Recently, Anthony Brookes, a Professor of Genomics and Health Data Science at the University of Leicester, wrote a piece for the Daily Sceptic arguing that central to the virus’s surge-and-decline behaviour is the emergence of new variants, which are “able to infect (or re-infect) some fraction of individuals”.
He writes:
A series of SARS-CoV-2 variants have arisen, many of which possessed a transient selective advantage that led to a wave of infection that peaked some three-to-four months later. Several such variants have spread globally, though different successful variants have arisen simultaneously in a number of countries. The result is a three-to-four month wave pattern per country, which is also apparent globally.
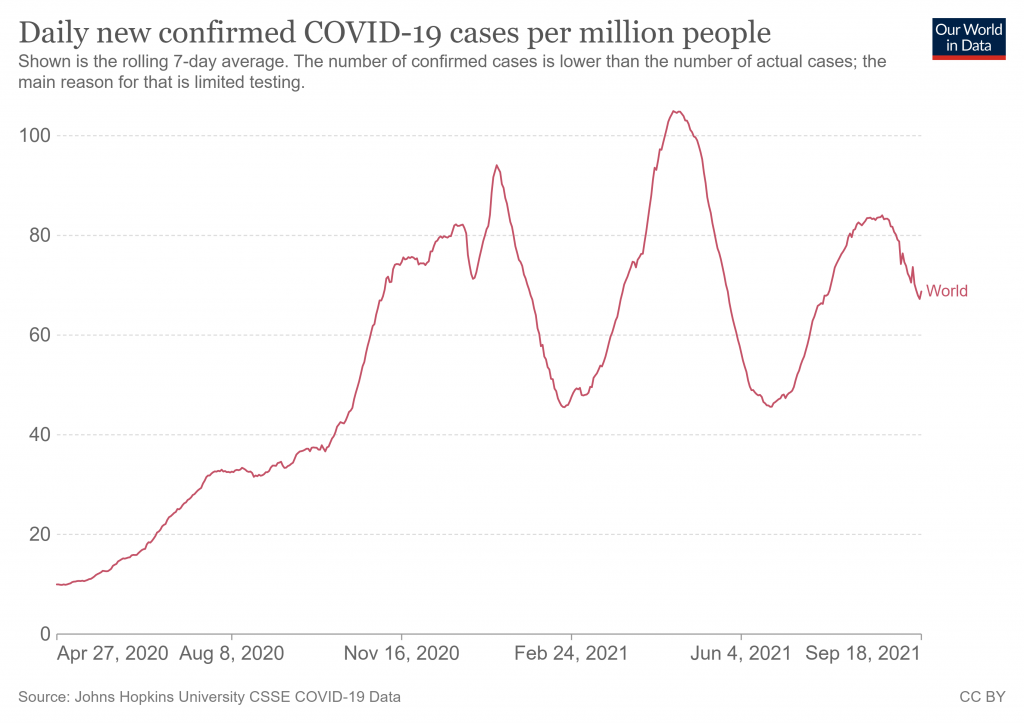
The global wave pattern is shown below. It features an extended autumn and winter wave, a spring wave and a summer wave (seasons here for the northern hemisphere, of course). Note that this graph is raw positive test numbers so does not allow for increased testing.
To illustrate how this global pattern is reflected in different countries and how it relates to the emergence of new variants, I have superimposed the graph of variant proportions over time from the CoVariants website onto the positivity rate curves (the proportion of tests that come back positive, which takes into account changes in the amount of testing) from Our World in Data. I’ve done this for the 12 countries which have done the most sequencing of virus samples (according to CoVariants), plus Israel and South Africa.
Note that the sequencing data is not necessarily representative, though the more sequencing that is done the more likely it is to be representative. Jagged lines in early data indicate small samples that are unlikely to be representative. Grey areas are unidentified variants.
My apologies that it is difficult to read the dates along the bottom of these composite images but hopefully you can see enough to figure out what is what.
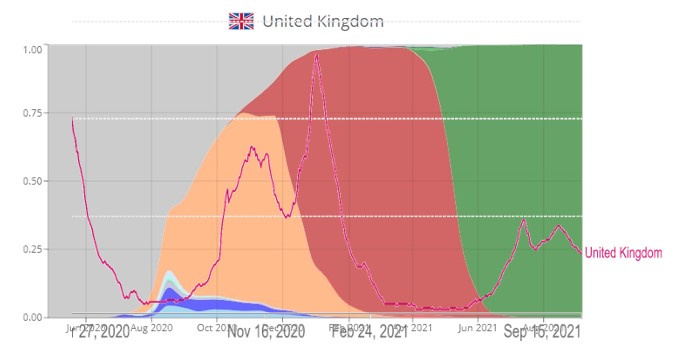
The three peaks in the U.K. are associated with the three dominant variants: the ‘Spanish’ variant (20A.EU1) in orange in autumn 2020, Alpha in red in the winter and Delta in green in the summer. The Alpha surge was large, presumably due to it occurring in the winter. Note the lack of a spring 2021 surge, which in other countries was associated with Alpha.
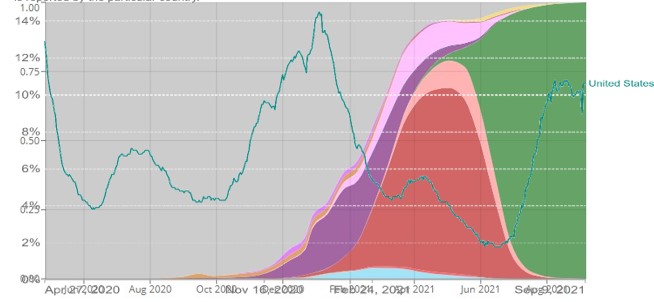
There is evidence in the U.S. of a small spring surge associated with Alpha and a larger summer one associated with Delta. There is no data here on the variant(s) associated with the large winter wave or the smaller summer 2020 surge.
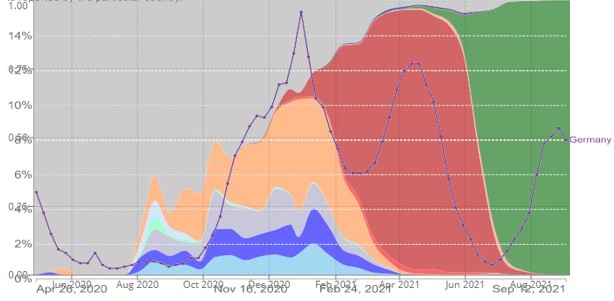
The Spanish variant is significant in the large winter surge in Germany, but is not dominant on this data. The spring surge associated with Alpha and the summer surge associated with Delta are present again.
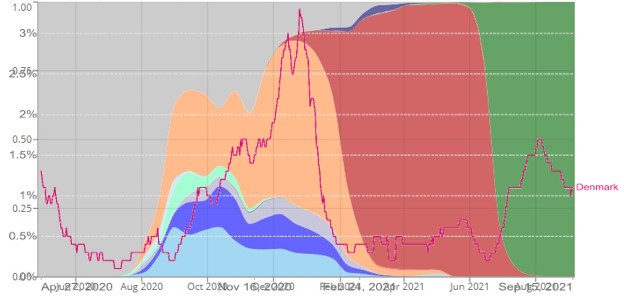
The large winter wave in Denmark is associated with the Spanish variant, though again it is not entirely dominant on this data. The spring bump associated with Alpha is there but very small, while the summer surge associated with Delta is more pronounced.
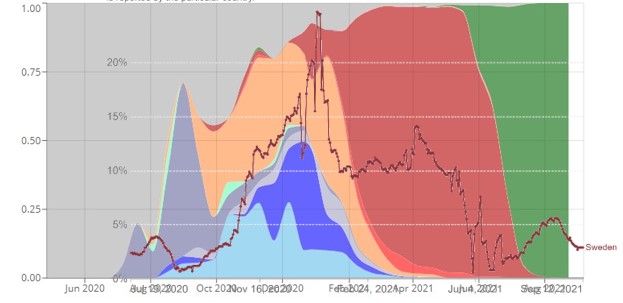
Sweden’s large winter wave was mixed variant-wise, though data at this point was sparse (indicated by the jagged lines). Alpha is associated with a slowing of the drop-off from winter and a second peak. Delta so far in the summer is associated with only a small ripple.
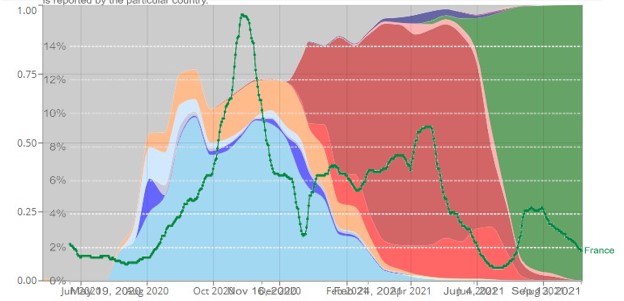
France’s large autumn surge was mainly associated with the ‘French’ variant (20A.EU2) in light blue, though again it was not entirely dominant. The subsequent winter peak was very muted, though a spring surge associated with Alpha and a smaller summer ripple associated with Delta are present.
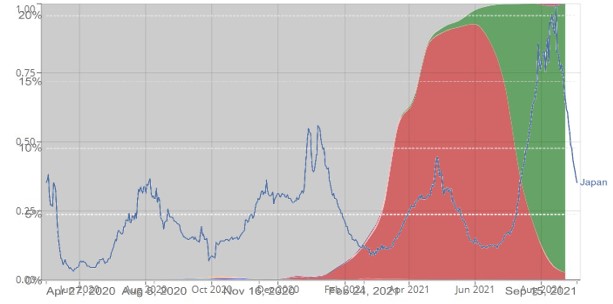
Variant data was sparse before spring 2021 in Japan, but the two most recent surges are associated with Alpha in the spring and Delta in the summer.

