It is said that people can only worry about one thing at a time; if so, then I’m sure that few people are currently worrying about the recent increase in Covid cases in the U.K. This is a good thing – the hospitalisation and mortality rates of Omicron appear to be significantly lower than those of previous variants, so it’s surely time to just accept Covid as another type of cold that’ll give us all an annoying sniffle every couple of years.
But the sticky problem of the vaccines remains. Do they work or have they made things worse? Luckily, the UKHSA (just about) continues to publish the Vaccine Surveillance Report and as a result we can explore how the vaccines are impacting on Covid in England.
Cases
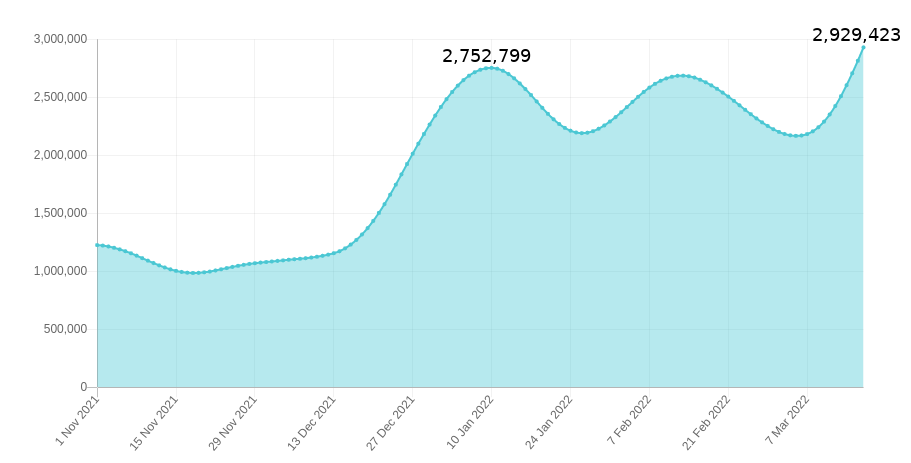
The new Covid wave, as defined by data from the Government Covid dashboard, appears to be gathering steam with new cases hitting 100,000 per day; it is easy to forget that the terrible Covid wave during January 2021 peaked at around 60,000 new cases per day (though this was admittedly before mass lateral flow testing had been brought in). We’re told that recent variants are nearly as infectious as measles – ignoring the surprisingly low household infection rate of Omicron variant, which doesn’t support the measles comparison. What do the data say?
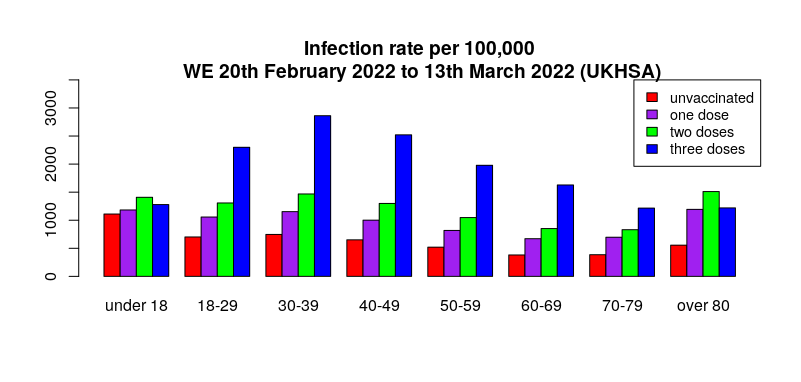
Yet again, the real-world data suggest that infection rates are generally highest in the triple vaccinated, with the lowest infection rates in the unvaccinated (see here for details on methodology and limitations). Could it be that the evidence for Omicron variant being as infectious as measles is only found in countries with high vaccination rates?
The delayed nature of the UKHSA data meant that in last week’s report there was no sign of the then emerging Covid wave – the question is, can we now see the latest Covid wave in the UKHSA data? Looking at all the weekly totals for all Covid cases there’s a hint of an uplift for most age groups in this week’s report.
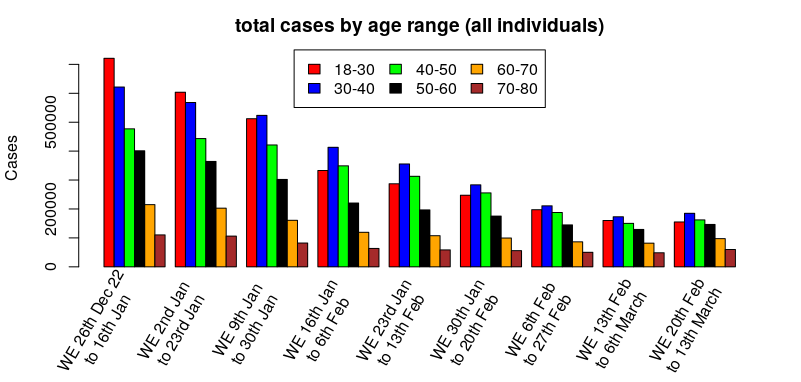
Hmm. The cases have definitely dropped significantly since the beginning of the year, but it’s a bit difficult to see if it is turning around – how about looking at the percentage change by week, that is, relatively how many more/fewer cases there are compared to the previous week:
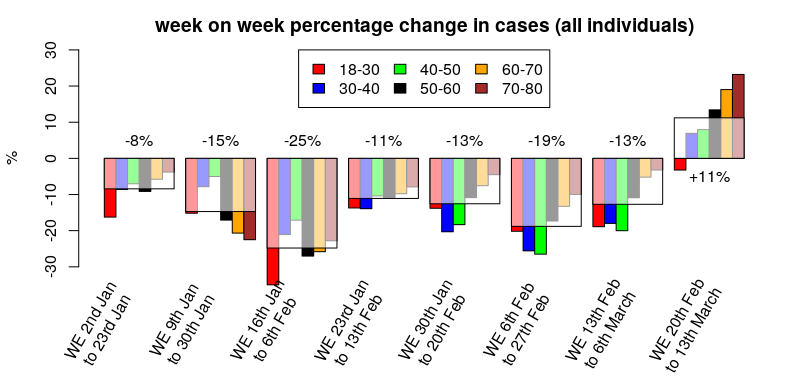
That’s better – cases appear to have been dropping since the start of the year, but this week’s report suggests that the reduction in overall cases has stopped and perhaps the start of the new wave can be seen at the far right.
What about by vaccination status?
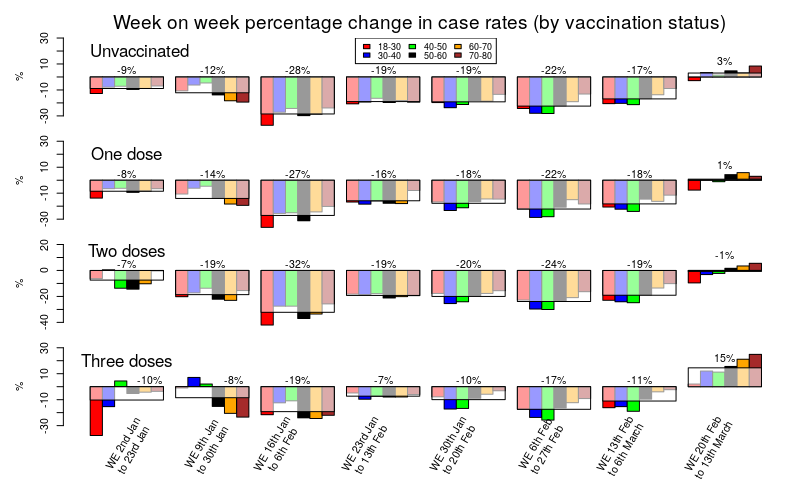
Hmm. That’s a busy graph, but perhaps if you stare at it for long enough a general pattern should become visible.
The change in cases for the unvaccinated, those with only a single vaccine dose and those with a double vaccine dose are very similar; a sustained reduction in cases since the start of the year, but with cases remaining broadly flat in this week’s data compared with last week’s.
Three doses of vaccine show a very different picture. Compared with the unvaccinated or those with one or two doses, the data for three doses show a much slower rate of reduction in cases, with generally about half the rate of reduction in cases compared with those that had taken fewer doses. Also note that this isn’t simply because the triple vaccinated had fewer cases; a glance at the cases graph earlier in this post clearly shows that case rates in the triple vaccinated are still higher than the unvaccinated, and previous posts have shown similar data for earlier time periods.
The big difference in the triple vaccinated, however, is in that final time period on the graph above (the column on the far right); in the latest data we can see that case rates have recently been broadly flat in the unvaccinated, the single dosed and the double dosed – but in the triple vaccinated we see a significant (15%) increase in case rate. It is noteworthy that the triple vaccinated make up the majority of the population for most age groups; are our new Covid waves being driven by the triple vaccinated?
