A few weeks ago, the Washington Post announced “President Biden, doubly boosted, is in a much more favorable position to fight COVID-19 than President Donald Trump was before the rollout of vaccines.” NPR elaborated, “Even if you’re the president, it’s hard to avoid a breakthrough Covid infection.”
We all know many individuals who have been vaccinated and boosted, yet still get infected. How does that happen? One reason is that original COVID-19’s SARS CoV-2 virus – to which human populations have built immunologic resistance through exposure, vaccine or both – no longer circulates. References to current illness as COVID-19 represents a category mistake (when a person talks about something as though it’s a different type of thing from the thing it is).
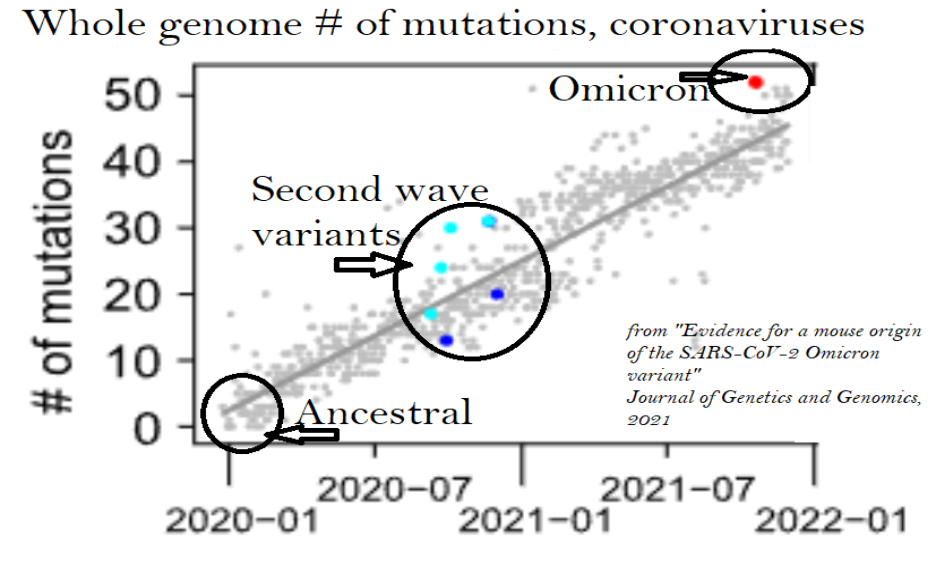
It was still pertinent to speak of ‘COVID-19’ after the late 2020 exit of the ‘ancestral’ version, since certain SARS CoV-2 descendants, via mutation, found gaps in our immunologic defenses to become next-generation (but milder) ‘variants of concern’ (VOC). They ran sequentially through the Greek alphabet, springing up around the globe: Alpha (England), Beta (South Africa), Gamma (Brazil), and Delta (India).
All of these second-wave variant-strains ultimately disappeared, superseded in the category of coronavirus infection by the significantly milder virus found circulating late 2021 in South Africa. This virus was given a Greek letter name as per the previous VOC format – but this was inappropriate, given that Omicron strain is not a lineal SARS-CoV-2 descendant.
Its sufferers are not therefore having ‘breakthrough’ COVID-19 cases. Omicron is a coronavirus, so there is some crossover; however, there is no substantial immunologic protection from previous natural-illness COVID-19 recovery – and essentially zero from doubly-dosed COVID-19 vaccines.
Before the SARS and COVID-19 pandemics, the textbook definition of a coronavirus episode was “acute, mild upper respiratory infection (common cold)”. Omicron symptoms are indistinguishable from the cold’s to the point that, in April, England updated its ‘COVID-19’-symptom list effectively to coincide with the common cold’s: “It’s not possible to tell if you have COVID-19, flu or another respiratory infection based on symptoms alone,” officials say.
Yet, experts have not acceded to a return to (pre-Covid) normalcy (of not fussing over the coronaviruses whose symptoms overlap with myriad other common-cold viruses).
A friend mentioned his exasperation and wonder of coming down with “COVID-19, again!” – but what were his actual symptoms?