The Netherlands’ positivity curve is bumpier than most, but there appears to be a large winter wave associated with (though not dominated by) the Spanish variant, a spring resurgence associated with Alpha and a summer surge associated with Delta.
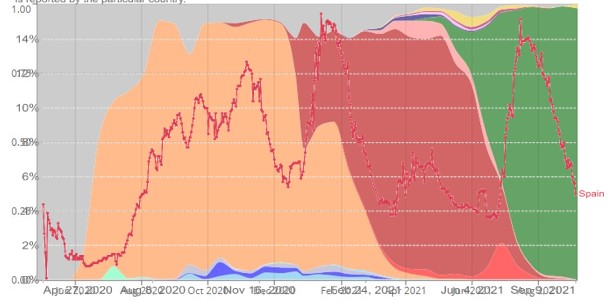
Spain’s autumn surge is dominated by the Spanish variant, but its winter wave seems to be a mixture of Alpha and the Spanish variant, while there is also a spring bump associated with Alpha. A summer surge associated with Delta is clear. Spain is unusual in having four peaks but three dominant variants, perhaps a result of the winter wave occurring just as Alpha was taking over from the Spanish variant.

Canada had little data till recently. While a summer surge associated with Delta is clear, the spring surge is associated with both Alpha and other variants, including Gamma (in pink).
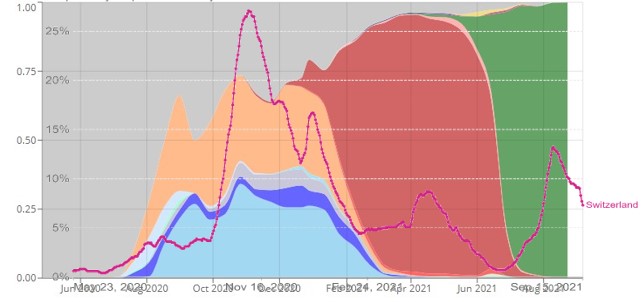
Switzerland’s autumn and winter wave featured a mix of variants, especially the French and Spanish. Alpha is associated with a spring bump and Delta with a moderate summer surge.
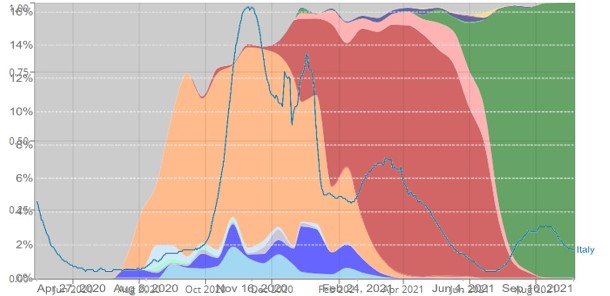
A large and extended autumn and winter wave associated with the Spanish variant is evident in Italy, and is similar to Spain in that Alpha takes over from the Spanish variant during the winter. There is then also a spring bump associated with Alpha and a small summer ripple associated with Delta.
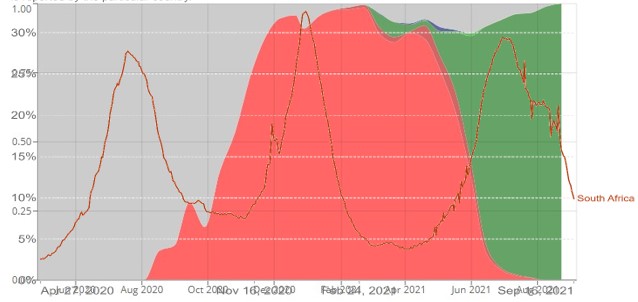
South Africa has not sequenced so many samples as the countries above, but a summer wave associated with Beta (light red) is evident, as is a winter wave (in this case) associated with Delta. South Africa is the only one of these countries where Alpha never became dominant, apparently being squeezed out by Delta.
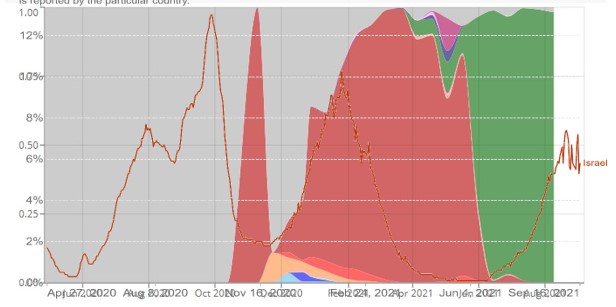
Sequencing in Israel has also been quite sparse, but there is some evidence of a winter wave associated with Alpha and a summer surge associated with Delta. The lack of spring bump may be, as in the U.K., because the Alpha wave occurred over winter.
These 14 graphs illustrate how variants are associated with surges in different countries. Importantly, almost every time there is a surge and a peak it is associated with one of the highly successful variants (Delta, Alpha, Spanish, French). The main exception is in winter, when there is a peak anyway, though even then it is usually associated with these variants in some way.
Importantly, by way of control, the U.K. and Israel show that when Alpha was the dominant winter variant, the spring peak, typically associated with Alpha, was absent.
This is to my mind compelling evidence that variants play a key role in driving new surges of coronavirus. It suggests that herd immunity is to some extent variant-specific, and that a new variant temporarily disturbs the herd immunity until the latest wave of infections tops it up again.
There is no sign yet of the emergence of a new successful variant that will take over from Delta. This holds out the hope that Delta may be some kind of evolutionary endpoint or optimum for the virus, and thus that the autumn and winter may be mild from a Covid point of view – though other viruses like flu may take the opportunity to make a comeback.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
This is very good work and shows the reason for the sudden surges and slumps. We have serially reached saturation (herd immunity) only to see it broken by the next variant.
I suggest watching Sunetra Gupta talking about herd immunity recently on YouTube. It is not a fixed state but a dynamic equilibrium. This is the behaviour of the other 4 corona viruses, so SARS-CoV-2 is no different.
She’s also done a similar presentation on variants which I haven’t watched yet.
Snap
no need to watch gupta. it shows the reason for the sudden surges and slumps. We have serially reached saturation (herd immunity) only to see it broken by the next variant. That’s how it goes.
It’s just more propaganda, using ‘variants’ as a never-ending source of reasons for more lockdowns and other Covid restrictions, and pushing the ‘vaccines’.
If there really was a deadly ‘virus’ and its many Mutants going around, the politicians would be wearing face masks in Parliament and definitely not allowing festivals and football matches to be allowed.
And people would avoid the supermarkets like the plague. Still, people shopping, and no dead people in Aisle Seven in Tesco’s.
I tend to agree with you. All viruses have variants some more transmissible but less virulent, some more virulent but less transmissible, some that are not very transmissible or very virulent; and in the past we haven’t actually cared about the details of the pathogen.
In the old days (pre-2020!) if I saw a patient with cough or cold symptoms usually without altered breath sounds it would be put down as a viral upper respiratory tract infection, no need to identify the virus or it’s type as it made absolutely NO difference to the management. My advice would be “maintain fluids, paracetamol for any pain, over the counter remedies for symptom control. If worsening or change in symptoms contact own GP, call 111. If very unwell attend A&E or call 999. If no improvement after 7 days contact own GP.”
Now people are attending A&E immediately with colds because they are frightened that they have CoViD19, no thanks to the symptom list resulting from the Tim Spector ZOE app.
Ah yes.. the dreaded Covid symptom list.. I apparently have it as I’ve only £23.74 in my current account..
Interesting that El Salvador’s outpatient covid treatment protocol apparently includes Ivermectin:
El Salvador Minister of Public Health Includes Ivermectin as COVID-19 Pandemic Continues
“The Protocol
Called the “Outpatient Treatment for COVID-19, the protocol includes the following:
MedicinesDose/Duration
Acetaminophen500 MG 1 Tab VO C/6 hours
Loratadine10 MG 1 Tab V C/12 hoursZinc50 MG 1 Tab VO/ day
Ivermectin6 MG 1 Tab VO C/12 day
Vitamin C500 MG 1 Tab VO C/day
Vitamin D2000 MG 1 Tab VO C/day
Azithromycin1 Tab VO C/day”
Vitamins, an antibiotic, an antihistamine and an anti-inflammatory, as far as I can see. Makes sense, but I’m a bit surprised there’s no aspirin.
That is following Peter McCullough’s recommendations, Peter has HCQ as a viable alternative to Ivermectin if available. Also other antibiotics are possible such as nitrofurantine. There were some good studies on antibiotics that seemed to stop the anchoring of the spike on the ACE2 receptor in the summer of 2020. They were all stopped under pressure from big pharma because of the ‘vaccines’.
A lot of people are allergic to asprin, alternatives are available.
Dr Zelenko suggests Quercetin 500mg in countries where HCQ or IVM are not available. Do check if there are any medication interactions if you’re taking any before starting on it. HCQ, IVM & Quercetin act as an ionosphere to enable the zinc to enter the cells.
As does the Zeneco protocol – as does a lot of them – there was a theory a parasite might be involved in the pneumonic stage – whatever works – quercetin is also a great deliverer of zinc to the cells – over the counter au natural – DYI is a sure way to stay healthy
People are attending A & E immediately because the government has not dealt with the scandal of GP’s refusing to see patients.
Snap. It’s a source of cash for some, but it would better to educate the general public about the normality of variations like that. Maybe the term ‘common cold’ has gone out of fashion, but it’s been around for a while!