These are still early days in the progression of the current Covid wave and this analysis should be regarded as preliminary – next week’s data should be interesting, if they provide it…
One more note on cases. I mentioned last week that the Zoe symptom tracker was disagreeing with the UKHSA and U.K. Government data on the drop in cases that we’ve seen over the last two months. The Zoe Symptom tracker has seen a sustained level of cases during that time (I have hypothesised that this is due to the 90 day exclusion period in the UKHSA data that would remove any reinfections). I mention Zoe because Thursday marked the point where the Zoe app’s estimate of the number of individuals currently infected with Covid in the U.K. exceeded the case rate during January, and with no sign yet of the increase in cases starting to reach a peak.
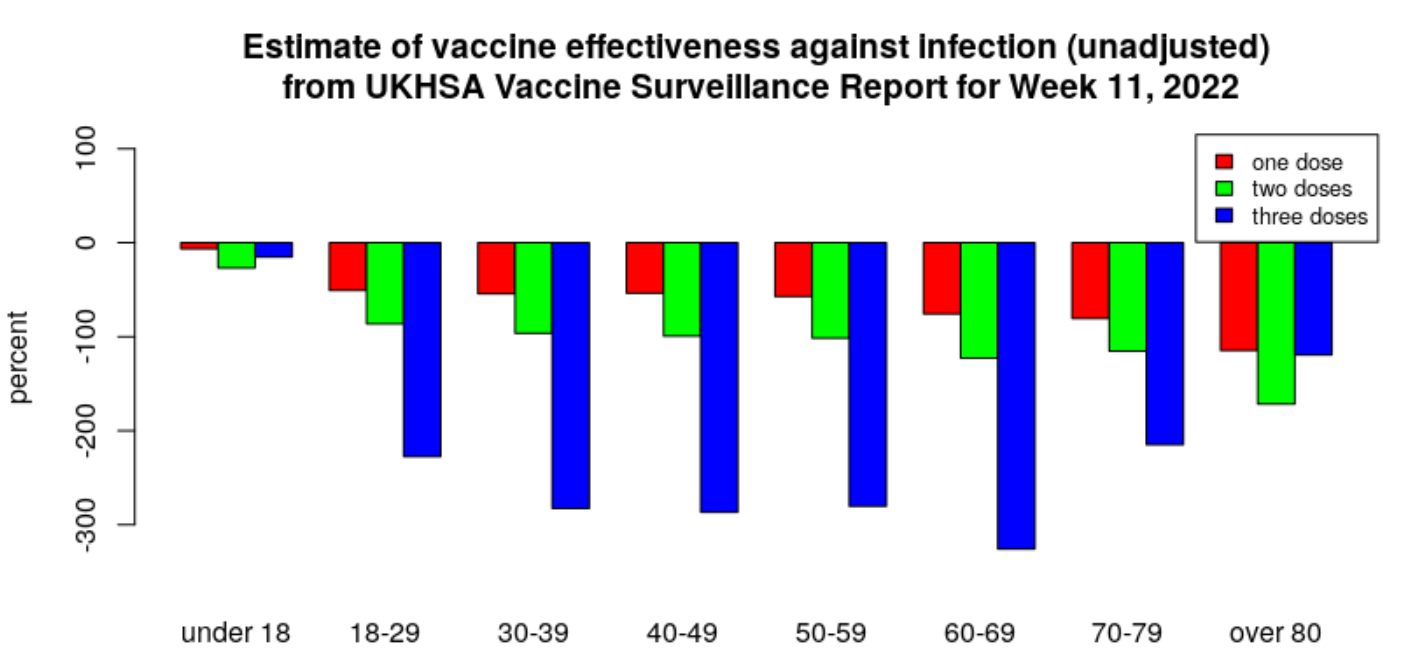
For the historical record, this is the current estimate of vaccine effectiveness according to the UKHSA data.
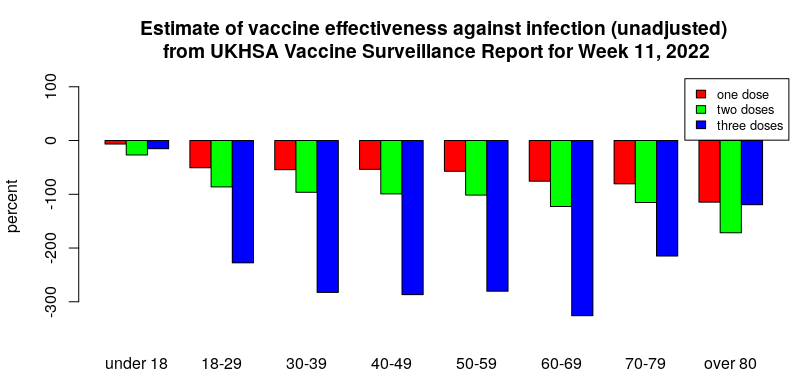
All are negative, meaning the infection rate in the vaccinated is higher than in the unvaccinated. It has reached as low as minus 300% for the triple-jabbed aged 30-70, with those in their 60s faring worst of all, meaning these groups are more than four times as likely to test positive as their unvaccinated counterparts.
Hospitalisations
The Covid vaccines appear still to be offering some protection against hospitalisation after Covid infection for those that were recently boosted, but the hospitalisation rate in those that stuck with one or two doses of vaccine is now much higher than that of the unvaccinated.
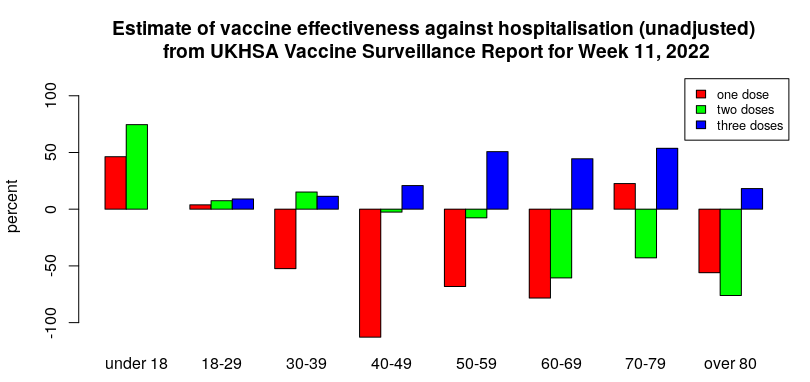
I’d note that it is possible that the higher risk of hospitalisation in those having taken only one or two doses of vaccine reflects them being more vulnerable than average (and thus passed over for the booster dose). If so, this ‘healthy vaccinee’ effect implies that the vaccine effectiveness against hospitalisation and death will be overestimated. That said, there remains the possibility that waning vaccine protection starts to be associated with increased risk of serious disease (possibly via antibody-dependent enhancement (ADE) mechanisms, which often only appear when the initial immune response starts to wane). It would be useful if some research was undertaken in this area.
An important aspect of the above graph is which age groups get the benefit of reduced hospitalisation after vaccination. The age group from 50 to 80 appears to have a reasonable level of protection (about 50%) and this might well support vaccination in that age range for those that are happy to keep on taking booster doses indefinitely (dependent on side-effect/complication rates). Protection in those aged over 80 appears to be poor – this is unfortunate as it is that age group that gets the largest share of hospitalisations and deaths. I also note that there appears to be very little reduction in hospitalisation in those aged under 50; it is questionable whether this level of reduction is at all relevant for younger individuals.
Deaths
The UKHSA statistics for deaths within 60 days of a positive test show a similar trend for the effectiveness of the vaccines to that seen for hospitalisations (only data for those aged over 40 are shown – Covid death rates are too low in those aged under 40 for meaningful analysis).
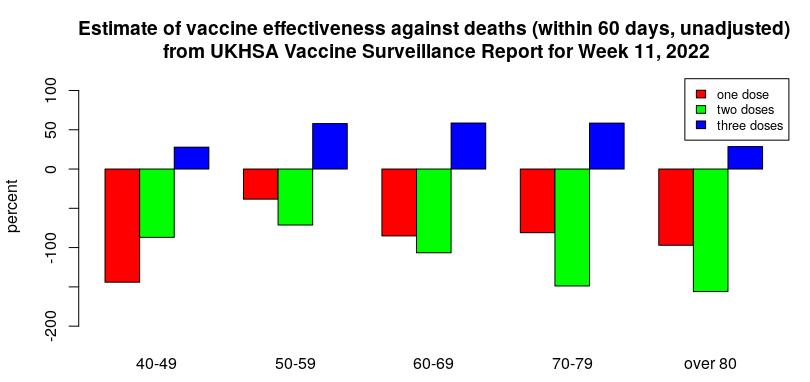
It is important to note that deaths with Covid have reduced significantly since the Omicron variant arrived. Thus, despite the apparent protection against Covid death offered by three doses of vaccine, it is questionable whether there is now much in the way of absolute, real-world benefit.