“Not much, a bit of a cough, some achiness for two days; my wife had a fever of 99°, basically a summer cold.”
“The President Gets A Summer Cold” isn’t news. Those Biden articles weren’t ‘fake news’ per se, but they did beg the question in declaring his illness to be “COVID-19”. The press is not fully to blame insofar as public health authorities purposefully keep outworn, outdated ‘COVID-19’ in the lexicon.
I propose that the vastly milder illnesses emanating from today’s predominant strain 22B-Omicron-BA.5 (and its successors) deserve rebranding outside the COVID-19 franchise. From a scientific standpoint:
- The “22B” prefix reflects discovery as the second Omicron of 2022 (fully three years after COVID-19’s eponymous origin).
- “There’s no transparent path of transmission linking Omicron to its [COVID-19] predecessors.”
- Genomically, Omicron’s gap from second wave VOCs exceeds theirs from the ancestral strain.
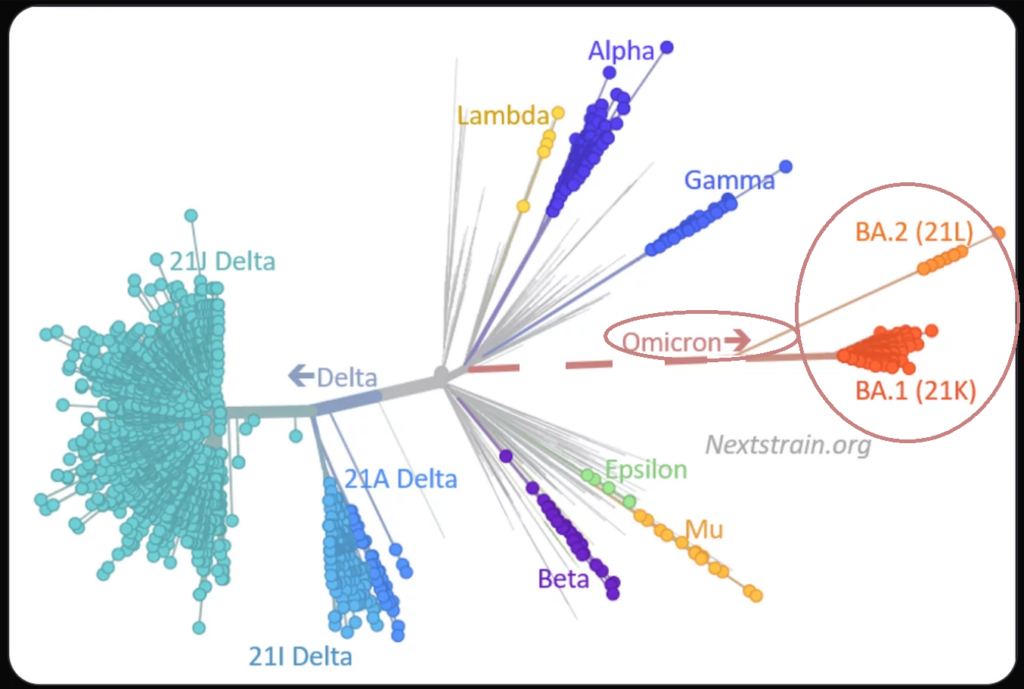
In other words, (per Emma Hodcroft of Nextstrain and the University of Bern): Omicron is almost like an orphan, without close relatives on the COVID-19 tree. Micaheleen Doucleff explains: “Its genes just looked so different from the other [COVID-19] genome sequences.”
Dr. Hodcroft places Omicron on a genomic map far afield from all previous SARS CoV-2 strains, positing but never proving connection to the COVID-19 ‘family tree’.
Clinically, Omicron is less lethal than influenza, verging on common cold, according to the Financial Times.

Omicron infection does show as a positive on ‘COVID-19’ tests; however these have never been shown to be specific to SARS CoV-2 (versus other coronaviruses).
As Omicron’s not a direct SARS-CoV-2 descendant, it may just be an (uncommon) ‘common cold”.
“Omicron may have picked up some genetic material from a cousin, a common cold-causing coronavirus,” notes Dr. David Aronoff.