…our doc used to look at the kid (cough cough sniffle sniffle), roll his eyes and say keep her home for a few days – when I asked what it was – inevitably a non specific virus (just one of them corona viruses all the kids get)… off you go. Halcyon days.
Talking to a believer the other day, who won’t attend his daughter’s wedding because “she has people coming from all over, and the last party she had, seven people caught the CoVid”. I asked, did they die? No. Did they have to go to hospital? No. If this was 2019 and seven people had caught a cold at a party, then got better, would you have even thought twice about it? He walked away, hopefully thinking a bit about how he has been played.
Depends if he’s over 70 with two underlying relevant conditions, or obese, of course.
There is still ivermectin and other repurposed drugs, which would have saved plenty of lives for all those with Comorbidities.
As you say, hopefully.
‘He walked away, hopefully thinking a bit about …‘
That’s a ‘big ask’.
Agreed.. see my post above..
None that I’ve seen!
Sorry, but its not good work. Coronavirus’s always mutate, and those mutations become weaker as they progress. They are easily recognised and managed by a persons natural immune system without the need of outside intervention.
I believe it was Mike Yeadon among others who’ve said these so called variants are so close in makeup to the original virus that in no way would they fool or defeat the immune system. The article is just more hype on the covid lie I’m afraid.. bullsh*t!
Agree, Yeads nailed this and the summer increases in reported CCP Virus was largely mixed up with normal mild summer virus, plus some obvious scamming around schools. People at both sides of the desk, took advantage of Williamson’s absurd rules and took 10 weeks off rather than 7. You can dip a flow test in a lot of liquids and get a positive.
“You can dip a flow test in a lot of liquids and get a positive”.. absolutely.. but those African leaders that do seem to end up dead.. !!!
Water produces a negative.
Yes, I remember Mike Yeadon referred to them as “samiants” because they were so similar.
He’s just saying able to infect those who have not yet had it. “(Or reinfect)” – I take that as a possibility, not a claim. He’s going on positive tests, with no allowance for political increases in testing, and no separation into symptomatic individuals, so it is all subject to Rick’s earlier. general remarks on plaiting.
I do still know some people who have not had Covid yet, but not many. Probably there are still pockets outside the big cities of Covid naive individuals, and quite a few careful elderly folk. I know of a lot of people who got it this summer, some of them twice jabbed. But I don’t know anyone who has got it – with symptoms – twice.
Obviously there was an early case, for example, of an old lady, in Belgium I think, who was reinfected and died, but she was in her 80s with cancer affecting her immune system.
Anyone here know anyone who got it twice with symptoms?
Thanks, yes, I did say that. Theoretically, a small change might alter the ease with which a pathogen infects a person, and the degree to which it can make you ill.
But once your immune system has beaten it away, it’s remembered a couple of dozen unique sequences from that pathogen, leaving you with highly selected T- and B-cell clones capable of rapid responses if you see the same OR SIMILAR viruses in the future.
I’ve checked with Dr Sin Lee & he’s given me the definitive list of changes in the amino acid sequences. We’re still less than 0.5% TOTAL changes since Wuhan.
Its completely irrelevant whether one or two further changes occurred in the spike. In fact, our immune systems, challenged with SARS-CoV-2, tends not to bother making immune memory vs spike protein. Most of the naturally occurring immune memory against other parts of the virus.
So on these grounds alone make it unlikely, from an immunological perspective, that really small changes in the virus will breakthrough any persons immunity, and definitely not break through population immunity.
I don’t think this is correct at all. None of the variants detected so far should evade a normal immune response caused by a genuine infection. If somebody caught and recovered from the vanilla covid virus then none of the variants, including delta will evade the immune system. Delta is only 0.3% different genomicaly from vanilla – the immune system is highly highly unlikely to be defeated from a variation of such magnitude. People in Korea had some immune response to covid from catching the original SARS back as far as 2002 (a 20%+ variation).
The reason the new variants cause a surge may be because they are more transmissible so they infect new people, the re-infections may well simply be people who had an asymptomatic PCR positive – i.e. they never actually had it at all, or they may be very unlucky in that they caught the new virus and it took hold before their immune system caught up.
If the vaccines are leaving people susceptible to a breakthrough infection then that strongly indicates that they are not stimulating a proper natural immune response in the first place. We all had the MMR as children and a booster at 12 and that protection is for life – no fading, no boosters required there remember. The same standard should apply to the covid jabs.
We all had the MMR as children and a booster at 12 and that protection is for life – no fading, no boosters required there remember. The same standard should apply to the covid jabs.
That’s a pretty high bar – other vaccines vary from MMR which is good for life through things like tetanus and diptheria which should be renewed every 10 years, shingles every 5 years, to flu which is recommended annually.
I was told by my GP that 2 shots of the tetanus vaccine with a 10-year-gap, should provide life-long immunity.
I’ve been told at hospitals that I almost certainly didn’t need a tetanus shot after being bitten by a dog, standing on a nail &c several years after my last jab, although they were happy to give me one. I haven’t had a tetanus jab for more than thirty years and have never considered myself at risk.
Tetanus isn’t a particularly good parallel. IIRC, the treatment immunises us against a non-replicating toxoid. In that case, I believe we need a sufficiently high titre of antibodies against that toxoid in order bluntly that we can mop up enough of it to ensure that there’s too little left unbound to cause us to be poisoned.
That is correct , just like a common cold…er, oh wait exactly like a common cold, who would have thought?
Billions of pounds and thousand of lives lost, businesses closed, and children tortured and jabbed, and the ‘experts’ now acknowledge it’s a normal Coronavirus that acts like a common cold!!
Thank God for the experts, what would we do without them?
‘Thank God for the experts, what would we do without them?‘
Keep calm and carry on?
“We have serially reached saturation (herd immunity) only to see it broken by the next variant.”
Not in the slightest.
He doesn’t explain how genetically similar the variants are to the original Sars-Cov-2 on paper. Even Delta is only marginally different, nowhere near different enough for your immune system to have trouble recognising it.
Variants would need to be wildly different, something like 40%+ different genetically from the original to start compromising natural herd immunity.
Tinker with the PCR cycles and you can create whatever seasonal patterns you like. Bogus data for a bogus pandemic.
Yes. I’ve always thought that was what was happening.
Obviously it’s a crucial distinction. If this is what’s happening, the key point is that ITS NEVER GOING TO END. Not unless we end it somehow.
Remind me, how do you know what a case is??? Look at all deaths; there have been no waves, period!
Take a look at ONS all cause deaths by vaccine status, and calculate death from all cause for the vaxxed and unvaxxed.
Except for the waves of deaths around April 2020, and the start of 2021.
In England only, a little bit in Scotchland, and not at all in Wales and Northern Ireland.
https://www.euromomo.eu/graphs-and-maps/
… and in 2018, and in 2017 (as the graph you link to shows), when nobody really noticed. Granted the waves in 2020 and 2021 were slightly bigger than the waves in 2018 and 2017 but the difference between the peaks of the spikes say in early 2021 and 2018 amount to 1 death per 16,000 of the total population, and most of these people were very old.
“Mass Delusion About COVID-19 Death Numbers”
http://participator.online/articles/2021/09/mass_delusion_about_covid19_death_numbers_20210917.php
The initial peak was largely induced through stressful movement of elderly, unwell people from one institution to another. That, coupled with inappropriate treatments, some of which led directly to deaths, I wasn’t there, so I’m not going to accuse all medical staff of deliberately poor care, though later on, I do think they mostly should have known that treatment was wrong.
I do have some insights via pulmonary expert friends in Italy. They were told, directly from China, that the sooner their patients were sedated, intubated & ventilated, the greater the chances of saving their lives.
This so-called “Wuhan Protocol” probably was followed & killed thousands of people. Note that respiratory virus infections rarely lead to obstruction & so mechanical ventilation is rarely really appropriate.
Worse, mechanical ventilation of frail, elderly people often leads to pulmonary injury & makes death much more likely.
Care home residents murdered with lethal doses of Midazolam, courtesy of Matthew Hancock.
Exactly as explained by a person on “the frontline” – John O’Looney, Undertaker in Milton Keynes who stated that during the March/April 2021Care Homes Midazolam DNR mass murder all his call outs were to Care Homes, something he had never seen before in his career.
There is a missing piece from this jigsaw —
Why does it take so long for the covid wave to become established once the new variant becomes present in the country?
According to the SIR model, as soon as the variant mutates it should quickly become established in that country. (SIR — Susceptible – Infected – Recovered — the disease model favoured by SAGE)
Furthermore, it is clear that each covid wave dissipates way before a herd immunity has been reached. Again, according to SIR this is unlikely.
The variants are important in the continuing presence of covid in each country, but the ‘variant model’ doesn’t explain everything.
SIR and SAGE says it all.. we’re talking normal mutations of a corona virus which are weaker than its parent. Now why would the likes of SAGE make a big deal of these mutations.. to keep the scam/fear going perhaps..????
Interesting to read this just after viewing Sunetra Gupta’s recent video piece arguing the opposite – that variants don’t drive numbers, but rather merely follow the basic seasonality.
Professor Sunetra Gupta explains the significance of COVID-19 variants.
Where you have two experts in the field who do not seem to be in hock to a vested interest such as big pharma or government, this is where real science can be done. Each has a suggestion for how things work, and the evidence for and against each can be tested.
There is an inherent problem here in the questionable nature of testing-based “case” numbers, but equally seasonality is being questioned in view of the recent apparent summer surges in the UK and US.