There is a worrying trend in the deaths data, however – the change in distribution between deaths within 28 days and within 60 days.
Historically, most deaths with Covid have occurred within 28 days of infection. However, there have been some additional deaths beyond this point; in general, each week’s report has seen an additional 20-25% deaths with Covid between 28 and 60 days after infection.
Over the past few weeks, the proportion of deaths with Covid in the 28 to 60 day period after infection has steadily risen until it accounts for approximately as many deaths again, as seen in the graph below.
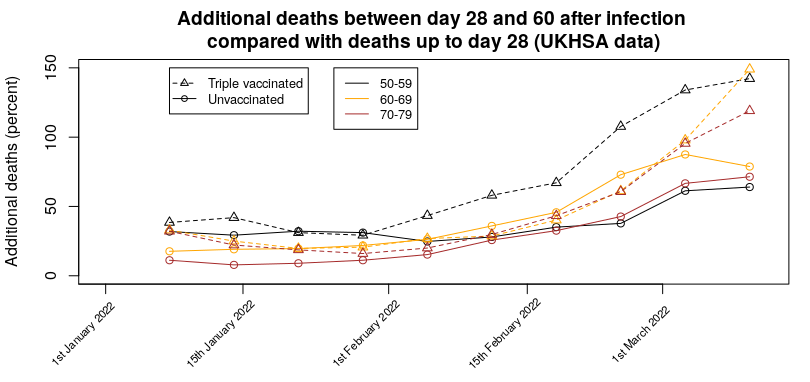
Even worse, there appears to be a vaccine effect, whereby there are more additional deaths in the triple vaccinated group (approximately 140% of the 0-28 day deaths in the latest report i.e., nearly one and a half times as many deaths occurred in the 28-60 day period as in the 0-28 day period) compared with the unvaccinated (approximately 70% of the 0-28 day deaths i.e, the number of deaths occurring in the 28-60 day period was around two thirds of the number occurring in the 0-28 day period). This means that in the triple-vaccinated we’re seeing more deaths with Covid in the 28-60 day period than in the 0-28 day period. This effect is also visible in the data for one or two vaccine doses. For the most recent week the day 28-60 deaths are 130% (single dosed) and 170% (double dosed) of the 0-28 day deaths.
It isn’t clear whether this effect is due to infection with the Omicron variant taking longer to get to the stage where hospitalisation is required, people remaining seriously ill inside hospital for longer, or more people dying outside hospital. It is also possible that this effect is due to changes in treatments being used in hospitals.
Given this effect, it is likely that the current ‘official’ death figures for Covid are now lower than they should be (though I note that ONS excess death estimates have also been low since Omicron arrived), and that official estimates of vaccine effectiveness against death will overestimate the protection offered.
Another interesting effect seen in the deaths data is the ratio between the deaths rate and the hospitalisation rate.
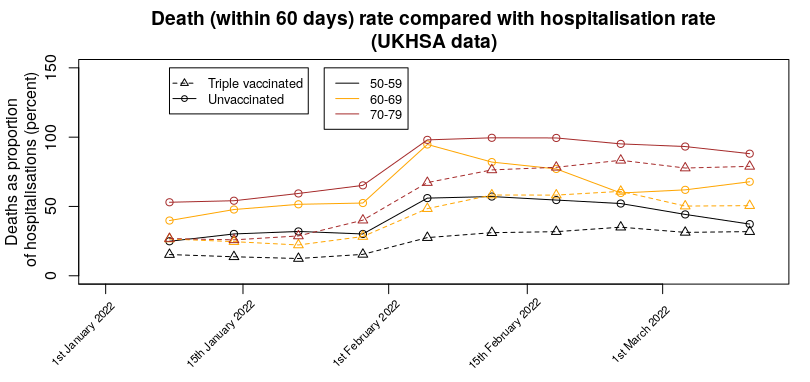
There does seem to have been a change in the number of deaths compared with hospitalisations over recent weeks, with a marked increase in February, so that more are dying per hospitalisation. It is unclear why this has happened. Note that is isn’t simply the hospitalisation death rate – many deaths with Covid appear to be occurring outside a hospital setting. This effect is seen most clearly in the proportion of deaths vs hospitalisations for one and two doses; for those aged 70 to 80 there are more deaths than hospitalisations (about twice as many for a single vaccine dose, about 50% more for the double vaccinated).
One more thing…
Arguably, the most important news in this week’s UKHSA Vaccine Surveillance Report was buried in the text (my bold):
From April 1st 2022, the U.K. Government will no longer provide free universal COVID-19 testing for the general public in England, as set out in the plan for living with COVID-19. Such changes in testing policies affect the ability to robustly monitor COVID-19 cases by vaccination status, therefore, from early April onwards this section of the report will not be updated. Updates to vaccine effectiveness data will continue to be published elsewhere in this report.
This was probably inevitable – the real-world data on the vaccines are consistently failing to support the Government’s position that the vaccines have actually helped significantly. While the excuse given appears reasonable at first glance, a few minutes thought reveals it to be weak – while there might be issues with overall cases and testing, testing at hospitalisation and to a certain extent death will continue. In addition, it is likely that routine testing of healthcare workers will continue for some time. It would have been trivial for the UKHSA to have continued to show data for hospitalisations and deaths and included a section on case rates in healthcare workers. But instead they’re using the occasion as an excuse to remove all data. I also note that the Zoe symptom tracker app has lost funding – their data were also going against the official narrative. Thus, like tractor production in the Soviet Union of old, the only statistics we’ll be allowed to see are those that aren’t inconvenient to the state.
Hopefully we’ll get at least one more set of data to see how the impact of the more recent changes outlined in this post have played out.
Amanuensis is an ex-academic and senior Government scientist. He blogs at Bartram’s Folly.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
What’s happening in Hong Kong?
And South Korea
Norway too
The Hong Kong situation is rather weird.
It could simply be that the vaccines do protect those at ‘intermediate risk’ (60-80 yrs) and we’re seeing the impact of lower vaccination rates in that age group there. It is a bit odd that Hong Kong has vaccinated 80% of the population over 12 (similar to Western countries) but only 1/3rd of those aged over 80.
It is worth highlighting that the vaccines do seem to protect against hospitalisation/death, but also seem to increase risk of infection (and presumably also transmission)– thus a situation where you vaccinate all the young people but not the old would seem to be exactly the wrong thing to do — the right approach with this type of vaccine would be to vaccinate as few people as you could get away with, ie, only the most very vulnerable.
In addition, I don’t trust any of the Covid data out of China –right from the start there appears to have been an attempt to suppress the existence of the problem, and then to massively exaggerate the problem — there is something rather suspicious about China and Covid.
I suspect that as a positive test results in 3 weeks in a prison cell most people are trying to keep quiet about a positive test.
I just wonder when people talking about ‘impact’ on unvaccinated are going to figure out that the unvaccinated cohort is getting smaller by attrition, not bigger… people don’t become unvaccinated. Nor are all unvaccinated people susceptible.
Sooner or later we’ll be down to the last vaccinated person – then what will the explanation be?
I’m not quite sure of the logic in the above (did you mean unvaccinated in the second para), but
The unvaccinated vs vaccinated (any dose) cohorts are now broadly flat — ie, people that have chosen to remain unvaccinated to this point aren’t changing their minds. It looks like attrition rates are similar in each group.
I imagine that if we get to no more unvaccinated they’ll still blame the unvaccinated — like vampires or witches in the middle ages, they’ll be the bogeyman to explain all ill.
‘It is worth highlighting that the vaccines do seem to protect against hospitalisation/death…’
Do they? Based on what evidence? There is no data to support that oft touted claim, and it is easily falsified because vaccinated people are being hospitalised and dying. If there is a causal relationship between two variables, there must be correlation. Just one hospitalisation and/or one death means there is no correlation.
I’m always in two minds when I say that they protect against hospitalisation/death; the top level figures do support this view, but whenever I delve more deeply I come up with too much data suggesting the vaccines offer no benefit.
I suspect that the vaccines are introducing immune tolerance, which would make the risk of hospitalisation following each infection lower, but which results in an increased risk of infection in the first place, cancelling out the benefit.
And that’s before you start adding in side-effects/complications arising from the vaccines.
