
One of the claims put forward by the authors of The Great Barrington Declaration is that lockdowns unfairly shifted the burden of COVID-19 onto the working class. As Martin Kulldorff and Sunetra Gupta argued in a piece for the Toronto Sun last November:
Low-risk college students and young professionals are protected; such as lawyers, government employees, journalists, and scientists who can work from home; while older high-risk working-class people must work, risking their lives generating the population immunity that will eventually help protect everyone.
The same idea was captured in a viral tweet by the art critic J.J. Charlesworth:
To evaluate this claim, let’s begin by looking at some of the data from Britain. Last July, the ONS attempted to quantify the extent to which different jobs can be done from home. Unsurprisingly, they found that higher-paying jobs in the professional and managerial classes are much easier to do from home, whereas lower-paying jobs in the skilled and unskilled working class are much harder to do from home. (‘Front-line doctor’ is an exception.)
While “key workers” are drawn from all income deciles, a relatively large percentage are drawn from the 2nd, 3rd and 4th deciles – particularly in the food and necessary goods sector. And according to the ONS, 15% of such workers were at an increased risk of COVID-19 because of a pre-existing health condition.
In January of 2021, the ONS computed age-standardised mortality rates for COVID-19 in different occupations. They found that men in professional and managerial occupations were substantially less likely to die of COVID-19 than those in service and elementary occupations:
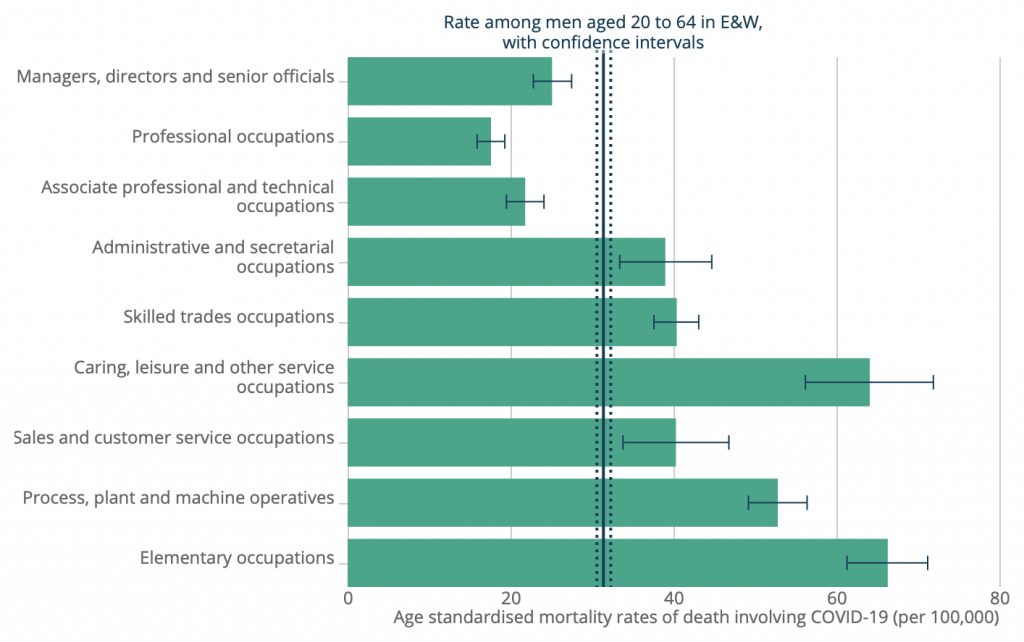
The pattern among women was similar, although somewhat less pronounced. (The highest age-standardised mortality rate was for women working as plant or machine operators.)
In a study published in Nature, Elizabeth Williamson and colleagues analysed data on a large sample of British adults, and found that individuals from the bottom quintile for area deprivation were significantly more likely to die of COVID-19, even after controlling for age, sex, ethnicity and a number of pre-existing health conditions. This may be because such individuals had greater exposure to the virus, although there are other possible explanations.
It’s important to note that men in elementary occupations and skilled trades are more likely to die for any reason than men in professional and managerial occupations. In other words, there is a mortality gradient across occupations for all-cause mortality, as well as for COVID-19. This means that the two gradients may be partly caused by the same factors – such as more men in working class occupations having pre-existing health conditions.