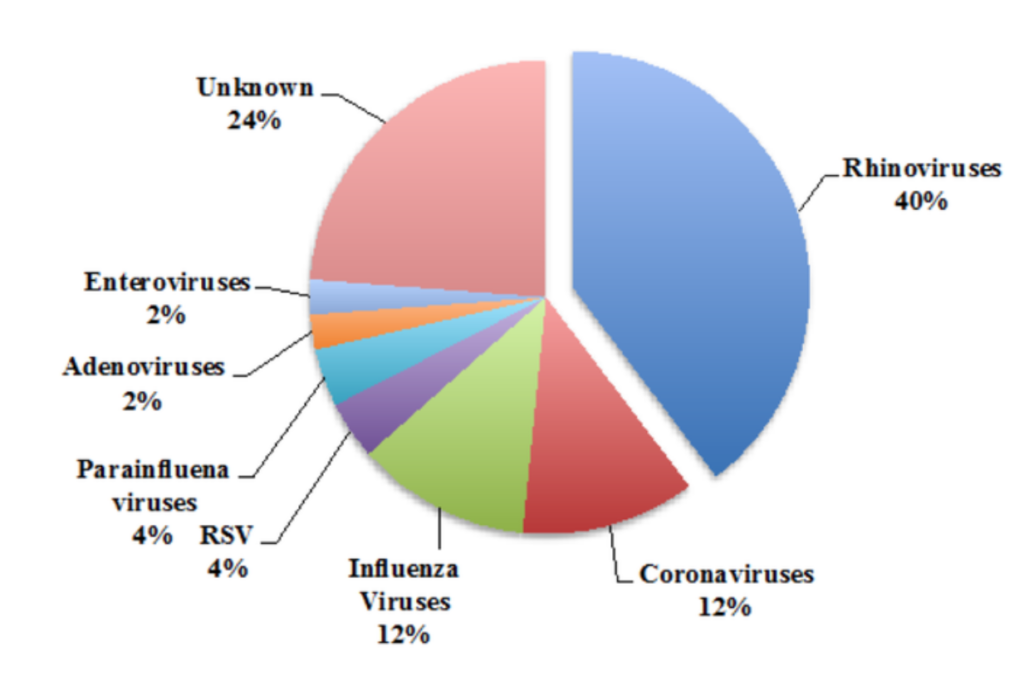
This shouldn’t be shocking: coronaviruses represent the cold’s second most common cause by type.
Historically, there has been no nomenclature enforcement regarding the ‘common cold’, itself a bucket-term based on symptoms rather than viral subtypes. So whether Omicron is a classic ‘common cold’ coronavirus or a novel coronavirus that looks and acts exactly like any common cold is a distinction without a difference.
No doubt if, for some reason, we put this same level of attention and testing to the other disparate viral causes of common cold, we’d find unusual variant strains of RSV, adenovirus, influenza B, etc. The thing is, we don’t – because there’s no cause to do so.
Omicron brings any further deep focus on coronaviruses to a point of diminishing personal and societal returns. Common colds are not tracked, discussed, tested, pre-vaccinated – let alone used as cudgels bureaucratically and legally.
Omicron, nonetheless, is still considered ‘COVID-19’ – yet warrants reassignment as ‘common cold’ – or perhaps baptism as ‘Corona-22’ – relegating erstwhile dangerous but now disappeared ‘Covid-19’ SARS-CoV-2 to the history books. So much confusion would be eliminated by Omicron’s simple rename to ‘Corona-22’.
- Current infections would no longer incorrectly be deemed COVID-19 vaccine ‘breakthroughs’.
- Antiquated COVID-19 vaccines would be seen immediately as having no rational reason to be called ‘boosters’.
- It would be medical malpractice to inject a 2019 flu shot today, even if relabelled as ‘booster’.
- COVID-19 vaccines could be memorialised for prior contributions, while removed from Corona-22’s pharmacopeia.
- mRNA for COVID-19’s SARS CoV-2 would be removed from the (inappropriately) ‘bivalent’ new anti-Omicron vaccine.