As it stands I’m persuaded by the data that are available that there is some residual benefit in terms of hospitalisations/deaths before side effects are taken into account. This benefit is probably of the order of 10-20% for most people. Side effect rates are yet to be determined.
The big problem I have with all this is whether the benefits will decay to zero, or whether with time it’ll go negative for hospitalisations/deaths as well; we can only hope that if this happens then it won’t be by too great an amount.
Hope is, of course, a poor strategy.
Firstly, thank you for your excellent data analyses.
My other point is that in weighing up costs v benefits re the jab, it is always assumed that all deaths are equal. I believe this is an over-simplification. Humans are not robots: we have (illogical) emotions. As a consequence I would argue that some deaths are more tolerable than others. For instance, a random death from being unlucky enough to catch a fatal dose of a disease is less intolerable than the case of a healthy person actively choosing to be jabbed and then being one of the unlucky ones who suffer (the rare outcome of) a fatal heart-attack. A more potent example would be that of a parent who takes their exceedingly low risk of serious infection, healthy child to be jabbed and the child dies as a result. Humans are much more accepting of bad outcomes where they were completely passive in the process but unlucky, compared with death in a healthy person resulting directly from their own choices. A 1:1 equivalence of the two scenarios does not apply but medics, governments, etc completely ignore this human trait. It’s what explains why a significant number of sensible, low risk people choose to avoid being jabbed.
Public Health uses the Quality Adjusted Life Year to guide spending.
To save a child with potentially many decades of life ahead is far more valuable then to delay death by 6 months of a person in their 90s.
To vaccinate and kill a child on the other hand is far worse.
The measure sounds cold but it agrees with what our gut instinct tells us.
Cold or not, it’s a metric that all insurance companies use, because they live in the real world with consequences for bad decisions, unlike politicians.
You say they seem to protect against hospitalisation and death. Is that still the case if they include people as vaccinated who are actually are vaccinated and not ignoring those within 14days of a dose? Prof Norman Fenton and his team have shown that when you take this into account and properly count people as vaccinated they are ineffective. Also there now seems to be increasing hospitalisations and deaths from other things in the vaccinated- such as strokes, heart attacks, clots, cancers, neurological problems etc. Will this be the damage to immune systems that some Drs are seeing? Some in the funeral business report now seeing a 600% increase in thrombosis related deaths and the ages are getting younger and younger. This doesn’t give me any confidence whatsoever.
Please remember that Hong Kong has used the Sinovac vaccine for many of its vaccinations. So you are not comparing like with like.
It’s Poot’n’s fault – everything is just now apparently, prices at the pumps, shortages in the shops, climate change…
Burying bad news? No surprise there.
The show’s over folks. There’s much more fear and suffering to scare us with now in Ukraine. Covid fear porn is old hat.
For the moment
And many countries are still promoting useless and harmful ‘anti covid stuff’, such as vaccine passports and masking of children.
I’d very much like covid to go away — it is now very close to the risk of OC43 for most people — ie, the ‘deadly influenza’ that caused problems in 1889 and that we all now live with as ‘just another cold’.
Of course it is when you now want everyone to get their “Spring Booster” – does that come with a bunch of daffodils I wonder?
Meanwhile – the BBC touts as some kind of near miracle almost worth approaching the vatican for some kind of sanctification a man with a compromised immune system in Wales who couldn’t recover from his covid bout and languished at home like a prisoner for over 7 months but has been liberated by having the covid jab, which enabled his recovery and is being hailed by the BBC as the first case where the miracle jab has been used to “treat” a covid infection, as opposed to merely prevent one (someone needs to explain to BBC that the jabs don’t prevent them even though Pfizer lied to FDA and told them that they would do that when they knew that wasn’t the case as their released papers show).
Wonder if they tried him in Ivermectin first, or if they just went straight to jab as ‘treatment’? If in doubt…
And in other news Raphael Nadal lost in the Indian Wells final, and was 4-0 down in the first set with “breathing difficulties” and needed medical treatment, saying it was “tough trying to get a breath in”. Novak Djokovic must be watching with interest.
The chocolate ration has increased
We are producing 400,000 more pairs of boots
We have always been at war with East Asia
And handily enough, we have even found ourselves an Emmanuel Goldstein
We’re at war with Eurasia.
But don’t worry, we’ll be at war with East Asia soon enough.
This year: We’re at war with Russia, we stand with Ukraine.
Next year: We’ve always been at war with Ukraine, we stand with Russia.
China is much more of a problem. I don’t understand why our authorities have driven Russia into allying with China — seems pretty stupid to me.
I’d say because across the Western world we now have the worst batch of politicians that we have ever had. They genuinely believe in the superiority of the West, while undermining the foundations of Western culture at every turn. Inviting in such large numbers people from such diverse and different cultures will dilute Western culture and the strenghts that culture has provided, but they seem not to see that (certaintly the dilettantes who think governments are some type of charity institution who are there to help all and sundry, rather than the citizens of the country they are supposed to represent).
Brussels is the perfect example. Almost everyone there is a former national politician – they all have the same self-serving career interests, they are virtually all university educated, speak several languages, all on incredible pay packages with benefits. They genuinely believe that a fisherman in Spain is just the same as an electrician in Poland, a farmer in Bulgaria is no different from a teacher in Germany. Just shove them all together, wave a magic wand, and there you go, a whole new one-nation Europe. Except it does not exist except in Brussels. If Europe really does get dragged into a war to protect Ukraine, just watch how fast ‘Europe’ disintegrates and how few people truly ‘stand with Ukraine’. The EU can’t handle Europe, no way it can take on China.
As for China – the West has outsourced so much to China, it can’t afford to get into a political fight with it, let alone a military one. Poor Taiwan, I do think China will make a move one day, and we won’t see any Taiwanese flag emojies then, they’ll be on their own.
There was a lot of standing with Ukraine during the televised sports events over the weekend.
That was when they weren’t taking the knee or making announcements about “rugby against racism”
Oh for the good old days when sport was just sport for sport’s sake.
We have always been at war with East Anglia
‘it is easy to forget that the terrible Covid wave during January 2021 peaked at around 60,000 new cases per day’
Very easy to forget, I must have slept through that
Me too. I am beginning to suspect that I am not human, just another creature who hibernates during the long dark winter.
Horrible mental image, but how many people had to stick a swab up their noses to collect snot to get 60k new cases?
The covid stats appear to be counting the number of people with a ‘bad cold’ during winter.
This seems rather irrelevant and is a good reason to just forget about Covid and unlock the world.
But the important point is that universal vaccination has significantly increased the number of people with said ‘bad cold’ and they’ll be wandering around passing Covid on to others — resulting in escalating in cases.
The end result of all this is increased cases in the vulnerable, some of whom will go on to die (as the vaccines don’t offer much protection in the vulnerable).
Thus the impact of the vaccines is to offer protection from death for the people who wouldn’t have died anyway, and massively increased the risk of catching Covid in the vulnerable, who don’t get much protection from the vaccines.
It really is looking like we’re in a far worse place now than if we’d only vaccinated the most vulnerable.
See above.
Didn’t you see the piles of bodies in the streets? It was terrible.
Quite. I still know of no-one that’s died or even become seriously ill with covid. I do know, however, rather too few people that have developed rare conditions that have had an impact on their lives over the last 9 months or so (and a few ‘sudden deaths’).
Actually, the number was higher:-
Positive test peaks
Specimen date:-
Date +ves tests rate %*
29.12.20 83090 344775 24.1
4.1.22 275591 2050101 13.44
Highest rate this winter by +ve date reported:-
01.01.22 179637 1029656 17.45
*the msm give bald, scary, numbers: only the rate is important for comparisons.
For the record, the rate in mid/late summer 2020 was <0.2%.
Don’t forget that a few weeks ago deduping of +ves for the same person was stopped thus all tests from the same person are now included which has an obvious and absurd impact.
Data source: government dashboard maintained by PHE.
Erratum: it was c.0.4% mid August. The following April 26 it hit 0.14%.
Go back one
What data?
The data is based on an inaccurate test?
The data from UKHSA is flawed and therefore no analysis is possible and no conclusion can be drawn
UKHSA data only fit for the bin
The quality of the tests is open to question, yes.
Nevertheless, the differential in the results by vaccination status tells us that something is going on (if the tests were completely hopeless the results for vaccinated and unvaccinated would be identical).
Unless testing is more prolific in one cohort than another. The data is meaningless unless we know how many in each cohort were testing.
Apart from the first ‘wave’ when the number of ‘cases’ was about 10% of the alleged deaths – so clearly no correlation, subsequent ‘waves’ showed ‘cases’ disproportionate to alleged deaths, so were in fact Testademics.
