
During the COVID-19 pandemic, Denmark and Sweden took very different approaches. While Denmark imposed mask mandates, closed schools and repeatedly closed so-called ‘non-essential’ businesses, Sweden imposed hardly any all-encompassing restrictions. Lockdown proponents have accused the Swedish authorities of recklessness and claimed their approach has led to an unnecessary death toll.
But now the numbers are out, and according to two Danish professors, Christian Kanstrup Holm, a virologist and Professor at the University of Aarhus, and Morten Petersen, Professor of Biology at the University of Copenhagen, in an article in the Danish newspaper Berlingske Tidende on July 8th, excess mortality in 2020 and 2021 was in fact the same in both countries.
In Denmark, harsh restrictions were justified by the need to prevent the breakdown of the healthcare system and the public has generally accepted this justification. The professors’ conclusion however is that this justification does not hold: despite very few restrictions in Sweden, the Swedish healthcare system was never even close to breaking down.
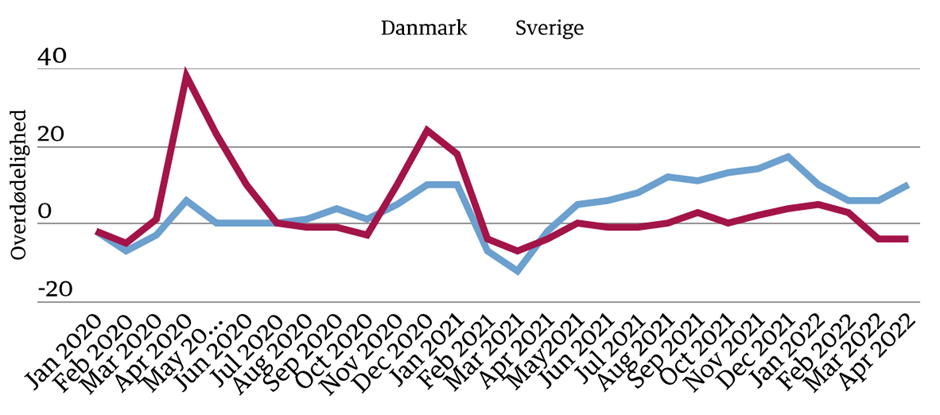
In 2020 the Swedish certainly saw excess mortality while mortality in Denmark remained approximately the same as in previous years (see chart below). But in 2021 the situation is reversed, according to the data. The two professors also point out that in 2020 there was in fact no excess mortality in Sweden among those below the age of 75, which simply confirms how COVID-19 primarily attacks the oldest.
According to the models used to justify harsher restrictions in Denmark, about 30,000 people were expected to have died had Sweden’s strategy been followed. But according to the data, the excess mortality in Sweden over the two years was around 6,000 and in Denmark 3,000, which amounts to the same percentage as the Danish population is about half the Swedish. Thus, the models were off by around 90%. It might be added that this year we see continued excess mortality in Denmark well above that in Sweden (though not all the excess mortality is with COVID-19).
“It often happens,” the authors say, “that individuals, groups or even whole populations get caught in false dichotomies. Those are commonly based on powerful anecdotes and lead to a general acceptance of the validity of one or more claims, which do not stand up to scrutiny.“ While some false beliefs may be harmless, “they can also persist for a long time, even if they have serious negative consequences, both for individuals and whole populations“.
They urge the authorities to make sure that in the future all consequences, including negative effects of restrictions on public health, psychological well-being, education and the economy be considered. For this to happen “it is crucial to have the courage to debate and analyse”.
Thorsteinn Siglaugsson is an economist who lives in Iceland. Find him on his Substack page.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Giesecke and Tegnell said right at the start, judge us in a year or two.
I am waiting for the Swedish King’s apology to them.
Unlikely, he’s very thick.
A long wait.
Indeed, one cannot call the winner at halftime.
Let’s hope that a proper debate ensues. It’s good that Sweden followed a different approach, especially as it was almost unique on this side of the pond. However, similar discussions could be valid between certain American states as well.
Absolutely. Texas and Florida versus California. Plain for all to see, if only they weren’t so distracted by and supportive of TheCurrentThing™
Indeed, on an age-adjusted basis, Florida’s excess deaths were equivalent to California’s.
Voluntary measures were sufficient to avoid all the other negative outcomes that we’re now experiencing.
The death toll probably wouldn’t have been much different.
Now we’re left with a legacy of record waiting lists on the NHS and people dying and will continue to die as a direct result of what we did.
