
The Telegraph‘s front page led today with the story that nearly a quarter of deaths (23%) registered “with Covid” in the latest official data for England and Wales were not “due to Covid” but were due to another underlying cause, according to the information entered on the death certificate. This percentage is up on earlier figures. The same figure for the original wave up to August 31st in England and Wales was just 8% (4,159 out of 52,327).
However, there is good reason to think both figures are too low. A Freedom of Information enquiry (pictured below) found that for Northern Ireland, the proportion of deaths that mentioned Covid but identified an antecedent condition (or conditions) as the cause of death for the period March 1st to November 20th was 38% (494 out of 1,301).
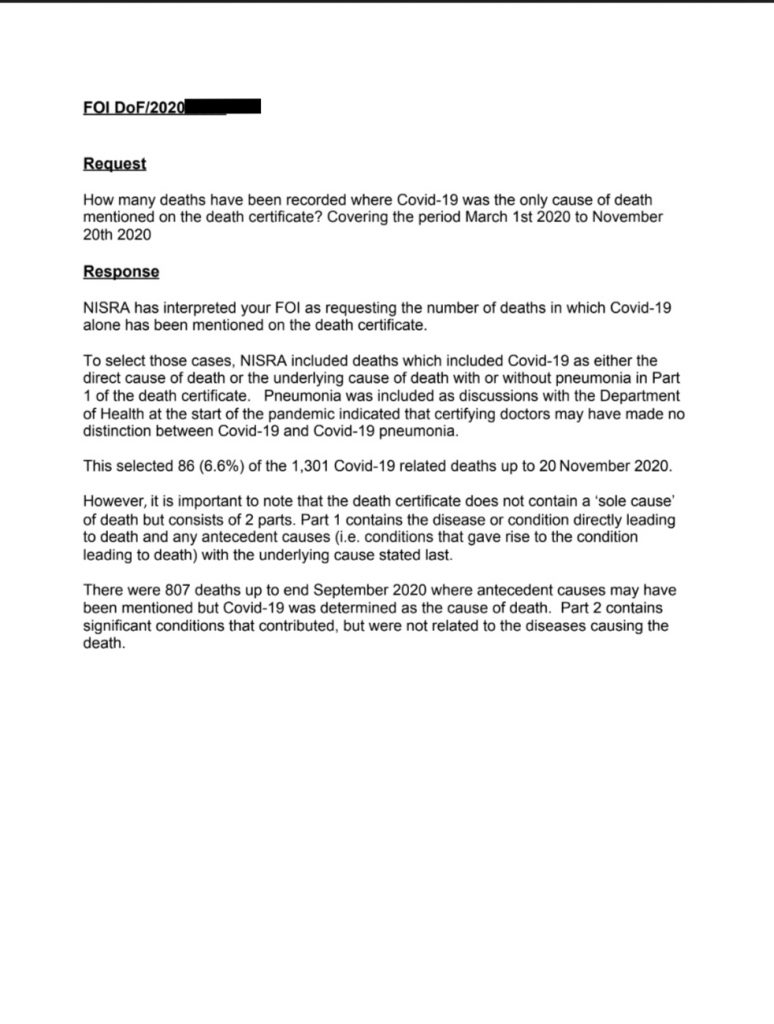
Why would Covid be the underlying cause of 62% of Covid deaths in Northern Ireland but 92% in England and Wales for broadly the same period? It wouldn’t, of course. The difference is how the deaths are recorded.
One reason may be because doctors in England and Wales were given a stronger steer to record Covid as the underlying cause of death. The British Medical Association told doctors early in the pandemic:
In those cases where the doctor is confident on medical grounds that a particular cause of death is likely then that should be entered on the MCCD [death certificate]. COVID-19 is an acceptable direct or underlying cause of death for the purposes of completing the MCCD, even without the results of a positive test, and it is important that likely COVID-19 deaths are reported as such via the registrar.
No similar guidance appears to exist for Northern Ireland.
Even 38% may be too low, however. A review by a county in Sweden in August found that 85% of the 122 Covid deaths investigated were due to a different underlying cause.
The Östergötland region has examined all deaths that have died at home or in special housing with confirmed COVID-19. Records from 122 people have been reviewed, which is 51% of the 240 people who had died in the county when the review was done.