The testing frequency for hospitalisations/deaths is sound.
No
For a vaccine that is supposedly 96% effective at preventing infection I think someone may have been telling porkies
96% at reducing risk of infection, but risk of infection is 0.88% so the absolute risk reduction was 0.84%. Doesn’t sound so good does it?
Given that risk of death from infection is 0.15%, the risk of death across the population prior to the pseudo-vaccines was 0.00132% – for this we near destroyed ourselves.
What an outrageous comment. Shocked. Shocked I am.
Well I never.
Clearly missing something here – deaths within 60 days of a positive test. Thought this old chestnut was put to rest. Death of or with covid. Is it mentioned above? Currently have an an old friend in hospital who is 94 and seriously ill unrelated to covid. Needless to say he has now caught covid in hospital. If he dies within 60 days he becomes a covid death? The same applies to a friend’s mother-in- law who is getting end of life care and has also now contracted covid.
In my experience, this relates to the vast majority of the current covid deaths. People who are going to die with or without that positive PCR test. I don’t know what they even test them for.
The purpose of tests was to create “cases” and thus make a plausible case for va$$ines.
Indeed.
It would have been helpful if right from the start they’d properly counted hospitalisations and deaths by:
‘incidental covid’, ie they were going to be there (or dead) anyway, and
‘causative covid’, ie they were healthy but then covid got them.
But the data offered is all we’ve got, so we have to try to work with it.
Hopefully the analysis should say ‘if you’re not old or otherwise vulnerable there really isn’t much threat from covid’ and ‘the vaccines don’t seem to offer much for the healthy non vulnerable’
Whilst I’m pretty fed up with the constant barrage of lists of “cases” and the various statistics (true, false, or biased), it seems to me that there are some areas which could have done with more explanation, but now will probably not.
If I’m wrong, please tell me, but the “vaccine” effectiveness and other related stats appear to be based on simple factors i.e. vaccinated or not, and number of doses. As I understand it, the two main jollops given were the Pfizer mRNA and AZ’s adenovirus-based stuff. Whilst the technologies are similar, there are differences.
Again, as I understand it, the “booster” or third (and subsequent doses) are Pfizer, irrespective of whether the first/second were AZ or Pfizer. As a layman, I would like to know whether the types of vaccine, or the mix’n’match approach, have any bearing on the efficacy, possible ill-effects and so forth. Presumably the information on who got what and what happened to them is held somewhere, but I can’t see where it is published.
It was initially published and there’s an article on daily sceptic about it.
I am not sure that anyone now is even looking at it.
After all, the “safest” thing to do is to not look as then you definitely won’t find it.
I’ve heard that this is the motto of the ons.
the “safest” thing to do is to not look as then you definitely won’t find it.
Ostriches are definitely in the ascendant.
What has also surprised me (but probably shouldn’t, given the track record of those involved) is how the JCVI et al can have so swiftly agreed to, and then asserted, that mixing up this stuff, let along repeatedly injecting it, is just fine and dandy, and “what the doctor ordered”.
When it comes down to the claim that even if everything to do with the “vaccines” is beneficial, although done “at pace”, it is just not believable.
Although I have concerns about mixing these chemical concoctions and what this could mean over the longer term for people, in terms of vaxx efficacy I don’t think it makes much difference. The efficacy of all of the vaxxes approved in the West (mRNA Pfixer/Moderna and viral vector AZ and J&J) wanes over time, as all of them only produce specific antibodies, which wane.
There may be a difference in the time span for waning, but that would appear to be it. Israel, which by and large only used Pfizer, was the one who started boosting back in the summer and knew by November that the 3rd shot was waning and without any actual trials simply started shoving a 4th shot in people because – well, why not.
I have just had a call from my surgery inviting me and my wife for our 4th shot on Friday as we am over 75.
I do not know what to!!
So far as I know I have not caught it and have been taking enhanced Vit D since the start of this farce. My daughter who lives with us has had Covid serveral times but we have been fairly strict about keeping our distance. She is also triple jabbed.
Do I stick or twist????
They’re really not telling us — anything that might be ‘vaccine negative’ is withheld by government.
Harder to apportion blame for side effects if two varieties taken. Is that part of the deliberation? Nevertheless I see lot of people in the financial markets selling vaccine companies as they believe they will eventually get their comeuppance. Others then come in and buy who have decided that they won’t, and then another lot short or sell, and so it goes on!
I would suggest that the rising case numbers amongst the triple vaccinated are entirely expected at this point (and indeed I told my friends this would be the case).
The reason?
We know that the booster effectiveness was found to last for about 10 weeks. We knew this in December when the government decided to boost everybody who would stand still long enough.
We are now 10 weeks from the ill informed, misguided booster campaign.
We will see cases rise for another 3 weeks in this group as each boosted group reaches the end of the meagre temporary “protection” the jab provided.
Meanwhile, I hear in dismay about people suddenly dropping down dead and weird aggressive cancer diagnoses and people needing repeated biopsies on lymph nodes that just don’t look normal on scan…
What do you think is happening to produce enlarged lymph nodes?
Cancer. And they’re covering the extent of that up too by claiming many are the result of the NHS backlog, see how that works?
And if you drop dead from a stroke it was probably due to stress thinking about those poor Ukrainians.
And your heart attack was most definitely caused by chaotic temperature fluctuations due to climate change.
Now you’ll have to excuse me please, i’m in the middle of trying to budget for a new £40k electric car because I can’t afford £2/L petrol.
Brilliant, though also deeply sad.
Lymphadenitis is probably related to the mRNA continuing to produce spike proteins far beyond the ‘few days’ that was initially described (without evidence).
The swelling will probably reduce once the vaccines stop doing their thing (obviously cancer is a potential risk and it shouldn’t be ignored).
The big problem is the downstream consequence of continued spike production — I guess we’ll find out once people start doing the research on it. Funny to do the research after vaccinating the world, though.
Yes that was my thought as well. If its caused as a result of inflammation due to immune system response then its probably temporary. Cancer problems in lymph nodes are usually because there isn’t an underlying immune system issue.
The figures from Canada extrapolated here show an alarming decline in the immune systems of the triple vaccinated. The article begins:
If this wasn’t backed up by copious graphs from Trudeau’s honest statisticians I would dismiss it as over the top scare-mongering. However it all looks rather credible to me. VAIDS is with us.
Here’s the link: https://dailyexpose.uk/2022/03/20/gov-canada-data-triple-vaccinated-have-a-i-d-s/
It concludes, rather alarmingly:
Please tell me this is the ravings of fringe bacofoil journalism. I’ll take some convincing.
Good news this morning is, my inlaws are not getting the 4th vaccine! I’m shocked, I didn’t believe it possible. One of my SIL works in the school vax program, the othe had Cancer and flies the “I’m immunocompromised” bannor like a virtue signalling batman signal, first in line for every vax dose, including 4th.
You’d have to know my M&FIL to get how huge that is, mid 80’s, retired business owners, BBC faithful, MSM right on, swing voters but Tory voters since Thatcher may swing back to labour nex time, very “middle england”. If the gov lost my inlaws it’s safe to say they lost middle england IMO.
Sadly, they’ll probably take it next time they dial up the covid fear dial.
I suppose I am like your inlaws: believed government/MSM, got my 1st and 2nd jabs and thought I’d protected myself and family (I’m 86). Then suddenly we’re told that the immunity had waned and we needed a booster. That’s funny, didn’t mention that when we got the jabs – didn’t they know that from their testing? Well, OK, I’ll have the booster (Oct ’21). Then we find out that jabs 1&2 only gave 20 weeks immunity and the booster another 10 weeks’ worth. Hey, what’s going on here?
So I started watching John Campbell on YouTube, Daily Sceptic, Unherd, read Robert Kennedy’s book on Fauci/Gates. Also started taking high dosage vitamin D, K2, zinc and am now resolved never to be jabbed again with these incompletely-tested “vaccines”. Fourth jab (booster) next autumn? Forget it, I’ll take my chances, thanks. I’m “middle England”, and now anti-lockdown, anti-mask, won’t again believe anything the government and the MSM says about pandemics. I don’t like being lied to.
Epoch Times has good advice from World Council of Health re medicines/prophylactics.
How to Detox Spike Protein After COVID or Vaccine (theepochtimes.com)
The format assumes people are bright enough to understand choice, contextual application, and moderation, so in my judgement it is fine to post on this website!
That is good news – I am glad they have seen sense.
I wish I could say the same for my elderly parents who fit your description of your inlaws to a T but unfortunately they are both in thrall to the NHS and treat their GP as akin to some kind of God. I would imagine they are ready to roll up their sleeves at the first possible opportunity.