These matters are highly complex and only partially understood, but at least with sceptical-leaning scientists we can have some trust that the underlying motives are honest. Scientists, of all people, should be sceptical of official truth and “consensus” views.
Now map those peaks to the individual countries’ launch of vaccination programmes…..
You mean like a cold
The strange thing about this article is how uncompelling the evidence is for something which is widely accepted. Don’t most people associate the wave last winter with the Alpha variant and the current wave with the Delta variant? The disagreement is over what to do about it. However, the article is full of charts of countries where the wave is only loosely associated with a variant.
The usual confusion of causation with correlation.
Correlation of what?
Assume the premises.
Discuss the details.
Strengthen the narrative.
Yet again you are missing the most important point – WHO FUCKING CARES? COVID19 HAS A SURVIVAL RATE OF 99.97% IN THE UNDER 70S. IT HAS A 99.85% SURVIVAL RATE OVERALL. IT’S THE FUCKING FLU/COMMON COLD. THE TEST CROSS REACTS WITH INFLUENZA AND IS 100% FRAUDULENT AND UNFIT FOR PURPOSE. WE HAVE DRUGS THAT CAN CURE THE SICK. WE HAVE PREVENTATIVE TREATMENT FOR THE AT RISK ELDERLY.
IT’S BASIC MEDICINE USING DRUGS THAT ARE LONG OUT OF PATENT, CHEAP AND WHICH HAVE WON NOBEL PRIZES. HMG HAVE BLOCKED ACCESS TO THESE DRUGS IN ORDER TO PROMOTE THE GENOCIDAL DEATH SHOTS TO FAMILIES AND THEIR KIDS. THE ONLY THING PREVENTING THIS NIGHTMARE FROM ENDING IS THE COLLECTIVE OF PARASITES, DEMONS AND CRIMINALS IN WESTMINSTER AND THE CORPORATE CONTROLLED FASCIST UK GOVERNMENT.
The only important issue now is how we transition from having proven mulitple crimes against humanity have been committed including genocide in the care homes and via prevention of access to safe drugs and attempted genocide via the death shots – which has already been done – to making arrests and prosecuting and sentencing the guilty, which includes the Crime Minister, Bojo the Genocidal Clown.
Professor Dr John Ioannidis the world’s number 1 epidemiologist writes:
Global perspective of COVID-19 epidemiology for a full-cycle pandemic
https://onlinelibrary.wiley.com/doi/full/10.1111/eci.13423
Status of COVID-19
https://www.gov.uk/guidance/high-consequence-infectious-diseases-hcid#status-of-covid-19
In this following interview, Dr Zelenko who formulated the safe and effective COVID drug treatments describes the Israeli government as NAZIS. Great to hear such levels of honesty from someone so respected and qualified.
Dr Pinky interviews Dr Zelenko (Heb Subs)
https://www.bitchute.com/video/irQcKJv0GR2U/
I agree with most of what you say but it’s NOT flu or the common cold, it’s Covid-19 caused by SARS-CoV-2 virus which has been “whole gene sequenced” over 3.2 million times and is different in it’s genome to other coronaviruses.
The PCR test is very accurate and does NOT detect different viruses it only detects SARS-CoV-2. The fraudulent side of the PCR test is the governments unwillingness to take into consideration the different CT rates of a positive result most of which won’t be infectious.
Indeed, before anyone starts ranting about false positives, consider that from 208,730 tests in August and early September 2020, only 159 were positive.
Even if they were entirely false, that’s still 99.92% specificity.
Receipts: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/methodologies/covid19infectionsurveypilotmethodsandfurtherinformation#test-sensitivity-and-specificity
Tinker with the PCR cycles and you can manipulate the data at a stroke.
Then the next week, the conditions can be changed & your assumption about the operational false positive rate is blown out of the water.
No one inspects the SOP & assures us that good laboratory practise is being followed. Neither the facilities nor the workers are properly certified. Initially, testing was done across 40+ NHS & public health laboratory services, but in summer 2020, it was all swept out of those well run labs with trained staff & poured into private labs where no one could see what was going on. Since then, capacity has been ramped up tremendously. It’s fake.
I’m pretty sure it has now been established that the test cross reacts with influenza but I forget which source this came from now. Your post is also disingenuous because PCR cannot diagnose anything and can only detect the presence of molecules – it cannot tell you if someone has a live replicating virus inside of them. I’m also quite sure that the NHS now admits it can detect molecules up to 90 days following a so called infection. It is the wrong tool for the job, but great if you want to create the illusion of a pandemic and magic a giant gravy train out of thin air – at the expense of innocent peoples’ health because the swabs are contaminated with all manner of nefarious particles and carconogenic ethylene oxide. The criminal governments have done everything in their power to abuse the test, which points to criminal corruption as opposed to cockup – like everything COVID related. At least some of the the labs are a total shambles as exposed in the famous documentary. The PCR test is part of the scam and it has been exposed as such in court in Portugal and Germany.
Allow PCR expert Professor Ulrike Kammerer to explain:
Prof Ulrike Kämmerer : Doctors for Covid Ethics Symposium – Day 1
https://www.bitchute.com/video/YwCYrYUBmINa/
Many issues with the PCR scam exposed here:
Review report Corman-Drosten et al. Eurosurveillance 2020
https://cormandrostenreview.com/report/
And for the vast majority, COVID19 really is little more than the common cold or most commonly – absolutely nothing at all
Antionietta Gatti | Analysis of Covid Test swabs | Planet Lockdown
https://www.bitchute.com/video/TrkiY1ZMXlo3/
No the PCR test doesn’t detect influenza and you won’t find a reputable scientific study that says it will.
The PCR tests for genes specific to SARS-CoV-2 not molecules.
I have already stated the CT rate determines whether the virus is likely to be “live” or not and if it is “live” then in many cases it can be replicated in the lab.
PCR expert Professor Ulrike Kammerer supports the PCR test but is cognisant of “handling procedures, underlying test protocols, and analytical reagents” in wet labs.
Eurosurveillance totally rejected that report which is full of flaws. The Drosten et al test was quite accurate but has since been improved.
Yes Covid for many is no worse than flu as I have had it myself.
Again I agree with where you are coming from but factual accuracy is paramount if we are to fight against the propaganda.
So the test is specific to SARS COV 2 apart from Tanzanian goat and pawpaw swabs. Or was that just the tests in Tanzania, but all the rest of them like the ones distributed in Europe (apart from the ones that test positive when dipped in Coca Cola), they’re the proper ones, none of your rubbish, and they ONLY react to SARS COV 2 and Tanzania got some bad batch but they had to assassinate Magafuli anyway because of Long Covid which can be really nasty especially if kids get it?
Goat and pawpaw ‘test positive’ for COVID-19 in Tanzania
https://www.youtube.com/watch?v=s4p8DM8rKJI
The accuracy and specificity of the PCR test is well documented by peer reviewed scientific research.
I cannot vouch for the veracity of something you may have seen on YouTube.
You are promoting a device which is being used fraudulently – the PCR test which forms a central part of some very high level legal challenges which are being brought and which has already been exposed as fraudulent and not fit for purpose in court as featured in articles on this very site. The device is being used illegally by these criminals – abused to con billions of people into believing in a clearly criminal agenda. You are lying and attempting to deceive people out of their freedom. But you have been rumbled and every point you have made has been destroyed. So you resort to type and continue lying and promoting falsehoods. I purposefully posted a video by Reuters, confirming the story of how the President of Tanzania showed the world that the PCR tests were a total fraud by swabbing goat, fruit and motor oil which came back from the lab showing positive.
Here is that interview:
President of Tanzania: Paw-paw, goat and Kware (quail) test positive for Coronavirus.
https://www.bitchute.com/video/yxsMmiTnuAaq/
Weimar Court Prohibits Mask-Wearing, Distancing Measures and Rapid Testing At Schools
https://dailysceptic.org/2021/04/14/weimar-court-prohibits-mask-wearing-distancing-measures-and-rapid-testing-at-schools/
Interestingly, John Magafuli the President of Tanzania is now dead because he exposed the scamdemic and the judge who ruled against the PCR tests and masks in Weimar had his property raided by the police and his possessions confiscated. This is the world you are helping to build with your lies.
German judge investigated by police after ruling compulsory mask-wearing in schools unconstitutional
https://ukhumanrightsblog.com/2021/04/28/german-judge-under-police-surveillance-after-ruling-compulsory-mask-wearing-in-schools-unconstitutional/
UPDATED: President Magufuli dead at 61
https://off-guardian.org/2021/03/18/discuss-president-magufuli-dead-at-61/
The PCR test is not fraudulent.
A handful of people had doubts about it and instead of writing a scientific paper for discussion and peer review they set up a website condemning it. Members of the public in their millions who don’t understand modern virology fell for it.
Their doubts were sent to Eurosurveilance who after review dismissed their complaints as groundless.
The PCR test works very well up to about a 36 CT rate. If you carry on testing after about 50 amplifications it’s no surprise that a variety of organisms tested positive.
The German case you linked to confirms what I have been saying all along in that the PCR tests very well for SARS-CoV-2 genetic material but doesn’t confirm whether the person is infectious or not. That can only be confirmed by a lab test to see if the genetic material can infect another organism.
You are determined to ignore the fact that the PCR test, in almost every case, is being misused.
Firstly, it´s designed to confirm diagnosis of someone with symptoms and is not to be used on its own as proof of infection.
Secondly the number of cycles used (36 to 45) will produce false positives in up to 97% of cases according to Mike Yeaton. Inerestingly, it´s now being used at 24 cycles – the recommended amplification – in the double vaccinated…….
It has two uses (like many tests).
In conjunction with symptoms and other aspects of patient history for diagnosis.