- As a medical side note, retirement has occurred routinely with Monoclonal Antibody Therapy (MAT). Each is phased out as its VOC disappears.
- Vaccines and MAT produce the same result: spike-protein antibodies; yet, while MATs’ shelf-life coincides precisely with its matched VOC, the ancestral 2020 COVID-19-vaccine has persisted with its own VOC long gone.
- The ambient ‘fear factor’ would downwardly recalibrate to Corona-22’s (Omicron’s) around tenfold diminishment in lethality.
- We’d have closure for the COVID-19 pandemic. (That day will eventually come, why not now?)
- COVID-19 societal roadblocks would contextually achieve obsolescence. The masks come off (and absurdities such as requiring this year’s pre-school children in Philadelphia again to be masked would more easily be counter-litigated).
- We’d begin to appreciate how common-cold coronaviruses got there in the first place – by the same ‘in like a lion, out like a lamb’ pathway.
Interestingly, the last point might help elucidate some of the others. Instead of lions and lambs, let’s look at wolves and poodles: both emanated from some now-extinct wolf. Current-day wolves can be as dangerous as they choose, having no investment in human health or happiness; from their own sanctuary they take human life with no remorse. The poodles’ ‘sanctuary’ is humanity. It’s foolhardy to bite the hand that feeds.
By analogy, Ebola, influenza, and the original 2003 SARS have animal reservoirs in which to retreat and regroup – and thus, can be vicious. The common cold is more like the poodle. Its viral success requires keeping human hosts upright, semi-functional and sneezing. Hospitalisation and death interrupt the chain.
A strong perimeter makes sense against wolves, but not poodles. There are influenza, but no common-cold vaccines. Pfizer is prepping one for Omicron, but as a tweak of its COVID-19 shot, keeping it under the Emergency Use Authorisation (EUA) umbrella. So long as the operative disease or virus term remains ‘ COVID-19’, the EUA’s liability-reduction, pharmaceutical company enrichment and political leverage remain. H.L. Mencken, cynic, said: “The whole aim of practical politics is to keep the populace alarmed (and hence clamorous to be led to safety) by an endless series of hobgoblins, most of them imaginary.”
Whether governments had valid reason to bring fear in 2020 is arguable. None exists in 2022. The EUA, as the gift that keeps on giving, prevents any turning of the page from COVID-19 to Corona-22 or some other rational resolution. There is no reasonable or legitimate public safety purpose to behave as if ‘COVID-19’ is still the major threat in 2022, nor that the COVID-19 vaccine is still necessary. Moreover, the incipient ‘bivalent’ Omicron vaccine fulfills no genuine patient need. Historically, the common cold has never been pre-vaccinated; vaccinating after-the-fact has minimal positive and potential negative effects; and the COVID-19 portion has no medicinal, only legal purpose for existing as the second ingredient.
Dr. Randall Bock is a primary care physician near Boston, Massachusetts, and the author of Overturning Zika. Read his blog and follow him on Twitter.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Many of us on here instinctively saw the March 2020 lockdown madness right away as a watershed moment and a clear leap forward towards the dystopia Simon Elmer describes.
Since then, for me at least, it’s been very stressful and relentless battle to alert people to this danger.
To be honest, I still don’t see anything but the large mass of the people marching towards their digital enslavement either oblivious or resigned that there is nothing they can do to avert it.
Anyone who’s alarm bells went off in early 2020 deserves a big pat on the back for having the wisdom and intelligence to understand that something was just not right with Covid 19.
Despite the almost universal understanding that this ‘virus’ had a 99.8% survival rate, that those dying were dying ABOVE the average age of natural death and that, despite social media, know one actually knew anyone who had unequivocally died of it, the governments still decided to lock the world down, stamp on civil rights, shut down the world economy and insist that everyone was injected with a highly dubious experimental drug.
Just as an illness has no chance of being cured unless the diagnosis is correct so Covid 19 has been misdiagnosed and the treatment and cure will, therefore, be ineffective.
This is an illness, just not a virus. Covid is actually an imaginary virus that does not exist in reality.
The real illness is Mass Psychosis, easily the biggest outbreak since the Medieval Witch Trials and just as lethal.
