematic. This approach isn’t going to obviously lead to a lower impact than infection itself, especially given that for many people infection appears to be largely a non-event.
I’m not trying to trip you up here or pick a fight. I would love to find in depth research that lets us measure the “intensity” of infection vs mRNA vaccination. If you know of any, please do provide links.
Thank you for the more considered reply. I must say, it does look like you have some personal interest (I don’t necessarily mean financial, perhaps scientific, who knows) in these vaxxes, you seem to be so keen to defend them.
If you are personally happy with them, that’s great, but at this point there is no evidence to support how they have been rolled out and how they are currently being pushed.
Was it so reasonable to rush it out? The greatest problems of the last 2 years stemmed from the lockdowns, not from the virus itself. Even if they felt safe enough to rush them out, there was no excuse whatsoever to unblind the control group. By definition, those participating in what were genuine trials knew full well they were exposing themselves to risk, that was the entire point. To say it was unfair to leave those in the control group without the option of taking the vaxx (after a measily 2 months) for a virus with this fatality rate was ridiculous and smacks far more of specifically wishing to get rid of the control group to avoid unfavourable comparisons. The group was 23,000 people in different parts of the world, hardly enough to overwhelm health systems.
As for it reduces infections – I guess we must be looking at different planets. The UKHSA data is very clear, no matter how many excuses they try to come up with to say otherwise, Dutch data follows the same path. The same applies here. The head of the Dutch OMT said 4 weeks ago we were in a different place than last year because of the vaxxes, no way would we have the number of infections or hospital admissions. This after the data from Israel, which came in months ago. He has referenced that data and the data from Qatar in official communications. He will have known of the waning effectiveness since at least August, older people here got their second vaxx around Feb, we are well beyond the 6 month mark, yet booster 3 was only planned for December, now pulled forward to next week. If these vaxxes work at all, then the current wave lies with the politicians and OMT for not staying on top of it. They have known since the summer that the vaxxed carry and transmit the virus and went out of their way to ensure that they can continue doing so, while restricting the much smaller group of unvaxxed.
I don’t know if any official reports stating there is ADE exist, but to me that means nothing. At this particular moment in time, who the hell in power would admit to that? But what I can see with my own eyes gives me no reason to believe it is impossible. The Qatar data is interesting, with a higher negative effectiveness rate for symptomatic infection at 6 months than at 7 months.
My decision being reasonable or harmful to society? What is that supposed to means in terms of an airborne respiratory virus? Why not take it all the way and insist that those who test positive put a plastic bag over their heads for 10 minutes? The virus will spread, this is beyond evident now, vax or not. It is not my responsiblity to ensure that the health care system is not overwhelmed, it is the responsibility of the government to ensure that the health care system can cope.
In addition, arguments as to societal good take more than one form. Some of us set great store by constitutions and other safeguards of fundamental rights and freedoms, that protect all in society, even if such rights are not always convenient. Forcing this vaxx on people, for a virus that in the grand scheme of things is not particularly dangerous, to cover up the poor policy decisions of the government and their failings in providing basic health care does not constitute good reason to violate the constitution, quite the contrary.
One could just as equally argue that it is not good for society to put those under 70 who are still productive taxpayers at risk to protect those who are over 70 and not taxpayers. Not my argument, as I do not side with the bogus “good of society argument”, the clarion call of totalitarian rule of the ages.
As to whether or not I wish to “risk” infection or “risk” the vaxx, in a free society that should be entirely my choice, as the end result will most likely be the same (except that natural infection is not a given, once a needle is in my arm, the pathogen in my body is a given). Again, in terms of duty to society, the better argument is to say that it would be better to lock up those most at risk rather than put a healthy, productive taxpayer at even minimum risk.
Which suggests you think spike proteins are innocuous. Frankly, as a very healthy human being, I’d rather have Covid than an experimental jab which forces your body to manufacture extremely toxic spike proteins which can harm many of your vital organs and cause clotting.
I’ll leave that for you to experiment with.
I didn’t pretend to be sufficiently young and healthy to be able to cope with the virus; I was aware of how vanishingly rare it is for healthly people of my age to be seriously affected by it. No pretence required. I was proved right. A few days of fever and strange taste sensations, a fortnight of being a bit weaker than usual, then back to normal.
I experienced the same thing In January 2021.
If it wasn’t for all the covid19 propaganda I would have assumed I had suffered a moderate flu.
‘As you are aware, the ADE problem was well-known prior to the development of the current vaccines and addressed before they were brought to market. After more than one year of use, there is no evidence whatsoever of ADE occurring with these vaccines.’
Given that the vaccines only started to be deployed in late December 2020, with many nations not starting their roll out until the middle of spring, I think you are being somewhat hasty in declaring that there is no evidence of ADE.
I think we will have to wait for this next winter season to pass, now that a great many people have theses mRNA injections in them, to see if ADE is a problem.
Excellent article. Even managed to make sense to a numpty like me which is quite an achievement!!!
lol Me too.
Thanks, appreciated.
Long, long ago, I seem to remember Bozo and his gang citing something called the Precautionary Principle.
Now what was that about…?
Actually, normal scientific process (the testing of a hypothesis against a probability of randomness) is the proper application of ‘the precautionary principle’.
The Precautionary Principle isn’t one option but two options – and most always cite the first option – It’s better safe than sorry. The other option, equally and often more relevant is, What are the consequences of following the first option? You know the answer: Shutting down a country’s health system for two years for a moderate illness posing a danger to a sliver of the population. Those are the consequences of misusing the PP.
Sounds just like that old fashioned notion of a ‘cost benefit analysis’.
Reminded me of the recent study lauded by the FDA which I think was a test negative case control study, where the cases & controls were tested in context of being hospitalised with respiratory (COVID like) symptoms. Could you do a follow up on the statistical issues involved in a TNCC study of that particular type (ie testing in context of respiratory hospitalisation), given that the vaccines are intended to reduce severe symptoms? Was the main problem with how that study was presented by the FDA & media that it could properly be used only to infer conclusions about vaccine effectiveness in terms of severity, but was presented as saying something about effectiveness in terms of sterilising immunity?
I’ll have a look at it.