By itself for screening and tracking the epidemic. There will be a certain number of false positives (and false negatives) but contrary to popular rumour and Mike Yeadon (if he really said that) the specificity is actually very good so the number of false positives cannot be excessive. The proof of this is that during the summer we are doing 2-3 hundred thousand PCR tests a day and only getting 2,000 odd positives. The number of false positives cannot exceed the number of positives!
I’m not ignoring that fact at all. Yes it is being misused by ignoring the CT rate which in 85% to 90% of cases the person is not infectious.
Positive results rarely go above 36 according to the data from the ONS Infection Survey.
I again agree with you that the unvaccinated are given a higher CT rate than the vaccinated to make the experimental jab look better than it is.
As I understand it, the SARS-CoV-2 virus was “detected”/isolated by taking entirely hypothetical primers (previously existing genetic sequences from gene banks) and putting them in touch with the supernatant of the pharyngeal fluid of an “infected” patient, that is with billions of RNA and DNA molecules. The primers then attached to something thing in that broth and as a result the conclusion was that whatever attached to those primers then forming a DNA molecule with the help of the enzyme reverse transcriptase was/is the “new” and unknown SARS-CoV-2.
The primers used were only an infinitesimal fragment of the alleged genome (18 to 24 bases – nucleotides – each; while covid is assumed to have 30,000 bases ie 0.07% of the genome
How is it possible to select the virus you look for with such a minute sequence – and from a sea of billions of molecules?
I am in no way an immunologist/virologist but the above is a distillation of matters which greatly trouble, let us say, independent experts in the field.
The computer programmers then take this over as fact and any deviation from the – predicted programme? = mutation.
SARS-CoV-2 is very similar to SARS where virologists had the complete genome.
The first initial gene sequence did in fact just detect the first and last bases and a computer programme filled in the rest.
However, since then the full 30,000 bases of SARS-CoV-2 have been laboriously “whole gene sequenced” many times around the world. To date virologists have taken over 3.2 million human samples of the virus, gene sequenced them using different types of machines and uploaded the results, which are all the same gene sequence (apart from the variants) to the GISAID Initiative.
Viruses are complex entities smaller than the wavelength of visible light (400-700nm) which are only evident when they attack another cell and therefore virologists have always known they cannot be “isolated” in the dictionary sense of the word.
If you have a million human cells without a virus and one human cell with a virus then Virologists are happy that they have “isolated” the virus in scientific terms.
“it only detects SARS-CoV-2.”
No it doesn’t. It detects a possibly related RNA sequence.
The gene sequence of SARS-CoV-2 is unique and the only other virus near it is SARS.
Influenza only has 13,500 bases whereas SARS-CoV-2 has 30,000 bases.
The PCR test will not detect other viruses.
“whole gene sequenced”
Using PCR to identify genetic fragments and claim they’ve found it?
No lab worldwide has isolated Sars-Cov-2 from an infected person and placed it on a cell culture to replicate more. It only exists as a digital virus on computer hard drives.
You really need to stop listening to Kaufman, Cowan, Bailey, Icke et al and read up on modern virology.
30,000 bases and they use PCR to identify less than 30, then use extrapolation to essentially guess the remaining genome and claim they found the virus.
How about isolating it the traditional way? They can’t and you can’t show me proof they have because it doesn’t exist.
The 30,000 bases of SARS-CoV-2 have been laboriously “whole gene sequenced” 3.2 million times in various labs around the world by highly skilled virologists and technicians.
Viruses are complex entities smaller than the wavelength of visible light (400-700nm) which are only evident when they attack another cell and therefore virologists have always known they cannot be “isolated” in the dictionary sense of the word.
If you have a million human cells without a virus and one human cell with a virus then Virologists are happy that they have “isolated” the virus in scientific terms.
You really need to stop listening to Kaufman, Cowan, Bailey, Icke et al and read up on modern virology.
3.2 million copies of the same technique to prove something exists that doesn’t?
The original SARS virus has been cell-culture isolated in a lab years ago, so why can’t they repeat the process for Sars-Cov-2?
You really need to stop being a patronising arse wipe, facts are facts and you don’t have any.
Here’s a quote from the CDC: “Positive results are indicative of active infection with 2019-nCoV but do not rule out bacterial or co-infection with other viruses.”
Here’s one from the British Medical Journal December 21st 2020:
“The only test for live virus is viral culture. PCR and lateral flow tests do not distinguish live virus. No test of infection or infectiousness is currently available for routine use. As things stand, a person who tests positive with any kind of test may or may not have an active infection with live virus, and may or may not be infectious.”
They have cell-cultured SARS-CoV-2 many, many times and shown that it can infect another human.
The BMJ article reinforces my replies on this thread that the PCR test doesn’t show whether a person is infectious or not although a low CT rate is an indication that they are. Cell cultures are done if confirmation is needed.
You really need to stop being a patronising arse wipe, facts are facts and you don’t have any.
If it is patronising to point out the truth, then I am all for patronising. GlassHalfFull knows his stuff. You can even get a sample of the virus from the CDC.
I had this exact exchange with you, almost verbatim, a few months ago and you fell short of providing the actual evidence of Sars-Cov-2’s physical existence also.
A pair of shills trying to distract people from the truth, as soon as you come across someone who knows what they’re talking about you skulk off to try and manipulate the weaker minded instead, how about the two of you join your few working brain cells together and put me in my place?
EVIDENCE PLEASE.
What would count as evidence?
The entire genome has been sequenced many times. Here’s a company that appears to do it for a business:
https://www.paragongenomics.com/applications/infectious-disease/coronavirus-research/?gclid=CjwKCAjw4qCKBhAVEiwAkTYsPNSD1q6-i2LY5zzUG6zsSijU59NP-I41XeM0c7KQ7CRdFzfifIfVmxoCBYUQAvD_BwE
You can order a reference copy from the CDC.
https://www.cdc.gov/coronavirus/2019-ncov/lab/grows-virus-cell-culture.html
What more do you want?
That’s not evidence, it’s the same bogus science you cited last time. The link they include as evidence of isolating the virus is that same debunked study using 37 genetic fragments identified with PCR and then computer extrapolated to guess the other 29,000-odd remaining genetic base pairs.
And if you order ‘the virus’ from them, you aren’t getting the virus at all, you are getting a serum made up of human and animal cells with enough genetic components included to give a positive PCR result for what they claim Sars-Cov-2 is.
Totally manufactured, bullshit science.
I don’t what would count as evidence for you. I suspect that whatever I link to, you will dismiss it as “bullshit science”. But just in case it makes a difference here are three links to papers describing isolating the virus. The first two include electron microscope images of the virus.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7036342/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7366528/
https://wwwnc.cdc.gov/eid/article/26/6/20-0516_article
I am on this site because lockdowns do not work and it is all propaganda and I paid money to Toby Young to continue highlighting this problem.
There has never been an article on this site which disputes that the virus is real.
You would be better off going on to the David Icke site where there is a lot of like minded people as you who have little understanding of modern virology.
SARS-CoV-2 has been scientifically isolated millions of times and it’s “whole genome sequence” is known.
You do not know what you are talking about.
You have a logic block. You know the lockdowns are wrong and propaganda is being used against the public, but you refuse to make the further leap that the pandemic itself is fraudulent.
People are not filling the hospitals with Covid you dimwit, they are dropping from adverse reactions to the vaccine, a vaccine they never fucking needed in the first place!
You and I are on the same side but you wouldn’t believe it with the abuse you like to throw around.
The threat from Covid has been blown out of proportion by the Global Elite who are the only one’s who benefit.
It is not a vaccine it is an experimental jab and I know hospitals are full of people having adverse reactions to it and at 65 years old I haven’t had a vaccine for 40 years.
We need to persuade the Government to change course.
The difference between you and I is that you believe any old twaddle on Youtube whereas I prefer to research scientific papers.
You believe people like David Icke whereas I seek out expert virologists for their opinion.
We are not going to persuade the public to put pressure on the government to change course if the evidence that you believe in is so weak.
We don’t need to persuade the government to change course, we need to wake people up to the biggest scam in human history.
And the only way we are going to do that is by facts and not pseudoscience from the likes of Kaufman, Cowan, Bailey, Icke etc. etc.
Nobel-candidate scientists have taken alleged PCR positive samples and tried to cell culture them in the lab, but they never got any Sars-Cov-2, only influenza A and B.
The same architects of the Scamdemic have concocted your science as well.
Citation please.
You are misinterpreting the quote from the CDC. A positive result means the SARS-CoV-2 virus has been detected BUT the person may also have a bacterial infection and/or another viral infection at the same time as having the SARS-CoV-2 virus.
At the start of this scamdemic I talked to my friend who works in pharmaceuticals and asked if they would explain the PCR.
The first thing they said was that if the PCR was taken out of knowledgable, well controlled laboratories it would be a disaster, as PCR is highly sensitive and easily corrupted …so I think we’ve all seen that that is true.
In relation to SarsCoV2 the PCR detects a string of viral RNA, by targeting one or more gene fragments. Is this virus active? Infectious or virulent? The PCR cannot answer that. That is why a cell culture done in a laboratory is needed.
I’ve never read anything that contradicts it.
When we talk about high and low cycle rates, this doesn’t mean it does or doesn’t find SarsCoV2 it means it is or isn’t more likely to find the RNA strand it’s looking for.
That’s my understanding, and why when PCR evidence has been required in Court it has failed (Portugal/Austria) because it cannot diagnose a person unequivocally with the virus.
Correct.
There are many, many different types of PCR tests all of which are very accurate at detecting SARS-CoV-2 even the original Drosten et al test was quite accurate but has since been improved.
