
The age distribution of non-Covid excess deaths in the U.K. and Denmark in 2021 was skewed heavily towards the elderly – the very group, of course, that all the Covid restrictions and vaccinations were meant to protect. Importantly, this means that any calculation of vaccine mortality rate needs to allow for the concentration of excess deaths in older people. Once this is taken into account, the estimated vaccine mortality rate in the over-75s exceeds one in 1,000 doses or 0.1%.
Following on from my recent article, which examined the correlation between cumulative vaccine doses and cumulative non-Covid excess mortality (NCEM), I further examined the age distribution of those fatalities.
One reader of my earlier article pointed out that in the Danish data there was no excess mortality in 2021 for any age group below 60. This seemed significant, so I examined the U.K. data to see if there was a similar trend, and found there was, albeit not quite so marked as in the Danish data
Below you can see the 2021 non-Covid excess mortality data from both countries, presented as percentages of the population for ease of comparison.
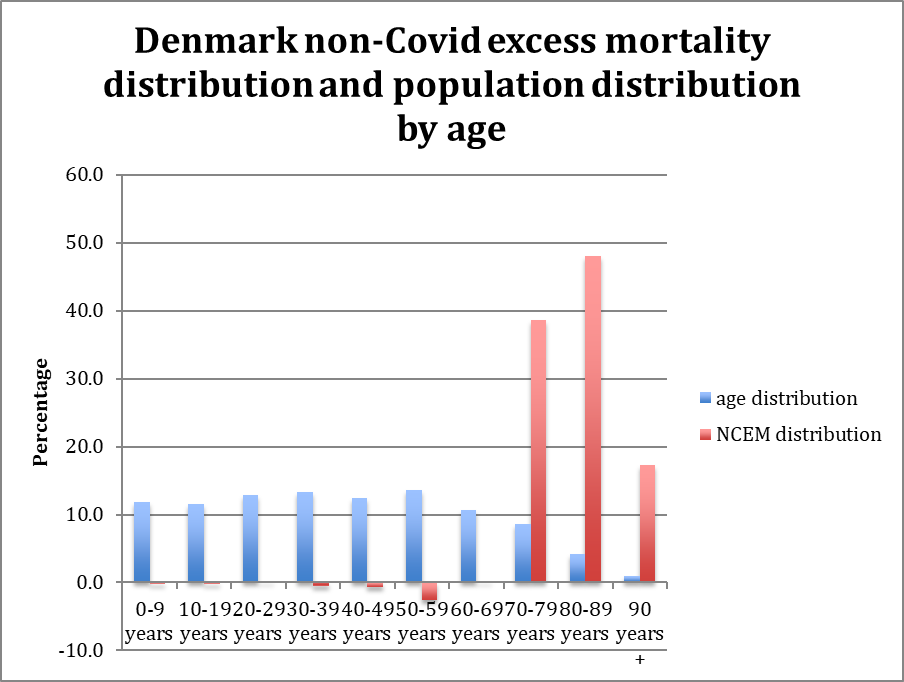
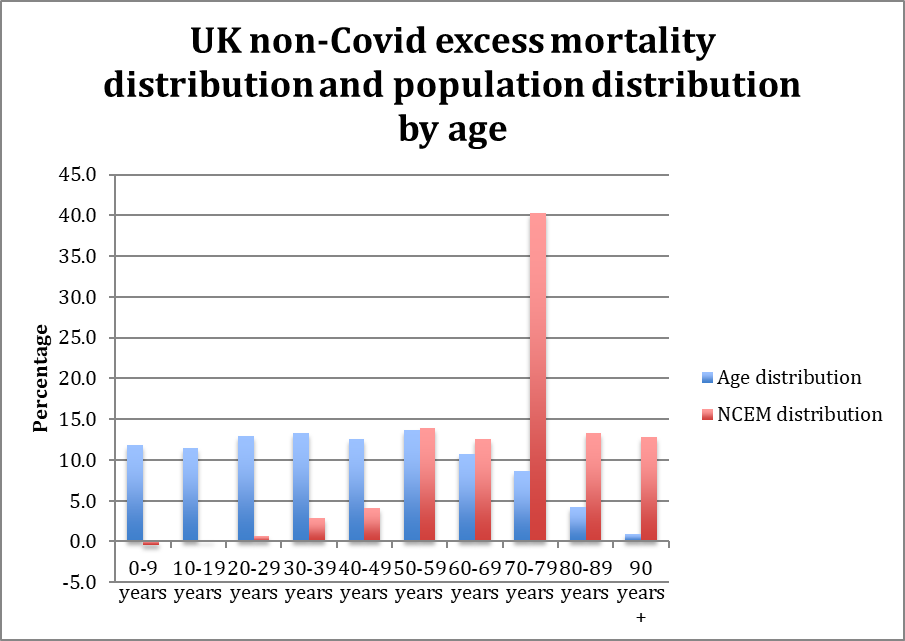
The Danish and U.K. mortality data here are the same as those used in my previous article, i.e., adjusted to account for mortality displacement, the absence of flu and the overcounting of Covid deaths. The ONS publishes the age distribution of Covid deaths in England and Wales and in calculating non-Covid excess mortality I have assumed that the same approximate age distribution holds for the U.K. as a whole and for Denmark.