And there is nothing I can say which will make them change their minds – if anything I fear that if I was to try to dissuade them it would just harden their resolve.
So all I can do is stand on the side lines and watch as they submit themselves to something that at best will cause them further harm, if not lead to their deaths.
If anything can suggest something helpful I could say to them which might make them change their minds I’d be very grateful.
I imagine that many of those who have not had any vaccine also do not subscribe to the testing and reporting regime that many of the compliant do.
I expect this to have an effect on these figures. Are there any statisticians who can suggest what the effect would be?
We don’t know, because the data aren’t being collected.
They should have done proper prospective matched cohort studies as they vaccinated each age group.
Sure, right at the start there might not have been time for this (Dec 2020), but there have been ample opportunities since.
This way we would now have proper statistics on the effectiveness and safety of the vaccines.
I suspect this is exactly why it wasn’t done — as it stands the various authorities can claim victory by their vaccine programme and any inconvenient facts about them being useless/making things worse can be suppressed.
Nevertheless, I consider it completely barmy that these studies weren’t done.
The injections are designed to maim and kill. Once that is taken on board it is easy to see why proper safety studies were not done – they knew what the results would be.
Thank you.
It is called a confounding factor – often unmeasurable – which introduces an unknown margin of error. In effect it makes all data that does not/cannot correct for confounding factors useless.
https://live.childrenshealthdefense.org/shows/financial-rebellion/qeGXsHDo0u
We have got to stop banging this tired old drum of cases and infection rates.
It perpetuates this lie, and that is its aim. This discussion is a deliberate obfuscation and misdirection of attention.
The above link is to an important interview with Sucharit Bhakdi,. He says
In other words the Bhakdi interview conclusively shows that this discussion should move on.
Why are our governments knowingly injecting a toxic product into pregnant women and children?
5G Technology and Induction of Coronavirus in Skin Cells. NIH retracted this paper in 2020 because…..well you’ll see why after reading the abstract:
“In this research, we show that 5G millimeter waves could be absorbed by dermatologic cells acting like antennas, transferred to other cells and play the main role in producing Coronaviruses in biological cells.
DNA is built from charged electrons and atoms and has an inductor-like structure. This structure could be divided into linear, toroid and round inductors. Inductors interact with external electromagnetic waves, move and produce some extra waves within the cells.
The shapes of these waves are similar to shapes of hexagonal and pentagonal bases of their DNA source. These waves produce some holes in liquids within the nucleus. To fill these holes, some extra hexagonal and pentagonal bases are produced. These bases could join to each other and form virus-like structures such as Coronavirus. To produce these viruses within a cell, it is necessary that the wavelength of external waves be shorter than the size of the cell. Thus 5G millimeter waves could be good candidates for applying in constructing virus-like structures such as Coronaviruses (COVID-19) within cells.”
You could trust FullFact’s smearing of the article, that skin doesn’t absorb millimeter waves, or you could go and look at what happened to the protesters in Canberra a few months back and make up your own mind.
There’s a reason this subject is a black hole, because it’s a key part of the scamdemic, and they want it rolled out everywhere double-time without waiting for safety standards (which they have long known about anyway and don’t publish).
Can you provide a link to this paper please?
There’s a saved copy here.
You’re not supposed to be within hundreds of meters of the towers/booster hubs, but they have been installing them on schools and public buildings anyway, often the warning notice to stay well clear will be so high up the pole you can’t even read it. None of the people who live nearby are told what’s being installed near their homes or about the health risks of living near them.
During the 2020 lockdown they were installing these things everywhere as fast as they possibly could when there were fewer people around to notice.
Wuhan was the first place to switch on their 5G network, and early on people did notice a correlation between 5G active areas and covid outbreaks in places like Canada.
I believe this is also why they put graphene into the vials, because it absorbs EMF radiation at a much greater rate than your body would naturally, turning jabbed into living antennas whose bodies can be stimulated to produce pathogenic effects simply by having specific frequencies beamed at them. And if there is a genetic sequence involved, like the above paper suggests, a fake test can be devised to test for it, completing the illusion of a virus being the cause.
“Why are our governments knowingly injecting a toxic product into pregnant women and children?”
You know the answer Kate – depopulation.
For the purposes of killing and population reduction.
Greece has a vaxx mandate for over 60s and Italy for over 50s. It is not clear yet whether those will remain in place even as other countries lift measures. I think I read something about Germany wanting to introduce a vaxx mandate for over 50s. We know that the vaxx is a therapeutic at best (personally I don’t think it is anything positive, but the authorities can now only argue that it is no more a therapeutic). The fact that they would be willing to violate any number of laws on fundamental rights and freedoms to a) selectively impose measures on one group of people purely based on age and b) impose medical treatment on people against their will and then particularly in that pesky, costly group of (near) pensioners is making me increasingly think there is evil and wilful intent involved.
People were softened up to the idea that a person’s body could be physically violated, by taking a step back and saying society at large is free but this one group requires this ‘extra’ protection, all the people who are not
Jewsover 50 might be perfectly happy to accept what is entirely unacceptable.The point of the analysis of cases/hospitalisations/deaths is to highlight that the vaccines aren’t helping.
Analysis of side-effects/complications is also ongoing.
Yes, but –
It can be shown that the vaxxes do not work by looking at the Pfizer trial documents which started to be released in December, following the FDA court case. It reveals a deliberate falsification of medical evidence.
The vaxxes never worked. They harmed more people than those in the placebo group. This injection has no supporting evidence for it’s EMA authorisation.
The question is why do all governments continue to push these known toxins onto young children at no risk from Covid?
Precisely
I completely agree Kate – well said!
I think our focus on this is now misplaced, as it is now sadly so much ancient history.
With the WHO about to negotiate a treaty which will require nation states to transfer their sovereignty to it in order to enable the mass vaccination and vaccination IDs (the contract for which has already been agreed) there is a strong suggestion that covid19 was nothing more than a “trial run” to put the infrastructure for all of that in place. THAT is where we should be directing our focus and attention.
COMMENT: A WORLD GOVERNMENT UNDER THE AUSPICES OF THE WHO AND THE UN PROMISES US? – Platforma39 (domengorenseklaw.com)
Vaccine Effectiveness Hits as Low as Minus 300% – as UKHSA Announces it Will No Longer Publish the Data
The bbc telling us the reason for the future rise in cancer.
https://www.bbc.co.uk/news/science-environment-60761972
It is amazing how many ‘new reasons for bad things’ are coming out at exactly this time.
my BS detector went mad when I read that – I thought I was going to have to have someone come out to inspect it it was bleeping so badly
Yeah, thing is, people of all ages who have been vaccinated are getting all kinds of serious illnesses that are difficult to explain and have no prior history.
Thats anecdotally for me. Of course the relatives of said sick people never suspect the clot shot. I’ve yet to bring myself to suggest it, knowing how that will likely blow up any social interaction.
Interesting to hear other people’s experience of this. I have 3 members of my family who have got cancer in the last 2 years, one probably started before the jabs but seems to have reached stage 4 very quickly. 2 have now died, the other is probably going the same way shortly. None of these had what are termed ‘prior conditions’ and no history of cancer in the family as far as I know. My BIL in particular was very fit and playing golf at least once a week.
I believe that the jabs, if not directly causing the cancer, may well have prevented any immune system reaction to it and probably worsened their reaction to chemo (which two of them had). Having said that, they were all elderly, 70s/80s and so the rest of the family just assumes that this was going to happen regardless of Pfizer doing their worst. I am sure this applies to thousands of others.
Yes, it does. I know two people who have been struck down by cancer in the last 2 years.
One began in late 2020, treatment was delayed because the medics insisted on 2 weeks quarantine before every appointment, but by early 2021, they seemed to be on top of the cancer. Then along came the jabs. She has had at least 2, possibly 3. During the summer and autumn of 2021, the cancer spread like wildfire, she has had various treatments but there is now talk of hospice care for her. She’s in her early 60’s. Again, previously a healthy and active person.
The other wasn’t even ill until late 2021, post jab. Again in his mid 60’s. Previously very active, running own business, working 5 or 6 days a week, very happy in his work. Now he is very poorly, cannot work, family trying to find a buyer for the business.
Both with no prior conditions, and at least one with no family history of these cancers.
Certainly, this might have happened anyway, but the rapid onset and growth makes me think that something else is behind it. And these are not elderly, frail people – or at least they weren’t.
Common denominator: the jab.
The family firm that put in my garage door – the owner a fit and active man at retirement age just went blind in December. Blood clot in optic nerve post vax.
In my small village there is usually, on average, one death and one serious illness per year.