The problem is that governments haven’t requested the amplification or CT rate of all positive tests so we don’t know whether the person tested is infectious or not. A low CT rate up to 20 is probably infectious, a mid CT rate of around 25 is possibly infectious and a high CT rate 25 to 45 probably not infectious. (Wales uses a CT rate of 45). Cell cultures done in the lab determine if it is infectious or not. https://www2.nphs.wales.nhs.uk/DisclosureLog.nsf/($All)/25467EE5D9CE52DA8025860300312B35/$File/451%20PCR%20Test%20Cycles%20.pdf?OpenElement
A study in the US suggested that 85% to 90% of positive cases are not infectious. https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
A further PCR test should be done a day later after self isolating on the 25 to 45 group to ascertain the trajectory of the virus in the person to see if they are coming OUT of an infection and therefore not infectious or going IN to an infection and therefore infectious.
It is the lack of CT rate information which is causing the “casedemic” and NOT a fault with the PCR tests per se.
The ONS Dataset, Coronavirus (COVID-19) Infection Survey: technical data, https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/datasets/covid19infectionsurveytechnicaldata shows the CT rate for a random number of people around the UK. If on this data you set the upper limit of an infection at 25 then approximately 60% of cases would potentially not be infectious which could be confirmed with another PCR test 24 hours later.
This would give an accurate view of how many people are actually “infectious” whilst giving those with positive test results but “not infectious” to carry on with their employment and lives and would avoid the problems with a “casedemic” and dramatically reduce the “case” numbers and thereby reducing the anxiety of normal members of the public.
If on this data you set the upper limit of an infection at 25 then approximately 60% of cases would potentially not be infectious which could be confirmed with another PCR test 24 hours later.
As I understand it there isn’t a simple relationship between CT count and infectiousness. It depends on the details of the process including how the sample was collected.
The lower the CT rate the higher the viral load and infectiousness.
The higher the CT rate the lower the viral load and potential for not being infectious.
If someone doesn’t have symptoms and has a positive PCR test at a high CT rate they are unlikely to be infectious.
The PCR test is very accurate but governments are ignoring the CT rate data perhaps to err on the side of caution but it means the majority of people who test positive are probably not infectious and governments appear to be happy with that situation for whatever reason.
The lower the CT rate the higher the viral load and infectiousness.
The higher the CT rate the lower the viral load and potential for not being infectious.
Yes – but it doesn’t follow from that there is CT rate which you can sensibly use as a cut off point.
It is unlikely a high CT rate shows a high viral load.
Personally I would stop the PCR test and have focussed protection of the vulnerable (as per GBD) and allow the rest of the fit and healthy population acquire natural immunity which is preferable to the limited immunity from the experimental jab.
As I see it there are three uses of the PCR test.
The question of who to vaccinate is a different one.
We don’t test for flu and there is now no reason to test for Covid.
If someone has symptoms they shouldn’t be at work regardless of whether it is a cold, flu or Covid.
If they turn up for work they should be sent straight back home and compensated accordingly.
The statistics show that mortality “with” Covid is no worse than 2008 and before.
Many of the deaths were caused by lockdown and “saving the NHS”
Covid has been blown out of proportion.
Mask wearing and experimental jabs should be voluntary.
We do test for flu for diagnosis.
A key problem with Covid is that there is a good reason to suppose you can be infectious without symptoms – presymptomatic or asymptomatic – which is not true of fly – hence the case for screening.
You don’t address the case for tracking case of a new virus.
A lab diagnosis for flu is different to testing millions of people for Covid.
Covid is already tracked through the ONS Infection Survey using a few thousand volunteers around the country.
Taking each use of testing one at a time.
Diagnosis – I guess you accept that? Similar tests used for flu.
Screening – seems to be a good case as Covid subjects can infect when pre- or a- symptomatic
Tracking – ONS infection survey is great – but inevitably is at least a week out of date – often more. There is a good case for an up-to-date record which can also act as a check to be compared to the other methods of measurement – ONS, Zoe etc (In addition if these figures were not published it wouldn’t take long for the government to be accused of lack transparency)
They don’t use a mass PCR test on millions of people for flu. Very occasionally they would do a wet lab test for confirmation and to see what strain it is.
I suggest screening is now unnecessary as the elderly and vulnerable have all been offered the jab and natural herd immunity should now be the goal.
It is a scientific fact that natural immunity is preferable to the experimental jab induced immunity.
In natural immunity although antibodies fade within around 6 months memory B and T cells can give immunity for life. Some people still have immunity to SARS 18 years later and one woman had immunity from Spanish Flu 80 years later.
.They don’t use a mass PCR test on millions of people for flu.
True – I am only drawing the comparison when it comes to diagnostics.
Very occasionally they would do a wet lab test for confirmation and to see what strain it is.
According to the weekly national influenza and covid-19 surveillance report in the week ending 4 July (the latest I could find) there were nearly 3,000 tests for influenza. This at a time when there was virtually no flu around. I wouldn’t call that “very occasionally” – but I guess it is subjective.
I suggest screening is now unnecessary as the elderly and vulnerable have all been offered the jab and natural herd immunity should now be the goal.
You obviously have more faith in the jab than I have! I am fully aware that it is not perfect and fades over time. I am not sure that natural herd immunity is practical goal for a care home.
The rest of your comments seem to be about the merits of natural immunity which I don’t dispute.
They maybe testing more for flu in the UK as the southern hemisphere hasn’t been doing it and we won’t know what strain to expect in winter for Big Pharma to supply the correct flu vaccine.
I have no faith in the experimental jab whatsoever but the elderly in care homes may benefit from it, or it may kill them, or without a shot they may die from Covid. It’s a tough call but the patient themselves or their family should make sure they are fully informed of the options from a variety of sources not just the government run NHS.
I personally doubt that Boris and his cabinet have got their heads round the issue at all. It is Sage who are ignoring the CT rate data, which they do understand, and taken together with their clearly deliberately skewed modelling this has to point to deliberate misinformation.
A very helpful summary, thank you for taking the time.
You’re welcome.
But PCR is calibrated to ONLY test for Sars-Cov-2 RIGHT?
Correct to a point.
It was calibrated for SARS related coronavirus species so any variants or strains of SARS-CoV-2 could be detected.
It has been modified and improved since then.
No, because how can you possibly calibrate a test for a virus you haven’t isolated and therefore remove the chances of simply testing for background instrument noise?
The virus has been isolated in the scientific sense of the word and it’s whole genome is known. The whole genome of the cell that the virus is attached to and isolated with is also known as is any other substrate.
The accuracy and specificity of the PCR test is well documented.
And you pretend the BMJ quote doesn’t exist because it takes your weak argument to the cleaners.
If you are referring to this one I have answered it many times but I am happy to answer it again just for you.
“The only test for live virus is viral culture. PCR and lateral flow tests do not distinguish live virus. No test of infection or infectiousness is currently available for routine use. As things stand, a person who tests positive with any kind of test may or may not have an active infection with live virus, and may or may not be infectious.”
There are many, many different types of PCR tests all of which are very accurate at detecting the SARS-CoV-2 virus even the original Drosten et al test was quite accurate but has since been improved.
The problem is that governments haven’t requested the amplification or CT rate of all positive tests so we don’t know whether the person tested is infectious or not. A low CT rate up to 20 is probably infectious, a mid CT rate of around 25 is possibly infectious and a high CT rate 25 to 45 probably not infectious. (Wales uses a CT rate of 45). Cell cultures done in the lab determine if it is infectious or not. https://www2.nphs.wales.nhs.uk/DisclosureLog.nsf/($All)/25467EE5D9CE52DA8025860300312B35/$File/451%20PCR%20Test%20Cycles%20.pdf?OpenElement
A study in the US suggested that 85% to 90% of positive cases are not infectious. https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
I would suggest a further PCR test should be done a day later after self isolating on the 25 to 45 group to ascertain the trajectory of the virus in the person to see if they are coming OUT of an infection and therefore not infectious or going IN to an infection and therefore infectious.
It is the lack of CT rate information which is causing the “casedemic” and NOT a fault with the PCR tests per se.
The ONS Dataset, Coronavirus (COVID-19) Infection Survey: technical data, https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/datasets/covid19infectionsurveytechnicaldata shows the CT rate for a random number of people around the UK. If you set the upper limit of an infection at 25 then approximately 60% of cases would potentially not be infectious which could be confirmed with another PCR test 24 hours later and cell culture.
This would give an accurate view of how many people are actually “infectious” whilst giving those with positive test results but “not infectious” to carry on with their employment and lives and would avoid the problems with a “casedemic” and dramatically reduce the “case” numbers and thereby reducing the anxiety of normal members of the public.
This is just not correct. The probe / primer pairs used can bind to and amplify pieces of DNA found elsewhere that in the in silico declared SARS-CoV-2 sequence.
No doubt at all that the tests COULD detect almost exclusively SARS-CoV-2. But it’s not being used in ways which make that a likely outcome.
I had understood that all Coronaviruses are genetically 80% identical ( Dr MY and others ) Perhaps where SARS COV2 differs is that it is – according to Daszak and others and “they should know” – a chimera, genetically modified using a bat and rat virus with the backbone from a different virus inserted at the furin cleavage site to make it pathogenically lethal as well as transmissible among humans where the original bat and rat viruses used in its design were not – i.e. GoF in action.