When we look at the U.K. data, it can be seen that the proportion of non-Covid excess mortality in an age cohort is approximately inversely proportional to the proportion of the population in that age cohort, so that as the size of the age cohort reduces with advancing years the proportion of excess deaths in the cohort does not reduce. A reason for this may be that in the younger age groups vaccine injuries may be much less likely to be fatal. The age breakdown of death reports to VAERS, with a preponderance in older people, supports this suggestion. Note there is a particular spike in the 70-79 age bracket above which has not yet been explained.
The U.K.’s current spring booster campaign, targeted at the over 75s, provides us with an opportunity to test the hypothesis that vaccines are largely responsible for non-Covid excess mortality by predicting the NCEM rate from the vaccine dose rate.
The analysis in my previous article implied there were around 37,000 excess non-Covid deaths in the U.K. from the start of the vaccination campaign to April 2022, during which about 140 million doses of vaccine had been delivered. This produced a headline rate of one death per 4,000 doses or 0.025%.
However, now we see that the over-70s, who represent just 13.7% of the U.K. population, accounted for 66.3% of the non-Covid excess mortality in the period. According to NHS vaccination data, this cohort received around 22.7 million vaccinations in 2021, meaning the vaccine mortality rate for this age cohort is estimated as one death per 925 doses or 0.108%
This allows us to predict that the 3 million fourth doses administered so far in the spring booster campaign would produce 3,250 non-Covid excess deaths for England alone.
The latest ONS data show over 4,000 non-Covid excess deaths in England and Wales in the last four weeks, meaning this prediction seems to be easily on target so far.
While we do not have mortality data by vaccination status to check the hypothesis (and the data from the ONS on this are not reliable), there is clear evidence that many more non-Covid hospitalisations are occurring in the vaccinated than in the unvaccinated.
The Government needs to release the full anonymised data on all deaths since the vaccine rollout began so these concerns can be properly investigated, including by people not invested in the Government narrative.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
You could argue and I would, that large events should have only shutdown for a few weeks. Combining this with a simple screening for healthcare workers and then actually using the Nightingale hospitals with some additional volunteer staff, should have been all that was required.
Indoor events, not outdoor. That is another psy-op.
I read a piece last week about the Cheltenham Festival which got a lot of stick at the time for carrying on just prior to Lockdown 1. because ‘obviously all those people crowded together infected each other’.
It suggested that few people would have cross infected during the festival itself because, as bozo himself acknowledges, the Covid gets blown away by the wind.
But many racegoers would subsequently have gone gone home on public transport and/or spent the evening in crowded pubs, restaurants and hotels thus potentially infecting their friends, other guests and staff at these venues.
This seems to me entirely plausible, in hindsight, though it might not have affected morbidity in the long run.
you can’t get infected in the morning and then infect other people that night …
Might have been infected previously.
Plus, it’s a four day festival with packed bars in the town and on course before and after. Not knocking it (had my biggest win there) but to present racing as purely outdoors is wrong. On a cold, windy day at York there’s often only fifty or so studying pre-parade, the other 20,000 are nice and cosy in the enclosed stands.
To be fair, as a regular racegoer, a substantial percentage never leave the (indoor) bars at all. In recent years racing has become a drinking opportunity with added entertainment.
Not a racegoer so thanks for the information.
The bollocks can be stacked and re-stacked – but in the end, all that needed to be done was to follow the pre-2020 strategies, with a clear emphasis on short-term quarantine for the symptomatic.
Simple.
Greater use of the army should’ve been considered. While they may not have been able to provide specialist nursing care in residential homes they could’ve provided a lot of basic care and would’ve lived in isolation for several months if ordered to do so, whereas civilian staff may not be able to due to child care/family comitments etc. Those staff that couldn’t isolate for long periods of time could’ve been given paid leave while those that could isolate would be paid extra to live in sealed camps with army personel.