It is the apparent irrational, bizarre and illogical reaction to this illness by the Governments and elites that have indicated to the skeptics that this MUST have been planned but, in fact, makes sense when we understand that it is actually the Doctors, scientists, politicians and media who were MOST affected by this group collective insanity.
The doctors were busy ventilating panic attacks, the elderly were being dispatched in the care homes with Midazolam and Morphine, the scientists were insisting PCR was 100% accurate (when the true figure could well be 0%) and people were dying at home from the effective shutdown in the health services. Add the vaccines, that must be killing people if Covid does not exist, and all those deaths, added together, equal the supposed Covid and excess deaths.
The Governments and elites are, today, simply acting out of irrational fear as the real cause of Covid has still yet, I believe, to be understood. Some of these people may understand what has happened but, if true, they would have to keep quiet as jail, or death by mob, may be a distinct possibility for daring to admit it.
The actual threat is that not understanding that this was a Mass Psychosis outbreak over an imaginary virus could lead to something even worse in the future.
As the saying goes “those who can make you believe absurdities, can make you commit atrocities”
We’ll have to wait and see.
The mass psychosis you refer to is the brainwashing that has taken place across the whole of the NHS, and you most definitely. I know upwards of a score of people who work in the NHS or associated fields and their adherence to the Covid1984 story is absolutely astonishing. Have you all been drugged and chipped?
Despite your disavowal of the covid story you have still been captured by it.
Have you not read and understood the above article? Covid1984, real or imagined, is not the point. The real point is Control and lockdowns were simply the opening Blitzkrieg aimed at taking control of national populations.
Your blinkered intransigence is staggering. For someone in your position I must say you are a menace and sadly I am beginning to think the same of all NHS staff.
How exactly have I been brainwashed if I’m saying that the medical profession went stark raving mad over an imaginary virus and slaughtered lots of innocent people?
You obviously don’t work in the NHS but, believe me, that’s NOT a popular point of view.
In fact, If I said it out loud to the management, I’d almost certainly be sacked.
Same here. I was posting on the DT website in April 2020 that Covid was “a very useful crisis” and the Establishment were using it to force through policies which otherwise they would struggle to advance – ie a cashless society.
I do think Covid was a test run, it started pretty well with lockdown compliance high, however I think the jabs where a failure. 20-25% of the population withstood the coercion. Jabbing kids was beyond the pale for most except the most ardent brainwashed zealots. The 40,000 who stood their ground in the face of no-jab no-job are heroes who proved that no amount of coercion will work on many of us.
Will they one back and try again? Maybe, maybe not.
Schwab et al couldn’t organise a piss-up in a brewery.
Is that to say we shouldn’t be very concerned by the direction things are going? No, of course not, but let’s not imagine they’re more competent than they are, and let’s realise how impractical their ridiculous ideas are. The control they want is absolute, and they are too blinded by idealism to realise it simply cannot succeed.
“The weakness of all dictatorships is that they are vast bureaucracies – what does not exist on paper does not exist.”
Frederick Forsyth, The Day of the Jackal
You don’t need to be competent to dictate to people. You just need power.
An enormous amount of power is concentrated in the state and its institutions. That power can be and is captured and used for the benefit of some at the expense of most others.
Given that the state has accumulated all that power over time, somebody will be there to wield it. I suppose you can hope that it will be well-meaning people that only act in the interest of the general public. Or you can be realistic and expect that people who are good at manoeuvring their way into power are likely to be not very nice people.
The massive accumulation of power in the state (or in anywhere really) is the fundamental problem. Once that happens, you can only expect that eventually terrible things will happen.
Competence or incompetence has literally nothing to do with it whatsoever.
I think you both make valid points.
More competent tyrants are more dangerous, surely.
Another question is whether the power grab has a notional “benevolent objective” or whether it is unambiguously malign. While I don’t agree, it could be argued that climate change or better management of the economy would both be better addressed by having a system based on central bank digital currency / personal ID / social credit. For example, limiting people’s ability to fly or drive using a system other than rationing based on price might be seen as fairer. Likewise, the use of negative interest rates to manage an economy would be arguably much more effective with a CBDC than the current system.