The Amish achieved zero covid by not reading studies
Statistics left me cold at ‘0’ Level but I recall in the very first weeks of Lockdown 1 medics telling me of something they called ‘Clinical Covid’. This was used to describe inpatients who presented many Covid symptoms, who were listed as Covid Patients (mortalities?) yet who consistently tested negative.
Never did read about theses pseudo-covids in the press.
no need to worry. He’s just saying TNCC is better than nothing, but still not right, there is no simple way to get the vaccine efficacy due to other factors. but the best methods do not yield negative efficacy.
..but the best methods do not yield negative efficacy.
Best for who? I’ll stick with the raw UKHSA tables, until it is clear that they are wrong. The cold hard facts are obviously upsetting for many working for vested interests. Their fiddling and the over finessing of these very inconvenient numbers is only to be expected.
.> Best for who?
best in the objective sense i.e. most true, vaccine efficacy can be determined easily in a large unvaccinated population. just give a small known sample the brand new vaccine, and give another equal sized known sample no vaccine, after a spell of time count who caught it in both groups and compare. if few in the vaccinated group caught it, while many in the unvaccinated group caught it, clearly the vaccine works, and that is what the trial showed.Once everybody is vaccinated the opportunity to do this dries up. Whicjh is why TNCC is dreamed up.
Nope. Thats not what he said. He said they have been using a maths hack which is understandable with short time scale data but we now have more than enough data to do far more rigorous traditional analysis which shows very different results.
It very easy mathematically to have negative efficacy. If the vaccinated group have an higher infection rate than the control group, thats negative efficacy. A not unusual situation during clinical trails.
For the SARs CoV 2 vaccines used as a public health measure around zero or negative efficacy is to be expected. The vaccinated group is seriously biased toward high risk people. The high risk group disproportionately are those for who vaccines have low / zero efficacy. Due to weak / impaired immune system. So the vaccinated group will have higher infections rates than the unvaccinated group. Mathematically thats negative efficacy as a public health vaccine. Which was the whole point in the first place.
What crap logic!
Glad its not just me! ewloe and jmc have stood on the pin head upside down to try to produce arguments which are simply illogical.
Public health measures clearly include killing people according to these people. Which I guess is born out by actions over the last 20 months.
It’s one reason why I make pleas to first get back to the simple facts of the matter. I am all in favour of using good statistical method as well – but in this case, the basics are, in themselves, utterly destructive of the Narrative smoke-screen.
That’s what pissed me off about ‘0’ Level Stats, and Economics, if the results don’t match what is required just weight some inputs until they do. I expect they have refined the technique over the past 40 years.
Its the maths, stupid. Thats how this stuff works.
Efficacy is defined as how much a therapeutic treatment reduces the incidence of the target disease in a particular group as against a specified control group.
That’s pretty easy to understand. Is nt it.
Ideally you have two exactly equivalent groups where the only difference is the therapeutic treatment. That is what a normal clinical trial looks like.
This is not what we have here. Repeat. This is not what we have here. With those numbers being discussed.
We are comparing two groups where the are many differences between the make up and constituency of the two groups. And the single biggest difference is that we have sorted most of the high probability of infection people into the vaccinated group and those of lower probability into the unvaccinated group.
So guess which group gets the most infections over time?
Now back to the definition of efficacy. Group A get vaccinated, Group B does not. If Group A get 0 infections and Group B gets 100 then thats 100% efficacy. If Group A get 10 infections that 90% efficacy. And so on…
But if Group B get 100 infections and Group A get 200 infections then what efficacy is that? By definition thats negative. There is no positive outcome by the definition of the problem. And in case you are wondering negative efficacy is not uncommon during proper clinical trials with proper control groups. In fact it was one of the most severe side effects during some previous mRNA vaccine trials. Where the efficacy went very negative after time due to immune systems response to subsequent infections attacks. Worked OK initially. But on subsequent infections the immune reposition collapsed completely. That one of the reasons no mRNA vaccine candidates ever got regulatory approval.
My logic is perfect. Because it is based on the actually mathematics of the subject being discussed. Sorry if your grasp of the maths isnt.
> A not unusual situation during clinical trails.
which did not occur with the approved vaccines.
Those “other factors” being data withholding.
“TNCC is better than nothing”
Trans : ‘Any old shit results will do’.
Oh dear!
https://www.gov.uk/government/publications/temporary-medical-exemptions-for-covid-19-vaccination-of-people-working-or-deployed-in-care-homes/temporary-medical-exemptions-for-covid-19-vaccination-of-people-working-or-deployed-in-care-homes
One thing that I hadn’t realised is that care home workers can self certify exemption from compulsory jabs until 24th December after which they need to use the NHS app and get an official exemption from their doctor. They have a further twelve weeks in which to do this. It will take them up to the end of March which will put them almost in line with the April 1st deadline for all other NHS front line staff.
I also believe that Scott Gottlieb, the former FDA commissioner, has said that he believes that the pandemic, (such as it is) will be over by January in the USA before Biden’s mandates come into force.
Interesting!
> the pandemic, (such as it is) will be over by January in the USA
how could he know, cases in America have been falling, but that seems to have slowed up, I hop Gottlieb is right….. only time will tell.
“I hop Gottlieb is right” Hope or not, there’s nothing you or I or anyone else can do about it, except probably look into ways to treat covid effectively, preferably with existing safety-tested treatments, improve the provision of healthcare (rather than hobbling it or shutting it down) and dial down the panic and let the healthy population get us to something approaching herd immunity. All things that governments could have done but chose not to. In fact almost everything governments have done has been directly or indirectly damaging to public health – the exact opposite of what they claim. It’s by far the most colossal fraud in history, the Biggest Lie ever told that has been believed by most.
My thoughts entirely. Common sense, it seems, isn’t so common.
Scott Gottlieb is also on the board of Pfizer !
> I also believe that Scott Gottlieb, the former FDA commissioner, has said that he believes that the pandemic, (such as it is) will be over by January in the USA before Biden’s mandates come into force.
From the CDC data the pandemic ended around early / mid Q3 2020 . When it comes to FROM deaths involving pneumonia / ARDS. Which is the standard criteria with viral respiratory infection epidemics.