The cause of death in the cause of death certificate has been COVID-19, but the review shows that other diseases may have contributed or been the decisive cause of death – for example, heart disease, lung disease or dementia.
111 of the deceased outside the hospital had extensive comorbidity and 11 moderate comorbidity. Half were 88 years or older.
COVID-19 was estimated to be the direct cause of death in 15% of deaths. For a majority of the deceased – as many as 70% – COVID-19 was a contributing factor rather than a direct cause. In 15%, the cause of death was judged to be other diseases, then most often heart disease.
The definition of a “Covid death” has been a consistent issue throughout the crisis, with the Government even knocking thousands of deaths off the running total in August after changing the definition following criticism. It has been frequently observed that different standards have been applied to Covid deaths than to other similar diseases – a frail elderly person who died with an acute respiratory condition such as influenza would not, prior to the pandemic, usually have had influenza recorded as the underlying cause of death, whereas Covid will often be recorded as such in similar circumstances. This novel practice has inflated the pandemic death toll and fed the narrative of fear.
Overall death totals (from all causes) are generally a much better guide to the impact of the pandemic – though even there deaths due to interventions become mixed up with the Covid deaths. Trying to get to the bottom of the true Covid death toll will not be an easy task at all.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Well done. A clear, analytical article.
I think (and it can only be that) that the Swedish figures are probably the closest estimate in this unholy and inexcusable mess that has been made of the data.
I would naturally assume the Swedish figures were closest to the truth because they didn’t lock down and had no need to scare their populations into complying.
I always assumed out of the 100,000 only a few thousand were real covid deaths. Even the 15% of Swedish ‘real’ covid deaths most are likely to be old age deaths brought forward a winter season or two
3 good articles here, all from the same author, but he does a good job, showing various elements of the enormous crimes that have been committed by HMG to engineer this situation, fiddling the figures, rigging the legal system and overturning established protocol for death registration to facilitate death certificate forgery and the corona fraud overall, all topped off with a healthy dose of psychological warfare to ensure compliance.
All of these things are discussed with good evidence and references provided.
COVID 19 – The UK Scamdemic – Part 2
https://in-this-together.com/covid-19-the-uk-scamdemic-part-2/
COVID 19 is a Statistical Nonsense
https://off-guardian.org/2020/05/05/covid-19-is-a-statistical-nonsense/
A Deceptive Construction – Why We Must Question The COVID 19 Mortality Statistics
https://www.ukcolumn.org/article/deceptive-construction-why-we-must-question-covid-19-mortality-statistics
Yes indeed, Iain has done a great job throughout this scam in getting to the bottom of issues. The last of the links I think is the nearest anyone has got to in identifying the correct number ‘of’ deaths. His thorough analysis puts most of the official stuff to shame.
He has also produced an excellent critique of the so-called vaccines trial results, explaining the difference between ‘relative’ and ‘absolute’ statistics.
Its very unlikely that over 15,000 people have died of/from covid in the UK.
If Iain and Ioannidis worked together I’m sure the recorded IFR would fall below 0.1% ie BELOW seasonal flu!
Yes he has been a great source of info, laying it out methodically, so the facts can speak for themselves.
Regarding the “vaccines which aren’t vaccines”, I read this article which has great detail about how they actually work and some of the very serious concerns about them which you might find interesting.
‘Healthy People Do Not Require Genetic Vaccination’
https://cassandravoices.com/science-environment/science/healthy-people-do-not-require-genetic-vaccination/
Plus Dolores Cahill testifies that she expects those who have had the gene-based mRNA vaccine to have a maximum of 5 to 10 years to live, even if they are in their thirties. 3 years for over 70s.
https://twitter.com/Teqmock/status/1380704775109545989
Thank you for that Marcus de Brun article. So informative.
https://cassandravoices.com/science-environment/science/healthy-people-do-not-require-genetic-vaccination/
How credible is this dying within 5 to 10 years? Everybody who has had the vaccine? Sorry I just don’t see that as a believable prediction. I’m sure some will suffer issues from it, maybe plenty will die, but everyone? Sorry I’m not buying it, and this from someone who will not have the vaccine, of any variety, himself.