Furthermore, the fact that people in working class occupations were more likely to die of COVID-19 does not, by itself, prove that lockdown shifted the burden of COVID-19 onto the working class. Such people might have been more likely to die of COVID-19 even in the absence of lockdown – say, because they were less able to engage in voluntary social-distancing.
In order to evaluate the claim that lockdown shifted the burden of COVID-19 onto the working class, we need to compare countries or states that did lock down with those that did not. Of course, the only major country in Western Europe that did not lockdown is Sweden.
In an unpublished paper, Sunnee Billingsley and colleagues analysed Swedish data, and found that workers in frontline occupations were not more likely to die of COVID-19 when adjusting for individual characteristics. Their findings indicate “no strong inequalities according to these occupational differences in Sweden and potentially other contexts that use a similar approach to managing COVID-19”. This supports the Great Barrington Declaration authors’ claim.
Another way of testing the claim that lockdown shifted the burden of COVID-19 onto the working class is by comparing infection rates across social classes before and after lockdown.
In a study published in BMC Public Health, Nathalie Bajos and colleagues analysed French data, and found that individuals in the highest social class saw a substantial decline in the risk of infection after the country went into lockdown, whereas individuals in the lowest social class saw a much smaller decline. Though it’s possible these differences emerged due to voluntary changes in behaviour that happened to coincide with the start of the lockdown.
Overall, there is tentative evidence that lockdown did shift the burden of COVID-19 onto the working class. However, comparative studies will be needed to investigate this claim more systematically.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
“Activist groups will now wield the power to complain on behalf of others”
I wonder how much success a conservative/right wing/non woke “activist group” would have in complaining on behalf of, for example, a lockdown sceptic who had been accused of being a granny killer for not following rules, being an anti-vaxxer etc.
Clarkson, I believe, made the fatal error of issuing a grovelling apology to the MMthus playing right into the hands of the activists. Presumably his fear of being cancelled trumped upholding principle.
This may both encourage activist groups to continue lodging//pursuing complaints to IPSO and emboldens the politicised IPSO to arrive at their ruling of upholding the complaint.
Piers Morgan did at least refuse to apologise to MM.
Never apologise, never explain.
IPSO effectively supported the COVID narrative. They are not independent.
yes I made several complaints to IPSO that the disgraceful series of articles in the MSM in early 2022 reminiscent of how things started in Germany that those refusing the jab were idiots, unclean,should not be allowed in hospitals, on public transport, made to suffer etc; offended the code as being discriminatory,harassing and inaccurate. IPSO rejected all complaints which it justified on the basis of a very strict legalistic interpretation of its rules
The veneer of civilization is waffer thin and is peeling away faster than a ginger with sunburn.
Oi..!
https://www.farminguk.com/news/natural-england-gives-sssi-status-to-penwith-moors-amid-farmer-concern_62886.html
A very worrying development. Land which has been effectively managed by local farmers for centuries will now be “locked up.” The attacks on farms and farmers will definitely intensify.
Interesting that the area is of value to wildlife after thousands of years of farmers managing it, so their solution is to stop the farmers managing it? A very similar thing is happening in Western Australia. Under the guise of protecting Aboriginal Cultural Heritage new legislation was passed which requires anyone who owns land greater than 1100 square meters to seek an assessment and approval prior to undertaking any disturbance in case they disturb potential cultural heritage sites.
Good points. Thanks.
Ipso, the press regulator…
I am absolutely fed up to the back teeth with ‘regulators’…
Regulators curtailing free speech, regulators facilitating the promotion of highly questionable medical products such as the Covid vaccines…
We’re awash with ‘regulation’ which is not working for the people.
Whose best interests are being served by this overbearing regulation?
I do not consent!
Hear, hear.
The only interests served are those of the serially incompetent who can’t get a job in the commercial world so end up as a ‘regulator’ sticking their noses in others’ business.
I see that the Financial Times, The Independent and The Guardian have opted out of IPSO. Perhaps it’s time the other papers did too.
I believe the chances of Jeremy Clarkson writing for any of the above publications is on the far side of remote.
True. But irrelevant!
Actually it is not irrelevant as it very neatly points out the bias of the named publications and of IPSOS.
above I have referred to my complaints being rejected by IPSO. At least I was able to complain about articles inTelegraph, Mirror, Express and Mail but I remeber could not do so for one in Evening Standard as not a member. So despite all its faults I am even more suspicious of those papers who are not members of IPSO.
Agreed. The use of the expression “going forward” at the end of the second sentence is incomprehensible, however.