At the moment its casedemic in the Blue states / small population states and pretty much back to normal, i.e early winter flu season, in the Read states. So purely a political disease by this stage.
The one twist is that hospital capacity already seriously reduced after last years shutdown for non SARs cases, lots of wards closed due to financial losses, are now having wards shutdown due to lack of staff due to vaccine mandates. Not just due to loss of nurses either. A huge problem in Blue state cities. Cleaning staff, food prep etc are leaving too. Admissions are already being curtailed in quite a few states due t o basic services no longer available due to staff shortages. A lot of this work is contracted out and the contract workers can work elsewhere.
Perhaps it’s time to turn the screws on reluctant GPs. An example :
I take blood thinners – as do many others for – for well-known reasons.
Should a GP question giving an exemption certificate, I would ask whether he can guarantee (and sign a statement) that the administration of a jab will not enhance my risk of clotting, given my observed medical condition and the known enhanced risk in this area from the jab.
Failing such assurance, I have rational grounds for exemption, and I am sure that others can find other such situations.
The point is that, under normal ethical standards, there has to be some really exceptional reason for over-riding my judgement
Join https://members.vaxcontrolgroup.com/record/WWSGMJU3KRHSWBQHDAWAVQ and fill your own exemption form, as part of a control group for those not vaxxed
Self exemption form
https://vcg-templates.s3.amazonaws.com/promic/Editable_PROMIC_Self%20Exemption%20Form_v10821_1.pdf?AWSAccessKeyId=AKIAX3RRMLSMLPANLJPG&Signature=wkx6ZmxSAv1mjn1PENuXJIuWUN4%3D&Expires=1636888886
GP exemption form
https://vcg-templates.s3.amazonaws.com/promic/Editable_PROMIC_Health%20Professional_Exemption%20Form_v10821_2.pdf?AWSAccessKeyId=AKIAX3RRMLSMLPANLJPG&Signature=UbNwsiIv3hUBeUXW8cTkhcSF2Kk%3D&Expires=1636888886
You will also receive an ID card stating that you are part of a control group of the non vaccinated.
Stand up for your rights.
See the ID card here
https://vaxcontrolgroup.com/
Yet these are folks who in most cases have for some 18 months been working unvaxxed in care homes. They will either be immune, or have had Covid. And hence be immune. Jabbing someone for a disease they are immune to makes no sense, all the more so now we know how dangerous these jabs are.
“get an official exemption from their doctor.”
Apologies for being a bit dense, but what is a doctor?
In summary, TNCC is not a silver bullet but better than nothing. Basically there Is no simple clean way to find vaccine efficacy, Spiegelhalter was right, he vaccines have good efficacy unless the data is processed using an oversimplified procedure.
Can you clarify what you mean?
No simple way to measure how good this works but here, stick it in you anyway? Or else you lose your job no less.
And are you also saying that Qatar study is bunk and a waste of time? Because vaccines work?
So the whole process is bollocks?
… so there can be no assurance of efficacy that over-rides the possibilities of harm?
… so, you agree that the ‘vaccines’ cannot be used on the basis of any short-term justification?
Fair enough.
except for the initial trial, which were impeccable.
I think you’ve read a different article to me!
Sent the following to my MP at 4 this morning….
As one of your constituents I am writing to express my disgust at your attending any remembrance services for those who gave their lives for our freedoms.
Freedoms you and your ilk are now destroying.
Vaccine mandates for care staff, when the primeminister himself has stated the so called vaccines don’t stop you contracting or spreading covid19. An experimental (it’s still in phase III trial) therapy jab for which the mid to long term adverse effects are still unknown. The short term effects are beginning to be realised with over 1750 deaths and 1500000 adverse reactions reported to the MHRA yellow card system, again all official data and recognised to be possibly as low as 10% of the true figures of those of effected. All for a disease with a fatality rate (from governments own data) of 0.12%, very similar to the flu and an average age of death in the over 80s.
You and the rest of government and parliament are total hypocrites.
One day there will be a reckoning, hopefully within your lifetime but definitely on your demise and you will all be found to be wanting at which point I trust the fires of hell will be burning strong.
Received the following at 09.11….
I note your email.
I will be proudly there Sunday morning, with many others who have served their community over the last 18 months as it faced the pandemic.
Remembrance is about those who sacrificed their lives for the ability to live in a democratic society and for people to be able to express their opinions, no matter how wrong or ill informed most would believe they are. With nearly 90% of xxxxxx’s population having received at least 1 jab the majority do not share your conclusions or suggested experience.
As for your comments on the afterlife as a Christian I believe Christ harrowed hell and offers his grace to all, with the Holy Father and the Archbishop of Canterbury having received their jabs their guidance is very different to your view. With Pope Francis saying getting a Covid jab that is “authorized by the respective authorities” is an “act of love.”
Since he has failed to respond to any of my previous 6 I’m hoping that this one actually caused him a twinge of doubt/fear, probably not, but I live in hope, it’s all we have these days.
I wrote to my MP back in April 2020;
With it, I included links to the Nuremberg code, Universal Declaration on Bioethics and Human Rights etc. I never did get a reply.
And if you were Blackford and received this crap, would you bother to reply?
Well, many would say that Blackford is himself a pile of steaming crap.
Same here – and this from an excellent constituency MP who has answered many emails and letters I have sent him. I think I am going to get a date at his surgery and dump all the medical papers I have collected which state clearly that the jabs are a catastrophe.
“Remembrance is about those who sacrificed their lives for the ability to live in a democratic society and for people to be able to express their opinions no matter how wrong or ill-informed most would believe they are.”
Where’s he been for the last two years? Living under a stone? There has been no debate at all allowed against the narrative.
His argument about the 90% not sharing your conclusions fails to take into account how many were hoodwinked into taking the jab because they thought it would allow them to live freely and travel once again or were told it would stop them getting Covid or passing it on.
You are correct. He’s a total hypocrite.
He’s been busy clambering up the greasy pole as fast as he can to the extent that his head is now so firmly wedged up the arse of the degenerate above him he is blind.
Like the vast majority of us most people who took the jab have no idea how it works or even if it does. At least with a car, a raygun or a computer we can see the actual results of technology without knowing how it works, not so a vaccine.