I have no idea how credible it is but as far as I know Dolores is a genuine expert in this field so when she comes out and says something like that, it’s not something you can just ignore. It’s someone who has got the qualifications and done the research saying it, as opposed to someone who hasn’t. The link to teqmock on twitter https://twitter.com/Teqmock/status/1380704775109545989 contains a list of links about “Antibody Dependent Enhancement”, starting at the top with the Fauci clip. Go through the links and you will have more idea what this relates to. ADE is what this is about, I believe. Dolores was the first person to alert me to this issue and since then all I have found is that what she says is true. Hopefully she is wrong with this.
Here is a document which confirms ADE is real and is not being disclosed in a way which is ethical. This relates to the Covid19 vaccine trial subjects but because of the “Emergency Use Only” licences given to these experimental shots, half the country has now had this injected into their bodies, before the trials end in 2023, so they are all effectively vaccine trial subjects. Here is part of the text, the link has the rest:
Informed consent disclosure to vaccine trial subjects of risk of COVID‐19 vaccines worsening clinical disease
https://onlinelibrary.wiley.com/doi/full/10.1111/ijcp.13795
“Results of the study
COVID‐19 vaccines designed to elicit neutralising antibodies may sensitise vaccine recipients to more severe disease than if they were not vaccinated. Vaccines for SARS, MERS and RSV have never been approved, and the data generated in the development and testing of these vaccines suggest a serious mechanistic concern: that vaccines designed empirically using the traditional approach (consisting of the unmodified or minimally modified coronavirus viral spike to elicit neutralising antibodies), be they composed of protein, viral vector, DNA or RNA and irrespective of delivery method, may worsen COVID‐19 disease via antibody‐dependent enhancement (ADE). This risk is sufficiently obscured in clinical trial protocols and consent forms for ongoing COVID‐19 vaccine trials that adequate patient comprehension of this risk is unlikely to occur, obviating truly informed consent by subjects in these trials.
Conclusions drawn from the study and clinical implications
The specific and significant COVID‐19 risk of ADE should have been and should be prominently and independently disclosed to research subjects currently in vaccine trials, as well as those being recruited for the trials and future patients after vaccine approval, in order to meet the medical ethics standard of patient comprehension for informed consent.”
Dolores Cahill has credentials that are second to none, for example:
https://dolorescahill.com/pages/about
Dolores is an Inventor, Founder and Shareholder of Companies, has been Granted & licensed Patents in Europe, USA & worldwide with applications in improving the early accurate diagnosis of disease (auto immune diseases & cancer).
Click here to visit her University College Dublin School of Medicine public profile. Her latest business ventures include the World Freedom Alliance, FreedomAirway and Custodean.
With more than 20 years expertise in high-throughput protein & antibody array, proteomics technology development, automation & biomedical applications in biomarker discovery, diagnostics & personalised medicine
Selected experience as Expert in EU over past 15 years:
EU Future & Emerging technologies (FETOPEN) Innovation Launchpad; EU Innovation Radar Expert, EU Horizon 2020 Societal Challenges 1 (Health).
Holds several granted and licensed international patents (EU, USA, Japan, Australia) (1995-present) and peer reviewed publications, and reports,
Professor, University College Dublin (2005-present)
Group Leader, Max-Planck-Institute, Berlin, Germany (1995-2003)
Supervisor of completed PhD & Masters’ degree students in Germany and Ireland…….
This page continues with further information about her career, but you get the picture, she is a very capable, very qualified, very experienced scientist who has broken rank and is now blowing the whistle
Of course ifshe’s right they will just be put down to covid deaths and we’re back in lockdown
Scary stuff . . .
Thank you for including these links. Because you did, I discovered the wonderful site UK Columns. This seems to be a rare example of truth-seeking journalists (and citizens) simply declaring that if the local press isn’t going to report the truth – and indeed seems intent on hiding the truth – we’ll do it ourselves. The world needs about 50,000 such sites.
It was actually TCFC who included the UKcolumn link to Iain’s article. They are indeed serving an invaluable service.
UK Column News Monday, Wednesday. Friday at 1 pm. Fantastic guys, the truth’s out there.
“A review by a county in Sweden in August found that 85% of the 122 Covid deaths investigated were due to a different underlying cause.”
Right from the beginning I said we need to pick actual deaths and investigate – talk to GP, look at health records etc. How long would they really have lived if not for covid?