For people you say “couldn’t organise a piss-up in a brewery,” they seem to be achieving their objectives so far.
In other words – what Icke said.
If I write a book can I also advertise it on here in the guise of an article?
The Advertorial Interaction with Free Speech and Journalism by Occams Pangolin Pie. Now available from all good bookshops. Please see screeds of details below on how to register your retina with our online Credit Score factors.
Anyone else find the phrase Add to Cart sinister?
Only when preceded by the words ‘Bring out your dead’.
A good piece, thank you. I’d suggest flying farther above the clouds and seeing with even clearer perspective.
The Hegelian dialectic currently at play (create the thesis and its antithesis, control the synthesis, perpetuate conflict) was also around during WWII.
Wall Street financed Nazi Germany. Mussolini was employed by MI5. And so on.
The point is – the enemy is always YOU.
The Satan-worshipping cabal of top-tier international finance has always been at war with humanity. Let’s stop shying away from the fact we are at OPEN WAR with them.
We must then wage this war wisely – with unity, kindness, compassion, awareness.
http://news.bbc.co.uk/2/hi/uk/8306475.stm
https://www.theguardian.com/world/2004/sep/25/usa.secondworldwar
But precisely why are the RPTB doing this.
Surely a major factor is that they realised years ago that Capitalism which they grew fat on, was dying and 2008/9 was final proof, the temporary way out only being to print more and more money which only kicks the can down the road.
The result now is that every “Western” nation owes trillions in debt.
But who exactly is that debt owed to?
It’s owed to the RPTB, the very bastards screwing us at the moment.
You’ve got to give them credit for using climate change, proxy wars and “pandemics” to instil the necessary fear to gain compliance, our only salvation being grateful acceptance of their digital social credit system – purely to enable them to carry on screwing us.
One way out would be for every nation to simply say in unison that they will not pay the “debt”.
I wonder what action the likes of Black Rock, Vanguard, The Great Unseen Banks ie the Rothschilds/Rockefellers etc would take to stop it happening.
I believe a certain Austrian Chancellor tried that about 90 years ago.
It didn’t end well.
Don’t lump Vanguard in with BlackRock, please.
The two are quite different organisations, with completely different ownership structures.
Jack Bogle (RIP) founded Vanguard in 1975 to great scorn from all the money managers, as the first passive Index Fund and a mutual which has done enormous amounts to improve the lot of the Regular Joe.
BlackRock, on the other hand… Don’t get me started, but I will write that Rob Kapito is a proper douche and a huge part of The Problem.
Thanks for the information.
I didn’t appreciate the distinction.
While appreciating the differences in structure (investors vs shareholders, etc), Vanguard Group Inc is one of the top investors in BlackRock (7.86% / 11,930,799 shares) and BlackRock Fund Advisors is one of the top investors in Vanguard (14.29% / 90,297,279 shares)(as of June 2022) and, for all practical purposes between them they own significant holdings in the vast majority of global companies. Vanguard’s purpose is focussed on (from their website): ‘investor needs first’ – which I assume is RoI or profit rather than social justice for all, just like BlackRocks shareholders. So pots and kettles, when it comes down it. Tim Gielen’s vid worth a watch https://www.youtube.com/watch?v=nuSpEgFkW94
Great to see Simon Elmer on DS. Elmer’s writings were hugely important and instructive for me very early in the plandemic, and back then, I wasn’t aware of anyone writing with more lucidity about the confected crisis and its totalitarian implications. I remember thinking instinctively right at the onset of the corona exercise that the state had effectively declared war on us, and it was so reassuring to read the words of someone who was able to express this in such an intelligent and coherent way.
But I find the current state of biosecurity affairs fascinating. We seem to be in a strange period of limbo where the corporate and state powers responsible for the plandemic are unsure about whether to maintain the pretence any longer. There was certainly a plan to forever change the social contract, making access to normal life contingent on regular ‘vaccinations’ but this clearly collapsed under the weight of its own nonsense and became completely untenable when it became obvious even to the most brainwashed that the injections didn’t work, even on their own preposterous terms. ’They’ overplayed their hand and in doing so exposed themselves to more scrutiny than they have even known. I think at this point we – the ones who weren’t fooled – have the initiative and need to make sure that the crimes of the last nearly three years don’t go unpunished.