So you are correct to say that most people took the jab in order to escape the restrictions placed on their lives through lockdown with perhaps an element of blind faith.
Totally agree and as I posted yesterday these people are more than that, they are ‘weapons grade’ hypocrites (forgive the wartime analogy).
You’ve a good one there, definitely eligible for the ‘do not resuscitate’ treatment.
Our MPig sounds like a carbon copy, but they are all reading from the same script aren’t they?
I feel reassured, not! Such a pity your MP didn’t look a little further into the differing bio-politics of the RC Church, particularly the views of Archbishop Carlo Maria Viganò warning the public about:
…the danger of ‘experimental genetic’ vaccines, vaccine mandates, media terrorism, the complicity of Pope Francis in Klaus Schwab’s Great Reset global coup d’etat, the Rockefeller Foundation’s Lockstep Plan, and how the climate change deception is being used to accelerate an elite agenda for a New World Order, and much more.
Sorry – but this was a totally pointless exercise, even given the assumption that your MP actually has any grasp whatsoever. There is a point where you just have to recognise th futility of an action.
The Flaw at the Heart of the UKHSA’s Vaccine Effectiveness Study; The “Vaccine”
I understand that somebody was shot dead in NZ and as he proved covid positive his death was recorded as Covid and not lead poisoning.
Yesterday’s roundup ended with a NZ video news report on the subject.
They are still at the stage of ‘anyone who ever had Covid must have died of covid’ even if, as in this case, they were shot down dead.
You always been very good over sight over facts (and I write that as someone who has chosen not to be vaccinated like 50% of our family). It is certainly true a lot of double vaccinated people have caught covid including in this family but I always want absolutely accurate facts.
Except we are not talking about traditional orthodox vaccines here, but experimental emergency-licensed treatments being administered by needle under draconian government regs. This fact keeps getting lost. And just as Webster’s dictionary has duly altered its definitions to fall in line with last year’s WHO edict to include experimental gene therapy, we are in danger of forgetting what ‘vaccination‘ and ‘inoculation‘ (words routinely wrongly used by this government’s propaganda machine) have always meant.
Similarly the roll out of the ‘asymptomatically infected’ category should always set the amber lights flashing. Many eminent medical experts argue that the whole notion of asymptomatic infection is a nonsense, and has only gained favour because of the unreliable (indeed not fit for purpose, as admitted its inventor) PCR tests, where if one really wants to find a covid type infection just up the cycle rate until it appears!
Much of this analysis might have been meaningful 6-8 months ago, and yes the data was available, but at this stage it is perhaps largely redundant as most of the population have been vaxxed already regardless. And yes, vaxx is a matter of personal choice, no matter how sickening the coercion, but using that vaxxed status to claim a vaxx passport to promote a two tier society is something else altogether.
It is fascinating reading, but I think there are a number of issues with this analysis.
How do you think we should measure VE?
Case Control studies, especially TNCCs, are a practical way of doing it. But don’t separate the symptomatic from the asymptomatic for the reason I gave above.
“Asymptomatic” is nonsense as Dr Mike Yeadon has eloquently explained.
Assume it is true that symptoms are masked in the vaccinated, but the viral load is the same in the unvaccinated symptomatic comparator. Because the protection in the vaccinated person isn’t in the mucus membranes and so infection is non sterilising only symptom reducing, by excluding the asymptomatic vaccinated person you miss a major source of transmission by only comparing the symptomatic as a control.
Sure you want to know if the vaccines protect against asymptomatic infection. I just don’t think you can validly separate symptomatic from asymptomatic if you are doing a TNCC. At least you can, but you will be measuring the relative prevalence of asymptomatic infection but this will not be a measure of the ability the vaccine to influence that relative prevalence.
“a”-symptomatic” – read “non-“, and separate from ‘pre-‘. The latter is a very narrow window.
i.e the notion of ‘asymptomatic infection” is bollocks. Although the dangers of symptom suppression by jab may be real.
When the unvaccinated outnumber the vaccinated 9:1 in ICU wards in a country with 65% vaccinated population, I’m pretty sure no further analysis of VE is required for the purpose of making the “vaccinated are better off” argument. You see, somehow the vaccinated don’t end up in the ICU wards with their “worst cold ever”.
Unless you can provide an alternative explanation of what is causing all the unvaccinated to get hospitalized or just have fun in discussing moot points for the sake of appearing clever, like our good Doctor Jones.
Which country is this? Would you make the assumption that the two groups were equivalent in other respects?
Germany. If you claim the groups are NOT equivalent, pray tell us, how are they different? Are unvaccinated supposed to be all much older and sicker than the vaccinated bunch? Or much more fond of coughing at each other?
Are you sure the figures you quote have been adjusted for bias?
Based on what I’ve read here about the increased confidence of the jabbed, one could argue that the unjabbed are more likely to turn up at A&E, thereby skewing the data.
What’s wrong with that?
In any case, if the adjustment for bias arguments negate the latest UKHSA data, then why would the same effect not negate your data?
Sorry, sunshine, but the low real-world efficacy of the jabs – estimated from what proper (within the usual pro-medication distortions) trial data briefly existed That has been long known – it hovers in the 1% area. All the rest is propaganda and bullshit.
Do catch up.
No need to catch up with your confabulated bs.
One obvious confounder is that the vaccinated – a group self-selected for trust in medical authority – are being explicitly told that if they get sick they won’t need to go to hospital, because it won’t be “severe”. This is a vague standard.
In other words, having told people who are self-diagnosing their own need for hospital treatment that they definitely won’t need it, the authorities declare victory when those people don’t go to hospital.
I’ve not yet seen any health authority take this into account or even recognize that such an effect could exist at all.
Let’s start from the hypothesis that the vaccinated get tested more often than the unvaccinated. And if we don’t assume that, then the vaccine surveillance report raw comparisons can’t be far off the mark in terms of relative positives tests.
So let’s for the purpose of argument start from the assumption that the vaccinated get tested more often than the unvaccinated. In that case we can also imagine that the unvaccinated generally have a tendency not to get tested unless they’ve got a pretty severe cough, flu etc (we see that in the comments here sometimes when people talk about getting tested). The vaccinated may generally get tested if they sneezed once (OK I exaggerate but you get the point).
