
The latest Technical Briefing on the variants of concern, number 22, has been published by Public Health England (PHE), so we can update our (unadjusted) estimates of vaccine effectiveness against the Delta variant using the data it includes from sequenced Delta samples from positive PCR test results in England.
As before, we subtract the figures in briefing 22 from those in briefing 17 to give the figures for the period June 22nd to August 29th. We also use figures for proportions of the population vaccinated by age derived from the PHE Covid surveillance reports.
Starting with the over-50s, for the period June 22nd to August 29th, PHE reports 47,874 Delta infections in the double vaccinated and 5,748 in the unvaccinated. PHE figures show that in this period the proportion of the over-50s double vaccinated increased from 87% to 89%, giving a mean of 88%, and the proportion unvaccinated was stable at 9% (Note: not 10% as I stated previously). Calculating the vaccine effectiveness against Delta infection in the over-50s (1-(47,874/88%)/(5,748/9%)) gives a figure of 15%. This is the same as the figure I calculated two weeks ago, though now using the more accurate figure of 9% rather than 10% for the proportion unvaccinated. This means that it represents a decline (using 9% for the previous calculation would give a VE of 24%). This continues to be very different to the estimate in the recent Oxford University study using ONS survey data, a study which I criticised for numerous inconsistent and implausible findings.
With regard to deaths with Covid (within 28 days of a positive test), PHE reports 1,004 in the double vaccinated and 399 in the unvaccinated in the over-50s in this period. This works out (1-(1,004/88%)/(399/9%)) at a vaccine effectiveness against death of 74%, down slightly from 75% using data from the previous briefing (even with the change to 9% unvaccinated). This is a 74% reduction in mortality including any reduced risk of infection, not in addition to it. It continues to be an encouraging figure, albeit lower than earlier studies have suggested, and dropping week on week.
For the under-50s, for the period June 22nd to August 29th, PHE reports 58,714 Delta infections in the double vaccinated and 160,143 in the unvaccinated. PHE figures show that in this period the proportion of under-50s double vaccinated increased from 18% to 39%, giving a mean of 28%, and the proportion unvaccinated decreased from 61% to 51%, giving a mean of 56%. Calculating the vaccine effectiveness against Delta infection in the under-50s (1-(58,714/28%)/(160,143/56%)) gives a figure of 27%. This is down from 37% two weeks ago, and though higher than in the over-50s, is still very low and much lower than earlier studies (including the trial) indicated.
For deaths, PHE reports 37 in the double vaccinated and 93 in the unvaccinated in the under-50s in this period. This works out (1-(37/28%)/(93/56%)) at a vaccine effectiveness against death of 20%. This is up from 12% two weeks ago, but is still very low and much lower than in the over-50s. This may be because higher risk people are prioritised for vaccination, or are more likely to consent to it, in the younger age groups.
These figures are much lower than those commonly quoted and used in modelling, and if they are closer to the truth then they mean the official, self-congratulatory estimates of “100,000 deaths” and “24.4 million infections” prevented by the vaccines are huge overestimates.
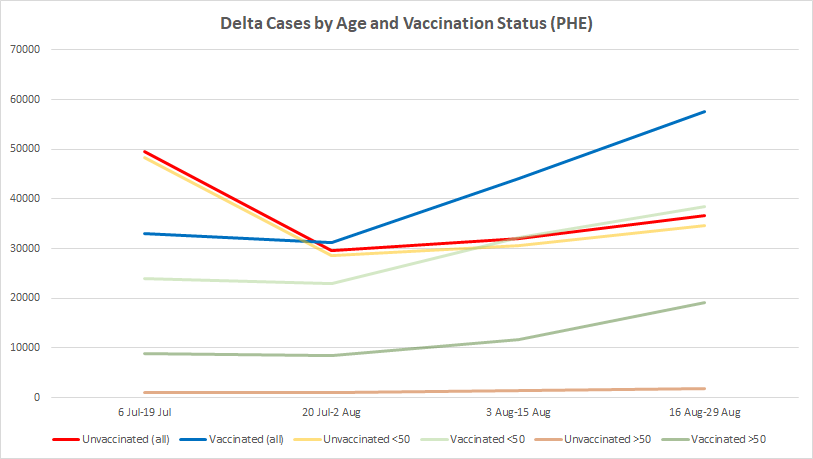
By plotting the differences between the reported total Delta cases in the last four briefings we can also get a picture of how they are changing over time in the different age and vaccine-status cohorts. The red and yellow lines in the chart below show that new Delta infections in the unvaccinated have started to increase again, but not by as much as those in the vaccinated (for this purpose, all who are at least 21 days after their first dose), which have continued to surge. A majority of new infections (57,565 out of 94,148, or 61%) are now in the vaccinated. This means that the recent increase in reported infections in England is being driven primarily by infections in the vaccinated. The fainter lines show the trends in the over- and under-50s, indicating that in both age cohorts new Delta infections in the vaccinated now outnumber those in the unvaccinated, and that new infections in the vaccinated over-50s are increasing particularly fast. This helps to explain the declining vaccine effectiveness estimates given above.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.