Any way, I’ll be ordering the book. Enjoyed the article.
“Since the revocation of coronavirus-justified regulations in the U.K.”
Well, the enabling legislation – the Public Health Act 1984 – is still on the books.
Yup …. and Hunt, who supported Chinese-style full lockdowns and mandatory jabbing, has effectively been appointed Fuhrer.
This is the current status of The Tyrants Charter (pt 2) AKA The Coronavirus Act 2020.
It was last updated 7th October 2022.
Note Northern Ireland temporary powers remain in force.
https://www.gov.uk/government/publications/coronavirus-act-2020-status#full-publication-update-history
The Tyrants Charter (pt 1) AKA The Public Health (Control of Disease) Act 1984 – is still valid, festering on a back burner, ready to be reignited.
Elmer’s book certainly sounds interesting. But his launch piece here doesn’t mention the other war that has been going on at more or less the same time.
And it is important to note that the war against affordable and reliable energy (which IS mentioned) started, at latest, in 1988. It seems possible that the Covid war came about because the Climate, or initially Warming war, had run out of steam.
But the war that is not mentioned here, or at least in Simon’s piece, is “The War on the West-how to prevail in the age of unreason” admirably set out in Douglas Murray’s brilliant new book, which amazingly seems to have had little mention on LS, or anywhere else.
Douglas specifically writes about the Critical Race Theory nonsense, the rise of REAL (anti-white) racism, of antisemitism, or the complete uninterest of our Beloved Leaders in the ongoing invasion, in the Muslim rape gangs, in the continual attacks on Western (especially British) history and culture, the incessant ‘blame’ for slavery to the West (which Britain went to great pains to abolish) but the ignoring of the larger and much longer slavery to the East and, of course, the slavery that is so obvious today. He also points out the sheer oddity of heaping blame on an obscure letter by David Hume, whilst airbrushing far more direct racist and antisemitic letters from Karl Marx.
This is by no means a criticism of Elmer’s book, which obviously I have yet to read. But it does seem odd that the war that he describes in the piece above was going on, just before the death of George Floyd sparked off paroxysms in the war against “whitey”, usually by the same “Antifa” protagonists.
An excellent excerpt, book ordered! I just wish that someone would be able to help organise the resistance, instead of each of us desperately trying to be prepared and doing our own thing. I make contact with other like-minded individuals in my area (or even generally), but it won’t be anything like enough. Anyway, forewarned is to a certain extent forearmed. (I am interested that Toby has let this go at the head of today’s DS email. Is he moving away from his bumbling foolishness of government idea?)
In order to implement this dystopia it would be necessary to change human DNA and achieve an enormous loss of individuality. Perhaps there is a connection between these things and concealing the faces of human beings while regularly injecting them with gene therapy. Sorry, if that sounds slightly sarcastic. These two assaults are the most objectionable, closely followed by Social Credit Scoring and biometric surveillance and governance. Patrick M Wood has predicted much of this for some years, but Elmer’s article and book are more than welcome. I too have been derided for venturing to warn of our impending fate, but fewer people are laughing now.
Part of the reason for the government’s easy removal of our democratic rights was the gutless, ignorant journalists in the mainstream media. None of whom carried out any accurate research or queried if the governments actions were fair or reasonable and the politicians who did not properly query what the government was doing. Hancock was a complete medical imbecile given the job of health secretary pretending he knew what he was taking about, signing off laws he knew nothing about. How is he still an MP?
The financial collapse, caused by decades of fraud, quantitative easing, selling out to the CCP, building-up unpayable debt that was never properly resolved after 2008 isn’t going to go away. Of course government’s are going to try to impose all manner of control measures to save their own skin whilst blaming the inevitable consequence of years of irresponsibility on a pandemic, institutionalised racism, Climate Change, Vladimir Putin, another pandemic, Dr Evil plotting to take over ze world, etc.