Now someone having trivial symptoms when they test is less likely to test positive than someone who has major symptoms.
Then if the control is to compare people who test who have any symptoms whatsoever (regardless of severity) then we create a bias because the unvaccinated symptomatic who get tested on average have worse symptoms. And so the tendency of the unvaccinated to only test when they have severe symptoms increases their chances of testing positive. This gets mis-allocated as vaccine efficacy instead.
And the worst cold ever issue is also a problem.
In fact there are all sorts of multiple issues with this supposed control.
So unless you do checks with asymptomatic also, and there can be issues with that comparison too, you have a very one sided analysis. At least by doing both you retain some objectivity.
Multivariate analyses can have issues too of course.
No study is perfect. But when you take one thing that makes a study less perfect (such as the asymptomatic number being low in the Qatar study) and then ignore all the major flaws in the UKHSA study, all you do is to demonstrate your own bias.
We all have our biases of course but it’s how we minimise those biases that matters.
Does the number of times someone gets tested figure into this debate?
It was established fairly early on that a negative test could not exclude infection, particularly in those who at that time were asymptomatic (one of the reasons for all the hysterical measures, the asymptomatic were supposedly spreading the lurgi like Typhoid Mary before they showed any symptoms).
Hasn’t it been said on various occasions that there is an optimal time for testing, x number of days after symptoms appear to get the most reliable results? Test too early and you get a negative, test a few days later and it’s positive?
I’m thinking of the recent case of Biden’s WH mouthpiece Psaki, double vaxxed, who got tested after there were positive tests in her household. It was said that she tested negative 4 days running, then positive on the 5th day. She is close to the old and infirm POTUS and therefore probably gets tested often. How likely is it that the average double-vaxxed will keep retesting after a negative test?
Naturally the same applies to an unvaxxed, but as you point out, an unvaxxed with serious symptoms is more likely to test, I therefore assume also more likely to retest if symptoms don’t resolve.
Let me put it that way, an intervention which is claimed to have 90%+ efficacy (in terms of avoiding undesirable events, i.e. ICU ward hospitalization), does not need statistics to analyze. It just needs looking at who is occupying beds in ICU wards.
Just like you don’t need intricate statistics to figure out that it hurts a lot when you get hit with a hammer in the head. Having a hammer and a head at your disposal is just enough.
About 17% of covid positive deaths in English hospitals are in the unvaccinated (source UKHSA vaccine surveillance reports).
And slightly less than one third of emergency care positive test admissions are in the unvaccinated (source UKHSA vaccine surveillance report).
Perhaps it is about 17% unvaccinated filling ICU awards if we assume equal chance of death once in ICU. So for every unvaccinated person on ICU with a positive test about 4 vaccinated with a positive test for SARS-C0V-2.
It’s the vaccinated who are predominently occupying the ICU wards.
Not the case in Germany. And you also need to consider the waning efficacy of those vaccines – those “vaccinated filling ICU wards in UK” are people whose vaccines have been done more than 6 months ago and stopped protecting them. If anything, it does not show that the vaccinated are dying, it’s showing that they are not vaccinated enough.
So, when all the lovely efficacy data was proclaimed for the jabbed, did you reply something like :
“Ah bu you also need to consider the waning efficacy of those vaccines – those “vaccinated will be filling ICU wards in the UK before too long” because they are people whose vaccines after 6 months will stop protecting them. It will eventually show that the vaccinated are dying, and that they are not vaccinated enough.”
Did you?
“with” Covid. Or FROM Covid. If the former, then meh…
Are you sure there is no bias in ICU admission policy?
Do the jabbed get admitted more readily to ICU then the unjabbed?
If yes or no, how do you know?
It seem to me from the amount of different possible biases being discussed, then it is impossible to interpret any data effectively and entirely possible to use any data for whatever argument suits us.
“The size of the vaccinated asymptomatic cohort in the later months in the Qatar study is tiny, leading to such massive confidence intervals it is almost meaningless”
Not wishing to be a Statistics bullshitter ( but knowing precisely how easy it is manipulate “data” to produce the “right” result, and then cover your tracks ) , I take this to mean the numbers in the cohort were too small to derive meaningful conclusions other than ” the numbers are too small to be a representative sample”.
Enlighten me and everyone else what were the exact numbers for each cohort of the original Pfizer Biontech trials run for the EUA application, and for good measure delineate each cohort categorised as to “type definition” ( not certain of the technical descriptor) -e.g. healthy/age group/covid recovered/gender/prior CV19 infected and not/pregnant women/anaphylasis compromised…..
Then confirm why, if so, that these drug trial cohorts were of a sufficiently significant size for the trial results to be statistically meaningful and therefore to be accepted for the EUA to be granted, a result with which you appear to be entirely content.
Is it possible that there is a – non mathematical, naturally – correlation between the cohort data in the Qatar survey upon which you pour scorn – “tiny….almost meaningless”, and the extremely low numbers ( sorry, given the game away now ) in the Pfizer jab trials which you strangely do not deem to be similarly “tiny” and “almost meaningless”. Is that not a Balls Out, Stone Cold, Nailed On example of the confirmation bias you exhibit in your unstinting support for the gene editing therapies and their efficacy that you deem “vaccines”?
Just so you know, I am not responding to your comments because you keep asking me to do all the work. If you think the cohort numbers were too low for the Pfizer trials (and therefore the confidence intervals too wide) then say what they were and give the link.
No – YOU made the statement as I note above, just as you have done many times before when extolling the virtue of these gene editing therapies you call vaccines. You are very fond of asking for cited references but are less enthusiastic to provide the “information dense” references to bolster your evident confirmation bias.
You even attempted to cast doubt on the source by asking “where did it come from”, i.e how did Amanuensis get hold of it. What relevance is that?
As “Milo” pointed out some days ago, my request for you to provide an “information dense” to back up your opinion…..fell on deaf ears, and remained so 24 hours later.