We didn’t save lives, all we did was shift the burden of death.
“Now we’re left with a legacy of record waiting lists on the NHS and people dying and will continue to die as a direct result of what we did.”
So TPTB got their intended result.
Record waiting lists are a feature of ‘Our NHS’ but the dullards in the population are just noticing.
Don’t overlook an extraordinary absence of sick people for a supposed pandemic caused by a fast spreading, virulent virus affecting all ages.
For every hospital case there should have been hundreds of thousands not sick enough for hospital but sick enough to stay home.
Where were they?
I’ve seen more sick people during the normal Winter Cold and ‘flu season.
I was in Sweden a month ago and Covid definitely felt very ‘done’ there. Hardly any masks (fewer than in London) and few signs. Local sports centre had some pro-vaxx signs up. Hardly ever came up in conversation.
Point being, because Covid was a much less societally traumatic event than in the UK (in Sweden everybody seems to think we Brits were locked into our houses) it is less embarrassing to admit error in certain areas. Hopefully they will be able to take a more objective view on lockdowns and vaccines.
Unfortunately, Sweden lost it’s way at the end of the pandemic, with mask and vaccine mandates in certain areas (fairly limited I think, but still). Not coincidentally this was brought in by the new female prime minister, who needed to get her virtue signalling in before it was too late. Pathetic really.
Hey all 👋🏻There is a teacher who was written a honourable piece in todays daily sceptic. He says he is alone can we let him know he isn’t. He is was brave in his stand!!!
Todays x please go and read and lend support
Oh I have seen it put on earlier .. support has been given that’s nice 🙂
Looks like even the cherry-picked Nordic comparisons haven’t aged well at all. Denmark and Sweden had the same excess death rates, and Finland was likely not far behind either. And of course Sweden’s Baltic neighbors (for whom there is no non-arbitrary reason to exclude them from neighbor comparisons) did far worse than Sweden or any Nordic country, as did their quasi-neighbor Germany. That leaves sparsely-populated and peripheral Norway as the real outlier, not just for their region, but globally as well. And for most of the pandemic, except for a few weeks here and there, they were overall either less stringent or no more stringent than Sweden, go figure.
As for the other global outlier, Iceland, the closest neighbor comparison would be the Faroe Islands, who were even less strict than Sweden, and ended up doing quite similar to Iceland in terms of death rates.
Game. Set. Match.
Kinda like how Belarus, Nicaragua, Tanzania, Brazil, and Uruguay all had similar or lower cumulative excess deaths compared to the average of their neighbors as well.
A lot of people don’t seem to like the term “herd immunity” because they don’t like the word “herd”. Well, we can always call it saturation, viral burnout, collective immunity, community immunity, collective resistance, endemicity, etc. instead. Or we can call it “The Final Countdown”, like the famous Swedish song.
(By that I mean naturally, since the jabs have proven far too leaky and narrow to do the job. Kinda like flu jabs, but a fortiori here.)
Either way, Sweden proved that it is really the only way a pandemic like this can end for good, at least once the genie is out of the bottle and it cannot be contained. Sweden admitted it from the get-go and got it over with sooner, while Denmark denied it and merely delayed the inevitable. And yet they both ended up in the very same place regardless.
What we need now is for scientists and politicians in countries that imposed lockdowns to officially recant. If one country does it, perhaps others will follow. It will not take much. After all these supposedly intelligent people shut down their entire societies simply on the basis of a news story in Italy, blind faith in China’s response and Prof Ferguson’s dodgy maths.Aka as panic.
Excellent article, but how did these economists compute excess mortality?I see that the Economist’s chart of excess mortality during the pandemic (https://www.economist.com/graphic-detail/coronavirus-excess-deaths-estimates) shows the cummulative rate for Sweden to be about 125/100K versus Denmark’s rate of about 65/100K. I went to the original article in Berlinggske, but it’s paywalled.
And, to follow up my comment: I realize that this article refers to excess deaths in 2020 and 2021, but the Economist chart shows that Denmark’s excess mortality was well below Sweden’s throughout those two years. The graph shows that in 2022 Denmark has suffered more excess mortality than Sweden, but the cummulative rate as of now is still only half of Sweden’s. I’m not arguing that Sweden made a mistake — as other commenters have noted, it did better than most of its neighbors. But I’m not clear how these economists quoted from the Berlingske article came up with the conclusion that Denmark and Sweden had equal rates.