I understand ( from the ILLA investigation and elsewhere ) that the Kary Mullis PCR does NOT test for the whole gene – the Cormen-Drosten RT-PCR fraud, instead of testing the two ends and a middle portion of the genetic code only tests I element (see pages 57 -70 of the ILLA pdf) so after RT conversion to DNA ( PCR does not test RNA matter as I am sure you know) and then amplification it confirms the existence of code that MIGHT be part of the whole SARS COV2 gene sequence, or it might be something totally different – Dr Richard Fleming’s test show no benefit of CT over 25.
Lastly Kary Mullis said (ante mortem) that the PCR can “give any result you want” and specifically that it is not a test of infectiousness.
Unless the WHO mandated Cormen-Drosten RT-PCR mass testing regime has been substantially altered – la plus ca change – has it?
As referenced very comprehensively below by “ComeTheRevolution”;
BTW Eurosurvelliance would be disposed to rubbish the ILLA report – they took part in the 3 day operation to publish, peer review and obtain the WHO mandate as the “Gold Standard” mass testing regime without mentioning that a member of the “peer review” team was connected to….messr Cormen and Drosten – a very clear conflict of interest.
Another conflict was that a member of the UK MHRA was part of the WHO team that signed off the Cormen-Drosten RT -PCR mass testing fraud – another undisclosed, factually accurate, conflict of interest.
“Factual accuracy” – sure is paramount.
Humans are genetically 90% similar to cats.
SARS-CoV-2 is different to other viruses and may well be a result of GoF.
The PCR tests for a fragment of the unique gene sequence.
The Cormen-Drosten et al test originally tested for the beginning and end bases and a computer generated the rest. Since then it has been modified and improved and millions of “whole gene sequences” have shown that the original computer generated ones were correct.
Kary Mullis has been quoted out of context many times.
CT rates over 25 do not mean infectiousness.
No, the PCR test, conducted at scale, mostly by technicians who’ve no history of commercial lab work, it’s not trustworthy.
There are no negative controls except for the final PCR plate. We’ve no idea what the actual operational false positive rate is in each facility & run.
The assumption is that it’s fixed & so close to zero that it can be ignored.
There’s no calibration so the number of cycles of amplification is totally arbitrary.
I don’t trust any result from such mass testing facilities.
Mike
The rate of positive test results went from about 2,000 a day at the end of May to over 50,000 a day on the 17th July. What do you think caused that increase? A dramatic outbreak of false positives?
“The Corman-Drosten paper describes some positive and negative controls as well as thorough validation. Precise setup of the test—including controls—is up to each individual user. And the user also has to define his own SOP.”
If you are the Mike Yeadon who co-authored the Review Report and the Addendum on the Borger-Kämmerer team against the Corman-Drosten et al paper you will be aware of the criticism of your report from people like Prof. Andreas Beyer who states
“The Borger-Kämmerer text is pseudoscience, it is full of misconceptions, errors and flaws. Therefore it is ignored by experts for good reason. The impact it had in public consciousness, however, is fatal. Borger reported on Twitter more than 30 Million views of his “Report” (March 2021) [now 50 million]. Hence I ask all colleagues please to spread this essay for at least a little bit of counterbalance.”
https://www.researchgate.net/publication/351286220_Borger_Kammerer_Corona_qPCR_Pseudoscience_Conspiracy_Theory_Revisited_-_an_Analytical_Essay_-
Just to be clear Mike I support 99% of what you say but I disagree with you on the PCR test.
A-fucking-men!
Agreed. Every so often, I read or watch or both testimony from around the world that sends another nail in the coffin of this casedemic non pandemic fraud. Earlier this week I watched John O’Looney, Milton Keynes Undertaker spell out his experience since Nov/Dec 2019 – I implore all sceptics and non sceptics to watch this man bare his soul – he anti faking it.
Today I read the testimony of De Stephen Hatfill – once again I implore people to read this on todays TWC or here : http://www.drstevenhatfill.com
I would be interested to know what folks think.
One comment. I find it disappointing that the authors of the great Barrington declaration as well as Drs John Ioannidis and Scott Atlas consider the vaccines safe. Why? The evidence is clear they are not safe or efficacious. And there is not any long term safety or efficacy data. See yesterday’s cdc VAERS. Another eye watering read.
Sorry Will , not at all compelling.
Gupta explains it well in terms of the adaptation of any particular virus.
‘Seasonality’ is a mixture of weather and humans changing location which induces a change in localised herd immunity. Virus exist in their trillions in the lower atmosphere, this coronavirus is no different. It moves around the globe on the back of weather patterns, wind and humidity. People change locations at various fairly fixed times; vacations, religious ceremonies, school opening, jobs, house moves etc. Both the natural and human seasonality factors overlay to temporarily change local herd immunities of all virus.
The graphs are as much a case of correlation not causation as anything else, but even here they are not good. If vaccination was overlayed it may also show an interesting correlation over the last year.
“There is no sign yet of the emergence of a new successful variant that will take over from Delta. This holds out the hope that Delta may be some kind of evolutionary endpoint or optimum for the virus, and thus that the autumn and winter may be mild from a Covid point of view – though other viruses like flu may take the opportunity to make a comeback.”
A new variant will of course occur by diktat or due to the vaccine, either way we can expect a ‘winter wave’ to mark the end of our ‘Freedom Holiday’.
Covid is clinically indistinguishable from flu according to the CDC.
““Because some of the symptoms of flu, COVID-19, and other respiratory illnesses are similar, the difference between them cannot be made based on symptoms alone.””
https://www.cdc.gov/flu/symptoms/flu-vs-covid19.htm
Isn’t it also the case that the current PCR test had its EUA withdrawn (pending) because it couldn’t distinguish between flu and sars? – essentially due to the Drosten paper that set out what the PCR test should be based on (spoiler alert NOT SARS CoV 2).
This is a common misunderstanding. The company providing the test withdrew its request for EUA because it had developed tests that were cheaper and quicker, including tests that could test for Covid and Flu simultaneously (it will still distinguish between the two). The new tests are not noticeably more accurate in testing for Covid as the existing tests are pretty accurate already.
https://healthfeedback.org/claimreview/eua-withdrawal-for-cdc-covid-19-pcr-test-is-due-to-the-development-of-newer-tests-that-help-save-time-and-resources-not-because-the-test-is-faulty/
Sounds like spin to me.
if the ‘new’ tests are not significantly more accurate why replace them.
Have you found a similar spin to explain ‘throw them in the bin’ about the LTFs?
if the ‘new’ tests are not significantly more accurate why replace them.
As I said – they are cheaper and quicker.
Have you found a similar spin to explain ‘throw them in the bin’ about the LTFs?
I don’t understand what needs explaining. Can you clarify?
May I point out that this piece is NOT compelling evidence. Rather, it’s a tedious load of boring graphs that no-one outside of the DS-reading regulars will bother with.
If we are going to change minds, we need a punchy, short, written-in-plain-English paragraph summarising the points, maybe backed up with a single, pertinent graph. This is true of most of the data-heavy pieces on DS.
I don’t think there’s anything wrong with data-heavy pieces per se, if they are well argued and don’t remain stuck inside the narrative of “cases”, but agree there’s a need for some pithier stuff. The data heavy stuff can be used as backup for those who want more detail.
I tend to agree, although the Daily Sceptic is a great source of info. in general, I fear they are falling into a trap focusing on this case numbers data, the debate on these numbers simply reinforces the idea in the casual reader’s mind that something serious is happening when it isn’t.
Personally I am focusing mostly on the death numbers because I think they are the only reliable data we have – the case numbers are simply not reliable enough to draw any conclusions from IMHO. See my link to my article in my reply under Bungle’s comment above.
Sure, headlines and intros could be improved. It’s all time and money, though.
Interesting piece in Conservative Woman – Google Ads, which control the on line ad market, have banned it from getting ads because of its excellent pieces examining the rna vaccines. This must be a key reason for the legacy media failing to ask questions.
Quite. Certainly the broadcast media are ransomed by Ofcom rulings and government handouts in the form of paid advertising; and print media much the same. The state is using Google and others to police internet-based media.
More ‘case’ and ‘surge’ bollocks. Problems with vocabulary rather than virus.
I suggest a listen to Sunetra Gupta’s exposition of the variant issue is rather more worth attention.
Question:
It is often said that viruses become less virulent and more infectious as they evolve, the reason being that the more virulent they are the less likely the host is to survive long enough to spread it on.
But where a virus is more dangerous to a sub-group of the overall population, the elderly in the case of Covid, presumably this logic doesn’t hold. At least not very strongly.
I can see how it might be more optimal for a virus to cause just the right amount of symptoms (coughs etc.) to allow it to be passed on, but weren’t sufficiently bad to cause the sufferer to stay in bed until better (which would limit the spread).
Once that optimum balance was achieved, presumably the virus would stabilise in what could presumably be a form that remained dangerous for the elderly and vulnerable.
In that case, could the arrival of Covid have a long lasting effect on average mortality, at least for, say, 5 years or so, until such time the elderly and vulnerable had built up immunity from prior infection from when they were younger and non-vulnerable?
“could the arrival of Covid have a long lasting effect on average mortality”
Well – it hasn’t so far! (Unless you’re dim enough to take an untypical short-term average)
Jon.. the average age of those dying is 82.. that should answer your question..
I probably shouldn’t have used the phrase ‘average mortality’. What I meant was whether we’ll see a few years of ‘excess deaths’ until such time the newly old and vulnerable have some prior immunity from having been infected when younger (i.e. now).
On further reflection I think my theory is probably correct. Whether it will actually shine through in the data or be unimportant relative to other factors is a separate matter.
Big scariants have little scariants
Upon their backs to fright us.
Little ones have lesser ones
So Mitchie’s crew can smite us.
Silly me, I thought it was the ‘vaccines’ that were the compelling evidence for causing the surges in ill health.