I don’t think the Pfizer trials involved pitifully small numbers in totally unrepresentative cohorts, not qualified to comment – but when properly qualified medics such as Drs Fleming/McCullough/Cole/Malone do point this out I am inclined to believe them. From watching and listening these medics and others, I have seen tables which number the Pfizer Biontech EUA trials cohort in the low hundreds – in you expert opinion is that a statistically relevant number on which to base the decision to inject billions with a preparation the full contents of which remain unknown, which has have evident serious side effects ( which you have deemed to be small or tiny, correct me if I am wrong) the long term effects of which are unknown, the delivery mechanism of which is acknowledged – by the manufacturer – to have adverse effects itself.
I ask again, show DS readers exactly the nature of the cohorts used in the Pfizer Biontech trial, and how they were categorised between different groups of people……good luck with that. Dr Mike Yeadon struggled with that but may be you know better than he.
If the Qatar study cohort involves, in your opinion numbers, that are “tiny”, it is very strange you do not extend that logic to the trials for a jab you deem to be …a vaccine ( when the manufacturer states otherwise ).
I try damned hard to avoid making value judgements about matters I am not qualified to do so – you seem to not be bothered about that, given your statements to the effect that these jabs “work” – when they appear from multiple sources of data world wide not to do so; and then you make egregious statements about these jabs and anaphylaxis which were complete ignorant rubbish – and I DO know about that.
Perhaps you reckon there is no “proof” of the efficacy of early treatment drugs such as Ivermectin….be good to get your view about that…
You are very fond of asking for cited references but are less enthusiastic to provide the “information dense” references to bolster your evident confirmation bias.
There is a difference between producing references to support my case (which I am prepared to do) and being required to find the answer to a question you have asked.
Excellent analysis of the problems of conducting studies, and the mess you get into by trying to short-circuit the process.
Let’s have a go at some simplistic statements that have also been staring us in the face :
(1) “Oh. Sorry. Those data are not available… The usual problem.”
The foundational problem. Before starting out on the journey, we need some assurance that the ruler isn’t bent, and that our basic assumptions about the data are correct. We don’t even cross the starting line here, given the definitional questions, driven by the anti-medical need for panic generation.
(2) “the initial clinical trials were time limited for understandable reasons”
Understandable? Mmmmm. But time-limited to an extent that was bound to invalidate any purported assurances on efficacy and safety. Simply : the testing cannot, by definition, be done satisfactorily in that sort of timescale (you can’t turn months into years) – particularly when the results of initial trials have thrown up – not assurance – but simple analytical questions about the absolute risk reduction. Such an approach isn’t just mistaken – it’s dishonest.
By December 2020, the ‘reasons’ (for speed) were far from ‘understandable’. It was clear by then that the investment was blown on an unnecessary bet.
The one insight that is indisputably valid in this analytical mess and short timescale, is that the vaccine shows no offer of significant population immunity on an observational basis, such as would be necessary for ’emergency’ authorization (particularly if the ’emergency’ doesn’t exist).
… and we can forget all the smoke about the snake oil never pretending to immunity and curtailment of transmission. It was indisputably rationalized on that basis.
Remember – the indisputable assurance of essential and justified use has to come from the protagonists, not the questioners. It does not exist when all considerations lack supporting evidence. It’s an ‘unless’ situation, not a sloppy ‘‘let’s give it a go – whatever‘.
Even on these simple grounds, we are obviously into misinformation and deception about ‘efficacy’ before we get to detailed analysis.
Very well said!
The obvious failure of the gene therapies, and worse, their possible worsening of not only individuals’ health but also the pandemic, is now so obvious that the regime must dedicate itself around the clock to avoiding charges of crimes against humanity. I would expect UKHSA to stop publishing these data, I would also expect much heavier censorship and an even more insane drive to destroy the control group with much heavier mandates. They must be stopped. They must be arrested and charged and they must face trial.
While the injections are likely reducing death in susceptible groups, all cause mortality among the injected is higher. This means they are killing more people than they are helping to stay alive, and very often young and healthy people including children. The regime knows this, and its knowledge of it is what makes it guilty of these crimes. This is a very serious business.
There are occasional outbreaks of sanity H.
I’m just starting to grok/absorb the contents of a Swiss bunch.
I haven’t seen much about them on LS/DS….
“ALETHEIA – Medicine and Science for Proportionality”
was founded in summer 2020 by 6 practicing primary care providers who have been treating patients every day in their practices for years, as well as a scientific-pharmaceutical advisor, with the aim of networking doctors in order to to obtain a differentiated and empirically and scientifically based view of current health issues.
the above blurb was translated from their website, they are openly “differentiated”
Founding members / active working group Aletheia:
Fabien Balli-Frantz, MSc. ETH Elec. & Pharmacy Student, Biel
Dr. med. Urs Guthauser, Bern
Dr. med. Andreas Heisler, Ebikon
Dr. Werner Michael Heller, Schüpfheim
Dr. Sc. Nat. ETH Barbara Müller, Ettenhausen
Dr. med. Björn Riggenbach, Neuchâtel
Dr. med. Rainer Schregel, Wattwil
Dr. med. Dieter Thommen, Thun
Dr. med. Ruke Wyler, Bern
they also have openly/publicly signed up >500 scientists & doctors, several thousand health professionals, and many thousands of other serious supporters
Now they are working – proselytising actualité & facts in preparation for a late November Swiss referendum on ‘emergency’ changes to the Helvetic constitution – if I’ve understood correctly
<blockquote class=”imgur-embed-pub” lang=”en” data-id=”a/Ah73I5f” ><a href=”//imgur.com/a/Ah73I5f”>UK Covif Inquiry and Deloittes – Private Eye No 1560 12 Nov 2021 page 9</a></blockquote><script async src=”//s.imgur.com/min/embed.js” charset=”utf-8″></script>
https://imgur.com/Ah73I5f
<a href=”https://imgur.com/Ah73I5f”><img src=”https://i.imgur.com/Ah73I5f.jpg” title=”source: imgur.com” /></a>
UK Covid Inquiry and Deloittes – Private Eye No 1560 12 Nov 2021 page 9
https://imgur.com/Ah73I5f
Really excellent article and very clear explanations of the methodology too. Thanks very much. Need to read it carefully when I’ve got more time before commenting.
Thank you, Amanuensis, for sharing your knowledge with us, not just in this article, but below the line.
I am not scientifically skilled, either through education or insight.