It needs stressing that any focused protection for people in the community, especially the provision of hotel rooms would’ve been voluntary to avoid accusations of locking up the elderly. For example people in multi generational households could’ve been offered a room in a hotel knowing that it would reduce their chances of dying, but mean they couldn’t meet with family members. Knowing the costs and benefits of taking up the offer people would then be free to make a choice, and they wouldn’t be locked up as they could return home anytime they wished but doing so would mean they couldn’t make use of the hotel again.
One comment – and not specific to this article. I wish the current trend for always prefacing the disease of Covid-19 with the adjective ‘deadly’ would cease. Yes, it can be deadly as we have witnessed but the use of this descriptor seems to imply that it is deadly more often than not and this just isn’t true. In the majority of people it is not deadly. After all flu can be deadly, a cold can be deadly in a very frail, elderly person, cancer can certainly be deadly but we never describe these illness as deadly flu or deadly cancer. It seems to me to be part of the psychological weaponry that has been used, so effectively sadly, to keep people fearful. I have noticed that even those who should not fall into this trap are using this phrase and I think it’s time they stopped.
“Another measure that makes a great deal of sense is telling symptomatic individuals to self-isolate at home.”
Given the fact that so-called ‘asymptomatic transmission’ has never been proven, surely the simple message of telling the unwell to stay at home should have been done from the start, rather than forcing all of us to mask up.
Given the Diamond Princess evidence, there would have been so few actually affected by the Virus in comparison with the blanket withdrawal of health care for 95% of the population:
“Diamond Princess cruise ship provided a perfect petri dish experiment with the infection. The relevant bit from the Wikipedia entry is:
During a cruise that began on 20 January 2020, positive cases of COVID-19 linked to the COVID-19 pandemic were confirmed on the ship in February 2020. 712 people out of 3,711 became infected (567 out of 2,666 passengers and 145 out of 1,045 crew), and 14 people, all of them passengers, died. At the time, the ship accounted for over half the reported cases of SARS-CoV-2 outside of mainland China.
So out of 3,711 people only 712 became infected (a 19% infection rate among a population in close proximity with each other and sharing the same dining rooms, air conditioning etc.) and of those infected, 14 died for a death rate among those infected of 1.966%. Bear in mind that the passengers were likely elderly (to afford such a cruise) likely to have pre existing conditions (high blood pressure, diabetes, heart and circulatory conditions and other age related factors etc.). But set that aside and note that 14 dead out of 3711 is a 0.377% death rate. Sad for the people concerned but compared with a normal flu season, it is a rounding error.
Similarly, worldwide, there have been a claimed 2 million dead. TWO MILLION DEAD!!!!!! TWO MILLION I TELLS YA!!!!!!!. Which, taking the world population as 7 billion means a death rate of 0.02857% or one person in 3,500. Hardly what I would call either a highly infectious disease or a disastrous death toll. Compared with the numbers of people dying every day of diseases such as malaria, measles etc it is trivial.
So where is the evidence that this virus is highly contagious & has a high mortality rate. All I can see is that the various governments have continued to count anyone dying with Covid (not “of Covid”) or tested positive within the last 28 days as a Covid death, even if they died in a car crash, were shot or some other cause of death. Just like Chicken Little claiming that the sky is going to fall and kill everyone, they are maintaining the panic for their own ends.
The Governments of the world have also not “closed the book” on the last Flu season but continue to total up the numbers from the first occurrence, which they do not do with the normal seasonal flu. We might as well go the whole hog and total up all the deaths from Flu from the 1918 outbreak and claim that ZOMG!!!! Flu is so lethal that we must shut the entire world down in perpetuity. It makes as much sense as counting every single death of anyone over the last year regardless of the true cause of death.
And where are the deaths from ordinary, seasonal influenza? Odd that no one has recently died of that cause, eh? But the governments have fudged the figures so much that we will never find out the truth.
As for vaccines, then the politicians have conveniently forgotten the Nuremberg protocols – one of which is that you cannot administer drugs or vaccines to humans unless it has been tested on animals first or perform medical experiments on people without their consent. Jews for some inexplicable reason are not considered to be animals and are broadly defined as human (the world needs a sarcasm font, right enough). Another is that you cannot rely on “I vuz only obeying zer orders” when committing crimes against humanity. So forcing people to have a vaccination using an untested vaccine and commanding doctors to “obey orders” to do so … Can I call them Nazis and be done with it?”