This year there have been 2 deaths (cancer, sepsis), one blindness, one baby born with enlarged kidney, one gall stone, one appendicitis, one stroke. It does seem as though something is at work here and the only common denominator is the jab.
“the jabs, if not directly causing the cancer, may well have prevented any immune system reaction to it and probably worsened their reaction to chemo”
It could be both of those things – Ryan Cole, the US pathologist, has seen a downturn in the ability of the immune system to fend off cancerous cell growth which he is able to attribute to the jabs.
I know of a case of a very young girl [20] who is being treated for breast cancer which stunned me – hard not to think of the jabs as being causative but you daren’t say it.
The Vax Control Group *may* produce useful evidence on this in due course.
More likely there’ll be confounding variables which are common in medical research.
But we can hope …
Everyone on here should consider joining.
and there is also this survey being done link to which can be found here:
PROVES study to find out if the vaccines are “safe and effective” (substack.com)
‘Plausible deniability’ was built in to the clot-shot recipe.
More anecdote. An acquaintance told me of two friends in their 50s who had keeled over with heart attacks unexpectedly in the last couple of weeks. He was completely unaware that the vaccine had been implicated in increases in heart related problems, and was a little shocked
know the feeling AYM – it is like walking through a minefield
The question that the caring MSM, the Members of Parliament who believe they are there to serve, the supposed health care community who care about their patients health should now be asking is why this data combined with yellow card reports clearly shows that these products do harm, but they are all silent, they continue to take the money and shut up and support the administration of the death shot, and collect the proceeds from their support.
and the GP’s continue to administer it without doing this kind of research first
In the last couple of days several people have told me that although vaccinated people are getting infected it’s still the unvaccinated that are taking the hospital beds! Can anyone direct me to some simple data or articles that I can use to show this is not the case. In fact I don’t mind complicated data if it can help me argue back. I’m so disappointed in some of my friends and contacts as it seems they are just desperate for restrictions to come back.
Table 11 of the UKHSA vaccine surveillance report (https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1061532/Vaccine_surveillance_report_-_week_11.pdf) clearly shows that the vast majority (>85%) of the hospitalisations in those aged over 18 (children are ‘complicated’) are in those that have been vaccinated.
Many thanks – I’ve now reached the stage where I want to print off these tables and stick them on the walls of my bedroom – like I did with my David Cassidy posters!
I don’t get the downvote here — the stats are official. Everyone is tested on entering hospital and so this isn’t based on ‘samples’. I put a link to the reference — you can count them up yourself. I welcome people arguing their point but a simple downvote is just stupid.
I enjoy the camaraderie on here immensely but the cowardly downtickers are a bloody nuisance.
They are, as you say, just stupid. Feel sorry for them because they are deficient.
Probably a case of ‘fat fingers’ ie someone scrolling through and not noticing they have hit the button.
I’ve done it on threads and caught myself so that I could reverse it, but probably missed a few.
Thankyou for the work.
Have to try table 11 on my wife who remains a true believer.
A song for the triple vaccinated, courtesy of tv miniseries The Pacific.
To the tune of Happy Birthday:
How f****d are you now?
How f****d are you now?
How f****d are you now?
You’re surely f****d now!
Callous, perhaps, but let’s not forget how gleefully the vaxxed anticipated OUR demise not so long ago.
One’s entitled to be worried about friends who foolishly took the first two jabs. They trusted the NHS and some have woken up and realise they were conned. People in the age range 55 to 85 got jabbed pretty early?
The younger you were, the more stupid it was. First, you weren’t at significant risk. Second, you had more time in 2021 to wake up to the risk/benefit balance and say ‘no thanks’ (or just ‘f*** off’).
In most cases, in the friends I know, it was for travel.
The unvaxed can always change their minds later. The vaxed can’t get it sucked out whatever happens.
Darn.
My Thursday sport of plotting the data (Report / 4) to give weekly average. The picture is so much clearer this way
.
..
This comment is specifically for Amanuensis, to give a little comparison. The Dutch authorities provide a lot of data, but not in the same type of detail, so it’s hard to compare. For example, so far I haven’t seen them give death breakdowns by vaxx status.
They started giving data on positive tests by vaxx status. It is updated weekly, but it’s presented as a monthly figure, so you can compare whole months. The most recent data from last Tuesday shows for January that 27% of positives were 3x vaxx and 27% were unvaxxed. Figures for March show 58% of positives are 3x vaxx, 12% are unvaxxed. 1x vaxx is pretty stable throughout (around 4%), 2x vaxxed has decreased somewhat over time – although over that time period one may assume that the absolute number of 2x vaxxed decreased as more people got boosted. So same thing here, there is a definite and substantial increase in positive tests in 3x vaxxed. There has been a slight uptick in hospital/ICU admissions over the last week, week and a half. The government corona dashboard shows a clear increase in people in the age groups 80-89 and 90+ and in ICU in 60-69/70-79 and a sharp increase in 80-89. These groups got boosted first, starting end November.
As for who is testing – larger events still require a negative test (regardless of vaxx status) until next Wednesday, I think it safe to say that the majority of people attending large events (clubs, discos, football matches) are probably in the younger age groups, so I suspect a majority of people testing are in fact those in younger, healthier people. It will be interesting to see if there is sudden drop in postive tests next weekend.
My question here is how many people in the older age groups are normally in hospital with respiratory ailments coming out of winter and is what we are seeing exceptional if we just list them as suffering from a respiratory virus as opposed to the virus du jour?
It doesn’t directly answer your question, but I happen to have some stats on deaths open at the moment: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/monthlymortalityanalysisenglandandwales I’ll be working with tab 11a.
The January 2022 data set shows:
Influenza/pneumonia rate 35.4(per 100,000) vs 72.6 (five year average excluding 2020)
Lower respiratory tract infection rate 53.5 vs 80.1
Ie, death rates for the above (per 100,000) are lower than the five year average by 63.8
The covid death rate for Jan is 79.3. Ie, a bit higher than the reduction in deaths that we’re seeing in other respiratory tract diseases.
Also, do you have a link to those stats?
Thanks for the numbers; it does sort of answer my question, in that although corona deaths may be higher, there doesn’t seem to be too much difference than one might see in terms of people in older age groups dying from a particularly nasty flu doing the rounds.
As for the stats
https://coronadashboard.rijksoverheid.nl
Sorry, I never can copy a link correctly, but that is the address. Speaks for itself, the corona dashboard for the Dutch government. In the top right corner there is the option of clicking on EN, which will present all the info in English. The start page is a summary; for more detailed info, go to the tab ‘national’, right toward the top. Then on the left-hand side you will have options to choose from. I have been taking the numbers for hospitalisations/ICU admissions from the graph at the bottom of the respective pages. It is an interactive graph, you can isolate each age group. I noticed the initial drop in admissions after November and the sudden climb again some weeks ago. There is also a page and similar graph for confirmed cases.
The breakdown of infections by vaxx status is in the epidemiological report that the RIVM/National Institute for Public Health (www.rivm.nl) publishes every Tuesday. This website also has most things available in Dutch and English. The report itself, a PDF, is only available in Dutch.
The numbers are in Table 14 on page 29.
A footnote says the numbers are based on random representative samples, not the actual absolute figures, which in reality are much higher.
Boostervaccinatie afgerond = 3x vaxx
Basisserie afgerond = 2x vaxx
Basisserie niet volledig afgerond = 1x vaxx
Niet gevaccineerd = unvaxxed
Fig. 11 on p. 30 presents the confirmed cases by age group in a chart.
If you do look at this pdf, which is very long and has a lot of info and there is something that you think might be of interest to you, let me know and I’ll translate it into English for you.
By the way – they first started handing out the booster on 18 November. There was a fairly sharp drop in admissions to a low at week ending 26 December. From around 9 January onward admissions in the higher age groups have been heading steadily up, supporting your view that the poke only provides some temporary protection, and for the rest seems to be merely postponing rather than eliminating the further progress of the virus.
Amanuensis, has your ‘3 months of trial data was enough to approve the jabs‘ stance changed since the first Pfizer data release?
3 months of trial data was never enough to approve the jabs other than for short term experimental authorisation in those most very vulnerable to the disease. It was no-where near enough data to support use in non-vulnerable groups (it is arguable where the point of ‘non-vulnerable’ is, but certainly healthy and under 65 or so isn’t that vulnerable to covid).
I strongly suspect that if they’d done the trials properly (ie, independent trials in each country and allowed to identify longer term effects) the vaccines wouldn’t have ever been approved. The absolutely dire short term performance of the vaccines is enough in itself (protection waning over a 3 month period don’t just show them to be not-fit-for-purpose but actually raises questions about what they’re doing to the immune system anyway) let alone the underinvestigation of vaccine side-effects/complications.