A widely cited paper gives 10 years. Written by a PhD student and literally academic fraud that assumed the longevity of anyone in the absence of covid would be the longevity of the ‘average’ person of that age/condition cohort but making no account of the severity of underlying condition.
Its not that 10% of average 70 year olds die (or whatever the number is) – its that the unhealthiest 10% of 70 year olds and they were going soon of old age anyway.
This is one of the key pieces of the fraud.
Excellent article with some interesting evidence that I’ve not seen before
This article from July 2020 showed how in a London hospital trust from 22nd-28th April most deaths were with covid not from covid (see attached chart from the report)
Changes in the hospital admission profile of COVID-19 positive patients at a central London trust
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7377982/
And the Scottish hospital audit from August is interesting although it represents the position in August 2020 so not entirely representative
https://blogs.gov.scot/statistics/2020/09/15/counting-people-in-hospital-with-covid-19/
The audit of inpatients identified 384 patients in hospital at 1am on 26 August across Scotland who had previously tested positive for COVID-19. The majority of these patients (87%) were in hospital for a condition unrelated to COVID-19:
……
The audit showed that 8% of patients were either receiving treatment for COVID-19, were in rehabilitation after their treatment for COVID-19 was completed, or were in hospital for COVID-19 related complications. (5% of patients could not be classified into the above categories.)
Of course if the number of “confirmed” deaths is reduced, the case and infection mortality statistics would be lower. Also, if more people have actually been exposed to the virus (than reported), the case mortality statistics would similarly be much different.
It would be nice if “case fatality” data was routinely presented by different age cohorts of the population.
For example, what is the case fatality percentage for a country’s population above the average life expectancy figure in a given country? I believe average life expectancy in the U.S. is 78.6 and 82.4 in the U.K. Thus, what is the probability a person will die if he or she contracts COVID and has already reached the average life expectancy?
Conversely, what is the probability a person will die if they contract COVID and are middle-aged or lower? This information can be presented by showing “case mortality” data for those who are under the median age in a give country (I think the median age in America is around 39 years old).
Journalists could also show the odds of dying for everyone in a given age cohort by simply dividing the number of people in a certain age cohort by the number of people in this age cohort.
To further provide a more accurate statistical representation of someone’s more-specific odds of dying from this disease, researchers/journalists could present these odds by race (mortality odds are much higher among Hispanics and Blacks, at least in America).
Finally, it would be interesting to report these mortality probabilities for those who do not qualify as “obese.” From my research, I’ve learned that “68 percent” of COVID victims were considered “obese” – one of the more telling statistics I’ve uncovered so far that gives readers a better glimpse of the “typical” COVID victim.
By providing such pertinent statistics, readers could, for example, calculate their own mortality odds of dying from COVID … if, say, they happen to be white, under 40, and are not overweight. The extreme differences in these better-defined mortality statistics (compared to those who have already reached their typical life expectancy and/or are significantly over-weight) would be eye-opening.
If such reporting was routinely done, it’s very possible the “fear factor” associated with COVID in much of the population would be quite different. And if this was the case, the “draconian” policies created to reduce one’s “risk” of dying from COVID might not be so stringent and life-altering. Basically, such honest and full reporting would show that the risks of dying from COVID – for probably the vast majority of the population – are infinitesimal.
Edit: Journalists could also show the odds of dying for everyone in a given age cohort by simply dividing the number of people in a certain age cohort (who died from or with COVID) by the the total number of people in this age cohort in a given country.
Oxford University do a calculator https://qcovid.org/ for the chance of hospitalisation or dying of Covid. It is from Oxford but it seems quite good and the risk of not dying for most of us is pretty high.
That’s a great link, thanks for that! Because of that I just learned that my risk of dying with covid-19 is 0.0029%. If I round that down to two digits it is 0.00%! And that’s supposed to be “the worst health crisis since 1945“…
In Sweden they have produced the underlying table. This is the calculated risk of dying of C-19 divided in sex, age group and co-morbidities but also factoring in the Health Care system. In the Coronabell curve in the US they have a similar calculation but the figures are worse most likely due to obesity and minorities in the US.
https://coronavirusbellcurve.com/#pa
Great article.
There is irrefutable evidence of GPs entering COVID as the cause of death on death certificates when it was known that the deceased was not infected with the virus. Add these numbers to those who died with and NOT from COVID.
If there is evidence that is against the law.