But I do believe in looking at what is right in front of my eyes.
Someone made a comment in the Jerusalem Post that got me thinking, so I just did a little check myself, using numbers from Worldometer.
12 November 2020, Israel noted 2706 corona deaths.
12 November 2021, Israel noted 8140 corona deaths.
Israel started vaxxing 19 December 2020, when the corona death rate was 3074.
So in the 11 months since vaxxing started, Israel has had 5066 more corona deaths, some 60% more than it had prior to vaxxing. To say this is accounted for by the unvaxxed seems bizarre, as prior to December 2020, everyone was unvaxxed. Why would the number of deaths be higher if the number of unvaxxed is so much smaller?
On 2 August 2021 the number of corona deaths was 6487. Israel started giving the 3rd booster on 1 August. Corona deaths over the 3 months between 2 August 2021 and 12 November 2021 are 1653, which does not seem a very favourable comparison with the 2706 deaths ticked up over the 9-month period from March 2020 to December 2020 prior to the vaxx.
Naturally the vaxx argument will be that the vaxx was not given in time to provide protection before the 2021 winter wave, that the booster shot was given after the Delta wave had taken hold and before it was realised that effectiveness waned, that unvaxxed have died. To the best of my knowledge, there is no figure given for the precise number of vaxxed/unvaxxed who are noted as corona deaths since the vaxx roll-out.
Just looking at these numbers, I fail to see any efficacy at all where it counts, i.e. mortality The so-called efficacy of the vaxx in keeping people out of hospital and alive seems to be more based on the fact that millions of experts, doctors and media repeat that phrase a gazillion times a day – but the reality does not seem to align. Repeat a lie often enough…
https://www.covid-datascience.com/post/what-do-new-israeli-data-say-about-effect-of-vaccines-boosters-vs-death-critical-severe-disease
https://www.bbc.co.uk/news/uk-59273273
this story makes my blood boil
This person should either write letters to the big national newspapers stating this (in layman’s terms) and/or try to get their article published (again, in more layman’s terms than the above so it can be understood by Joe Normie [who likely won’t understand much of the above]) in one of them.
I still strongly suspect that the ‘vaccines’ were always designed to be short term sticking plasters by the pharmacutical giants as it means repeat business and huge profits, mandated by government.
Why stop an epidemic in its tracks when you can keep it going for years, even decades and milk the public for every £ or $ they have and control them at the same time, making huge amounts of money for your other corporate buddies and giving so much power to you, them and their government/civil service/media cronies?
Because if your competitor happens to develop a vaccine which sucks less, you will be out of business (as evidenced by what happened to AstraZeneca vs. mRNA)
Governments main reasons for promoting the experimental jabs are to reduce hospitalisations. It would be interesting to see an unbiased study on how effective the experimental jabs are at reducing hospitalisations compared to the unjabbed.
Vaccine Effectiveness against infection is interesting but as it dramatically reduces after a few months governments propaganda is focused on reducing hospitalisations and not so much the jabs effectiveness against infection.
“Governments main reasons for promoting the experimental jabs are to reduce hospitalisations”
Are they? I doubt they give two hoots about what the jabs do in reality. Their main reasons for promoting anything are always political – how does it look to the voters, to other countries, does it increase or consolidate our power, cover our Big Lie?
“It would be interesting to see an unbiased study”
Good luck with that. Maybe in 50 years time.
“governments propaganda is focused on reducing hospitalisations and not so much the jabs effectiveness against infection”
Except that the logic of vaxx passports is that the vaxx reduces infection
I quite agree but in September 2021 the government stated ……
“The latest estimates indicate that the vaccination programme has directly averted over 230,800 hospitalisations. Analysis on the direct and indirect impact of the vaccination programme on infections and mortality, suggests the vaccination programme has prevented between 23.7 and 24.1 million infections and between 119,500 and 126,800 deaths.” https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1019992/Vaccine_surveillance_report_-_week_38.pdf
I would like to see Amanuensis or anyone else do an unbiased study on these wild government claims of 230,800 hospitalisations and 126,800 deaths averted.
I suspect that this would be as difficult to prove as those double jabbed who’ve “tested” positive for Covid saying “Ah but I would have been a lot worse without the jabs”
Precisely.
I’m arguing that exact point with someone.
They’ve convinced themselves they would have been a lot worse mainly because the government keeps telling everyone they would be a lot worse.
I believe it’s the exact opposite, it is the experimental jab which is causing people to catch Covid and to be hospitalised let alone the deaths and injuries the jab causes.
A detailed rebuttal of the governments claims of 230,800 hospitalisations and 126,800 deaths averted is much needed.
I tell people who say that to me that they are comparing apples with pears. This year we have been dealing with the Delta variant, a much more virulent but a far less dangerous variant than the original. The jabs are trying to fight this year’s war with last year’s weapons.
Well they may well have said that and some people involved in the process might even believe it.
If you believe that rubbish you are visiting the wrong site.
I don’t, that’s why I said they were “wild” claims.
Doctor Jones’ analysis here is a splendid example for the fallacy “something could be going wrong; therefore it is going wrong” – on which pretty much every conspiracy theory in existence is built. It is not enough to mass-produce hypotheses, Doctor Jones, in fact this is only where science begins.
Then you have to do the hard work of testing your theories (which you won’t do for lack of resources). But of course, this “subtlety” will be lost on your readers, and so you can publish another triumphantly inquisitive article a few weeks down the line.
But as a matter of fact, given your target audience and purpose of these communications, you could even spare yourself the cherry-picking efforts and just fill your articles with some sciencey-sounding gibberish (as many of the anti-vaxx “experts” tend to do). So I guess you deserve some points for at least not doing that.
You’ve made some silly comments on here but that is up there.
He’s cited other studies which diverge from the UK reports and ponders why. He’s landed on some excellent methodological points.
You’ve read this as the writer presenting this as proof of willfull attempt to massage the numbers. He’s done nothing of the sort, that’s you projecting your general view of the readership onto this. How is he cherry picking things?
And if this is some sort of deceptive piece, and the UKHSA is correct, what are they doing in Qatar? Cherry picking to made vaccines look bad?