Taking the data in table 13 Page 45 of the HSA week 11 vaccine surveillance report (COVID-19 vaccine surveillance report – week 11 (publishing.service.gov.uk) and applying it to a population of triple vaxxed & unvaxxed 60-69 year olds you’d expect 7 deaths amongst the triple vaxxed & 4 amongst the un-vaxxed. In other words, regardless of the size of the population you’d expect 1.75 deaths in the triple vaccinated for every death among the never vaccinated.
For those of you who like to see the table, here’s table 13 from COVID-19 vaccine surveillance report – week 11 (publishing.service.gov.uk) illustrating the point that the triple vaccinated appear to be dying at a higher rate than the unvaccinated.
Sorry Nick, I’m only a GP and stats aren’t my strong point. Your table 13 appears to show that death rates are higher in the unvaxxed than in the vaxxed.
I am a total sceptic and believe the medical gene therapy is causing many many problems, but I always hated stats.
Please enlighten me
Efficacy of shots hits -300% and UKHSA announces it will no longer publish data. That’ll be correlation not causation, no doubt.
When I was reading this this morning I thought my experience bears it out – unvaccinated and just can’t seem to catch Covid.
However, I did notice a bit of a sniffle today. Did a lateral flow test and … positive! I thought it was never going to happen.
Assuming it’s a true positive, I’ve already priced in death as part of the Ts&Cs of living on this planet. However, while being prepared for the worst I’ll assume the best.
It would be a nice feeling to know I’ve got natural immunity, if and when travelling restrictions are fully lifted. It’s better to get the first hit at home.
‘Did a lateral flow test and … positive’
Are you hoping for a boy or a Cold?
A cold. But if it’s a boy I’ll sue the manufacturers of the “Rapid Antigen (Lateral Flow) Test” equipment.
PS. If I never comment again, it’ll either be because I’m dead, or because I can’t take any more of those captcha challenges when logging into The Daily Sceptic. Or else because it was a boy.
I know – today’s felt like it was a kind of trick question on some kind of intelligence test.
I was asked to identify “bicycles” when all the picture showed was motorbikes – were they waiting for me to fall for that one and when I didn’t I got admitted?
Save yourself buy lemsip!
This piece elicited a chuckle.
A dark, cynical chuckle.
Thank-you for your service.
All this is just twaddle as long as the PCR Test or Lateral Flow Test are described as ‘cases’.
What we need is diagnosis of infection by symptoms and presences of antibodies; ‘cases’ defined by the foregoing plus hospitalisation, deaths – those hospitalised and properly diagnosed.
I think the numbers would be very small.
Given the reliance on testing, could the high incidence of ‘cases’ among vaccinated and triple vaccinated be a result of these anal retentive having themselves tested every five minutes, whereas unvaccinated people are mentally normal?
But don’t worry, the 4th and 5th booster will definitely work, and if they don’t, the UKSHA won’t tell you about it, comedy at its finest.
If they won’t then, sorry, but what are they for and should they continue to get government funding???
“It would be useful if some research was undertaken in this area.” There are an awful lot of areas of Covidworld where a spot of research would be useful. For two years I have wondered at the paucity of useful research.
a most excellent analysis, but nevertheless fraught with hazard because understanding of the PCR and asymptomatic transmission frauds informs inevitable degrading of every derivative statistic.
Thanks for this report. UK public health agencies continue to argue it’s inaccuracy in knowledge of the number of unvaccinated that causes it to appear the vaccinated have a higher risk of COVID infection.
But with millions of vaccinated and unvaccinated the simplest of random surveys could answer the question to an extremely high degree of statistical accuracy. Yet months after seeing this signal in the data no public health agency has done so.
It’s just maddening. This is clearly THE most important thing to find out if the vaccine is actually damaging our immune systems and the public health agencies make no attempt to find out the answer even though it would be quite easy to do so.
It’s quite clear they don’t want to know what the true answer is.
Robert Clark
By the way, the CDC in the U.S. has not been as forthcoming on the data for hosp./deaths for the vaccinated as in the UK: they have admitted not providing the real numbers. See discussion here:
CDC giving incorrect numbers for vaccine effectiveness against hospitalizations and deaths.https://clarkr.substack.com/p/cdc-giving-incorrect-numbers-for?s=r
When you suggest the booster is providing some protection against hosp./deaths in the UK data, remember these lag infection rates and the booster is waning just as the 2nd dose was. Within a few months the booster will also show negative efficacy against hosp./deaths.
This reminds me of a severe flaw in how this data is presented. It’s given after a certain time, in weeks, after vaccination began. But clearly that obscures how long it has been since an individual has been vaccinated, since some people may have been vaccinated earlier and some later. So the data should be presented in accordance to how many months someone has been vaccinated.
Done that way it may already show the booster negative efficacy against hosp./deaths.
Robert Clark
I think the jab is very successful. It’s doing exactly what it was meant to do……kill off the population. Those who keep insisting on their boosters will go in to contract other horrible diseases like cancer, stroke and heart attacks. We know this because there is a rise in these. I think the real comparison should be those with three or more jabs who are dying with cancer in particular.
I have noticed a significant increase in lung and liver cancer in my neighbourhood. However, we have bern conditioned to accept that this is due to lack of testing over the last two years……. Don’t you believe it!! Let’s start doing some real investigative work.
“…so it’s surely time to just accept Covid as another type of cold that’ll give us all an annoying sniffle every couple of years.”
Just to remind readers that this is exactly what I predicted almost exactly two years ago in my poem “Pandemic Polemic” which was later kindly reproduced on the Daily Sceptics site.
A voice then crying in the wilderness… might I be the Galileo of 2022?
One possible hypothesis is this: the vaccines protected well against previous variants, especially Delta. They don’t work against Omicron. (Even the government admits that Omicron evades them to some extent.)
So the unvaccinated are much less likely to have caught previous variants. Those who caught previous variants now have the broad spectrum protection that is provided by prior infection. Therefore they are less likely to catch Omicron.
The vaccinated on the other hand were protected against previous variants, so don’t have that broad spectrum protection and are more likely to get Omicron.
I should have said “the unvaccinated are much more likely to have caught previous variants”.
Witnessing plenty of covid here in Devon. Ages ranging from 18 – 80. All adults triple jabbed. Some admitting they had covid when it first appeared on the scene, but this time it is worse. Some of our elderly friends quite ill. Elective surgeries cancelled making room for….you already know.
Why isn’t ivermectin available for those who would like to take it for the early treatment of covid? Instead, the Uk is ramping up their vaccine program to give a fourth jab, despite the failure of the first three jabs. Immune systems being affected negatively? It sure looks that way.
by the way, which scientists are now advising the government since sage has been dismantled? Anyone know? Burying data is never a healthy sign, who exactly made that decision. Worrying times ahead for a gov’t that lacks clarity, honesty and integrity.
IVM is not “approved” because it would be a de facto pre existing treatment therefore scuppering the “vaccines “EUA” application status – they would never have been approvable , certainly in the US ( re. Dr Peter McCullough and his experience on drug trial safety boards); I believe the same is true in the UK/EU but do not have any reference that I can remember!
If you look at the ONS deaths data, you will see a persistent number of excess deaths >400 at home. To date there have been 4473 excess deaths in 2022 at home.This was raised last year by UK Column. It is concerning and probably is a reflection at both the poor health care provision + possibly fear of hospitals.
I must confess I know so many people who have had Omicron, but I don’t know anyone who has been seriously ill. It’s unpleasant but no worse than a bad cold (which can be nasty but rarely lethal) It is clearly infectious which suggests that it is a novel virus. But it’s also clear from the data that the vaccinated are at much greater risk of catching it which also suggests that the so called vaccines have harmed people’s immunity.
My colleague says he felt much worse after a Friday night out…it’s propagnda
Hi, a new user here. Thanks for this data analysis.
Could you please explain the reasons why the UKHSA report keeps emphasizing that the raw data “SHOULD NOT” be used for calculating vaccine effectiveness (p. 37-39 of the report you link to)? Why is this not possible according to them, and why do you think it is right (as your figures above show). The difference between effectiveness data in the first pages of the report and the figures above is huge…
Many thanks, a confused reader.
Easy. Because they reveal the appalling truth of the death jab campaign.
Could be, but that’s not what they say. Instead, they give a host of reasons of which I’d like to understand better whether there’s any statistical sense to that. Telling a friend who normally believes MSM that they simply suppress the truth isn’t nearly as convincing as being able to tell them why the maths/arguments don’t add up.