“Note that this graph is raw positive test numbers”
Completely worthless then.
The graphs are “raw positive test numbers.”
So basically bunkum.
BTW, who funds that Professor’s position?
Has anyone overlaid testing amounts with ‘case’ amounts in each country. Every time i look at a ‘surge’ in cases it is alongside a ‘surge’ in testing. India was a prime example, UK more so. The more we test, the more we find…?
Far be it from me to sound cruel but I have to wonder whether we’d even have variants if we hadn’t taken such a bullshit approach to covid. Covid was and is dangerous to those at the end of their lives suffering from various comorbidities and typically above the average age of death. I’m sure I recall that at least one variant of concern came about from someone kept in hospital in a near death state who was kind of fucked from the beginning but kept alive through various treatments which then caused this virus to mutate.
Whether that’s true or not, you only have to look at the harshness of nature when a virus hits the animal world. The weak are left to die, the herd moves on. In a perfect world of course, humans wouldn’t have to do that, we would have unlimited resources and medical staff and treatments with which to treat such diseases and situations.
But we don’t live in a perfect world.
Instead we live in a world where Big Pharma, Political egos and single issue ****stains have skewed our thinking to the point where we are very nearly all fucked over by the worst-ever reaction to a relatively mild harm.
Fuck the communists who fake-newsed the world into believing lockdowns were the answer after fucking us all over with their virus.
Fuck the Tories who couldn’t bear to be seen to carry on with a sensible strategy in case Peston and the left-wing trolls could accuse them of ‘letting the weak die’ and not being the party of the NHS.
Fuck the media who deal only in sensational fear-porn to generate clicks.
Fuck the americans who turned it into an anti-trump political jamboree and wanted to blame deaths on libertarians.
Fuck the so-called scientists who could only look as far as their next funding from big pharma and who deliberately played down the idea of a lab-leak and any kind of natural resistance or existing treatments to ramp up the possibility that this would need vaccines to get away from it all.
Fuck Hancock and all the other ****s who felt so important dealing with such a big issue and getting themselves all tumescent over the chance to play the hero.
Fuck Ferguson and every other modeller twatty skid-mark who continue to falsely claim that their advice has saved hundreds of thousands of people.
Fuck the young ****s in Eastern Europe who began the mask charade.
Basically, fuck everyone involved in the whole debacle, it’s been the worst of humanity.
I hope we get to a Covid Nuremberg in the next year or two ……..*****……. . The only way we will prevent this happening again is if we take strong action to inhibit these ****s from ever acting like this again.
Yours, amiably,
Norm.
This article has been moderated, witness the ***. Broadly speaking we enjoyed the views expressed in it, but this website is visible across all age groups, so I hope you dont mind but we have moderated the language a little. Thank you
It’s amazing and grotesque the amount of people falling for the ‘variant’ deception; doctors with integrity such as Mike Yeadon have already informed us that variants are NEVER dangerous and that they never ‘escape immunity’.
But even if C19 was real, which it isn’t – C19 doesn’t exist because it was never isolated and purified in laboratory [Koch Postulates], therefore everything else are LIES.
My motto is ‘KEEP IT SIMPLE’… so simple I keep it: because C19 doesn’t exist, the jabbed cannot get ‘infected’ with it, nor the ‘vaccines’ can producing ‘variants’!!!
Stuff your ‘variants’. All coronaviruses continually mutate. So what. Mutation tends to decrease virulence and increase transmissibility. It appears that vaccinated people are the source of new variants. However, a forensic approach is needed. We are dealing with an unprecedented worldwide crime scene, with two central frauds (1) the myth of asymptomatic transmission (2) the use of PCR test for ‘diagnosis’. This implies that absolutely no derivative Covid data (eg ‘variants’) can be believed. Another source of fraud is computerisation of laboratory investigations and findings, because all computerised processes are vulnerable to psyops hacking and results falsification. Absolutely all data concerning SARS-Cov-2 should be considered to be fraudulent. This accords with Lord Denning’s 1956 judgement that fraud vitiates everything it touches.
You couldn’t make this shit up. First, the bent FDA inexplicably sanctions the roll-out of a bunch of gene-changing experimental vaccines – bang in the middle of a global pandemic. This, entirely predictably according to numerous experts, leads to virus escape and sparks a succedssion of variants which trigger continuous waves of infection. And the masterly solution to this self-created problem? “Booster” shots every few months for the vaccinated of the same, tweaked snake oil which failed to protect them first time around! No wonder Bill (“I want to vaccinate everyone on the planet”) Gates and his cohorts are laughing all the way to the bank.
This article could do with a few more graphs.
Thanks for an interesting article and quite convincing that the virus mutates until it becomes endemic and seasonal. Now possibly having to compete with other viruses especially the reappearing influenza virus in Indian Sub Continent,South Africa and Arabian Peninsula and even a sporadic influenza virus found in Germany.
If we did not have sequencing of the virus, we would have the world picture with the three waves. However, these waves need to be correlated to deaths and more important excess mortality to see whether it has become endemic.
Influenza pandemics behaved with these waves and the different secondary waves were driven by mutating virus but we had not resources at that time to do sequencing. The Spanish flu waves has mostly been done retrospectively and Spanish flu is shown most clearly in the excess mortality waves.
It will take 1-2 years for a pandemic influenza virus to mutate enough to become the next seasonal influenza virus and the corona virus seems to be very like influenza in its ability to mutate. We are just waiting that the C 19 will become our next endemic seasonal 5th coronavirus and having to compete with all other 200 respiratory viruses.
Reading some of the comments here is disappointing with attacks on the author and DS for publishing it. Just change the word variants to mutation and then it makes much sense.
People are killing the messenger for stating rather obvious scientific facts. It is quite another ballgame the whole mad response to the pandemic, throwing out Henderson’s pandemic guidelines, over emphasizing case detections, useless NPI/LD, mad mass vaccination (increasing the mutations) when having a disease with very well defined risk groups where a very selected approach with experimental vaccines would make a sense.
The appropriate response was only to increase hospital capacity for this unstoppable new respiratory virus.
So the vaccines drive the variants? Those countries involved in initial vaxx trials experienced variants. You know the kind that occur when the virus fights the good fight to survive. Also variants spread quicker but are less virulent. Sort of like now, so many cases of covid in the double vaxxed but deaths and hospitalisations continue to be low. So when the next experimental biologicals is produced can we expect the next variant?
Israel is the poster boy for Pfizer. Loads and loads of covid after not one, not two, but three shots. Why do people still think this stuff works. Yesterday’s cdc vaers makes for another eye watering read. Between Dec 14 and sep 10th 2021, 791,561 adverse events and 14,925 reports of death an increase of 419 over the previous week.
For the real story on viruses, variants and immunity, have a look here: https://juliusruechel.substack.com/p/the-snake-oil-salesmen-and-the-covid?r=lcww7&utm_campaign=post&utm_medium=web&utm_source=copy
Herd immunity is never perfect for rapidly mutating respiratory viruses.
WHO CARES??? Viruses are nothing to be frightened by. In the eighteen months that have elapsed since the start of the first wholly unnecessary lockdown my wife and I have met a total of two people who who knew of others who had died ‘of Covid’: one, a neighbour, knew someone who knew someone who knew someone who was related to someone who died ‘of Covid’, the other, a typically loquacious taxi driver who claimed to work with someone related to two people who died ‘of Covid’. We know of just two people who have tested positive for the virus. One, my brother-in-law, although perfectly well, tested positive, self-isolated for two weeks and developed no symptoms at all, the other, a women who is not at all work-centred, fancied two weeks on furlough.
And that’s it for Covid over the past eighteen months.
By contrast, a close friend of my brother’s next-door neighbour had the first jab, despite their pleas to him not to, and died two days later, and everyone of my wife’s forty or fifty colleagues has suffered an adverse reaction to their jabs, approximately a dozen of whom were so severe they needed more than two days off work.
There are ‘variants’ of a virus that is little more severe than a common cold and has an average age of death two years higher than for all other causes and a survival rate in the highest risk group of 99.32%, so what?
I don’t trust any of the data upon which all analyses perforce are based.
PCR mass testing simply isn’t capable of distinguishing an infected person from incidental carriage.
The sequencing required to be sure of what’s in the samples is also being badly done, according to Dr Sin Lee, who has repeatedly written open letters to the CDC.
He believes mostly that they’re still sequencing small stretches of what is thought to have been viral RNA, and too few of the specific mutations are confirmed in many such determinations.
So while this is all very interesting, I’m left scratching my head, unsure what if anything can confidently be drawn from the many plots.
Credit to Will for the efforts,though. Wouldn’t want to take anything away from him.
Cheers,
Mike
I have to question this article in the light of the Milton Keynes Funeral Director Mr O’Looney concerning his belief that the increase in deaths allegedly due to Delta Variant have come as a result of the Vaccinations. This was first observed in India, then Gates visited India four times and eventually the link was dropped from pressure Gates brought to bear. The vaccinations contained virus particles. There was never a sudden surge of visitors from Asia into the UK to cause the Delta Variant. Neither is there corroborating evidence to suggest all the countries shown in the graphs above have had similar large influxes of Asian people. When all the possibles are removed the only probable answer is that the vaccines are causing the variants, especially Delta. Irrespectively we are still being fooled into accepting false-positive results as actual symptomatic cases and deaths as all covid created. The mislabelling of deaths and poor quality of tests and lab results are not something that should be relied upon. Once the Government has sufficient DNA samples from the testing they will not be pushing them as much. The Vaccine passport is a backdoor method of the country accepting ID cards.
Lord Stephen, Baron