Oh yes, he’s done something of the sort, namely dug up a single study which appears to confirm his prior assumptions, while blissfully ignoring all others.
As do government sponsored propaganda experts, ICL SAGE modellers, assorted Big Pharma shills and whole phalanx of woefully unqualified ministers (with an honourable mention to Mr Javid for gibberish above and beyond). So your point is what, exactly?
Yes, pretty much so. Non sequitur.
The article was written by Amanuensis, not Will Jones, as you might have noticed had you actually read it.
At the bottom it says “By Will Jones” because he posted it for Amanuensis.
It’s enough I’ve noticed who is posting the same sort of article over and over again. That he is now copying someone else’s (anonymous) work to confirm his viewpoint does not exactly exonerate him.
Bwaaahaahaa, oh dear Doh! etc etc.
Think Rayc has an agenda he’s desperate to push?
rayc – you are going to develop serious piles with the straining required to produce this amount of shit!
Great analysis and great discussion
There must be some reason why the world lost their collective minds and locked down.
don’t forget healthy people caught Covid and died, Johnson was hospitalised by it. Governments the world over did the same collective actions.
covid 19 is not a myth, I think the conspiracy is still to be unearthed. China are still heavily locking down when a few people blow there nose & I suspect they know far more about this thing than anyone is letting on.
it’s important to ensure the science and statistics stands up to scrutiny, comprehension then needs attributing to the results.
government actions from China to the North Americans does not align to the statistics. I think that was obvious from the start.
I think the question is why take such actions when the data never supported it and those making the decisions and doing the calculations knew the data would not support it.
there must be something else to Covid that is not widely known that causes nations like China to lockdown because of a sore throat.
What bothers me is that we used to think, when it suited us, that the case numbers generated by the PCR test was a load of bollocks.
And I still do.
And now some of us have moved the goal posts, when it suits us, to put forward the idea of the falling effectiveness of the covid “vaccines” based on the now infallible PCR test?
Correlation is causation is the graveyard of bad science; even worse is correlation, involving a crap test, is causation.
Sometimes it is.
Next?
“….many behavioural effects in the vaccinated compared with unvaccinated groups…..”
The immediate problem of whether the only difference between the ‘population’ of unvaccinated and the ‘population’ of the vaccinated is whether or not they are vaccinated?
Have the unvaccinated been getting out and about as much as possible?
Have a better exercised immune system?
Have the more widely read unvaccinated been pill popping vitamin D and zinc for sometime and never felt better since; like me?
And are they being less affected now by other microbial infections that have picked up strands of covid 19 genetic code that produce PCR postives tests?
My concern over PCR testing is cross reactivity and the really, really interesting, recent and growing subject of gene transfer/exchange between microbes.
I had been following that before all this started.
Eg
[…………………
https://phys.org/news/2010-10-horizontal-gene-microbes-frequent-previoulsy.html
https://en.wikipedia.org/wiki/Horizontal_gene_transfer
https://journals.asm.org/doi/10.1128/JVI.00955-10
https://www.nature.com/articles/srep26934
https://journals.asm.org/doi/10.1128/JVI.00955-10
…………………..]
Thus the potential for the very tiny fragments of the “genes” used to identify covid 19 being incorporated into the millions of unidentified [RNA] based virus’s and god alone knows what else.
Here’s a pre-covid article on the mRNA technology.
https://www.statnews.com/2016/09/13/moderna-therapeutics-biotech-mrna/
Some quotes showing that this technology isn’t safe for ongoing dosing:
Delivery — actually getting RNA into cells — has long bedeviled the whole field. On their own, RNA molecules have a hard time reaching their targets.They work better if they’re wrapped up in a delivery mechanism, such as nanoparticles made of lipids. But those nanoparticles can lead to dangerous side effects, especially if a patient has to take repeated doses over months or years.
Moderna’s most advanced competitors, CureVac and BioNTech, have acknowledged the same challenge with mRNA. Each is principally focused on vaccines for infectious disease and cancer, which the companies believe can be attacked with just a few doses of mRNA.
“I would say that mRNA is better suited for diseases where treatment for short duration is sufficiently curative, so the toxicities caused by delivery materials are less likely to occur,” said Katalin Karikó, a pioneer in the field who serves as a vice president at BioNTech.
Amenuensis has provided an excellent and highly-credible analysis. However, the chances that the UKSA will act upon it are zero.
Why? Because the pseudo-pandemic is a smoke and mirrors operation built on a lie and sustained only by a litany of lies, half truths, evasion and obfuscation.
Thankfully, largely due to a relative but influential handful of distinguished dissident voices on alternative media platforms (soon to be silenced via the egregious Online Safety Bill), the propagandised public is starting to wake up to what the “COVID crisis” is truly about – power and money.
https://rumble.com/vlwbgv-the-real-reason-behind-everything..html
https://www.bitchute.com/video/IQoUmvcoiStX/
Is it any wonder that the Governments/pharma are so keen to eliminate anything resembling a control group in the population?
The ongoing COVID-19 nonsense here in the United States exists solely and exclusively because our governments have failed to use the correct treatment. They used so-called “vaccines” when Japan has just proven, in less than ONE MONTH, that Ivermectin can wipe out the disease. IVM was awarded the Nobel prize for medicine in 2015. One of the 3 most important drugs in human history: Aspirin, Penicillin, and Ivermectin. Get your Ivermectin today while you still can! https://ivmpharmacy.com
Many thanks for an excellent article. Crystal clear and understandable. Well done.
Covid Crusher: Mix one heaped teaspoon of Iodine table or sea salt in a mug of warm clean water, cup a hand and sniff or snort the entire mugful up your nose, spitting out anything which comes down into your mouth. If sore, then you have a virus, so continue morning noon and night, or more often if you want, until the soreness goes away (2-3 minutes) then blow out your nose and flush away, washing your hands afterwards, until when you do my simple cure, you don’t have any soreness at all, when you flush – job done. Also swallow a couple of mouthfuls of salt water and if you have burning in your lungs, salt killing virus and pneumonia there too.
My simple salt water cure, kills all Coronaviruses and viruses, as soon as you think you have an infection, or while self isolating, before the viruses mutate into the disease in your head and body, for which there is no cure.
Richard