
The ONS announced last week that there were 43,081 deaths registered in England in February, which is 6,700 fewer than in January, and 7.2% less than the five-year average from 2016–2019 plus 2021.
Age-standardised mortality rates for leading causes of death other than Covid were again below their five-year averages. Though recall that the ONS now uses a new baseline for the five-year average, meaning that the latest figures are not directly comparable with those for previous months.
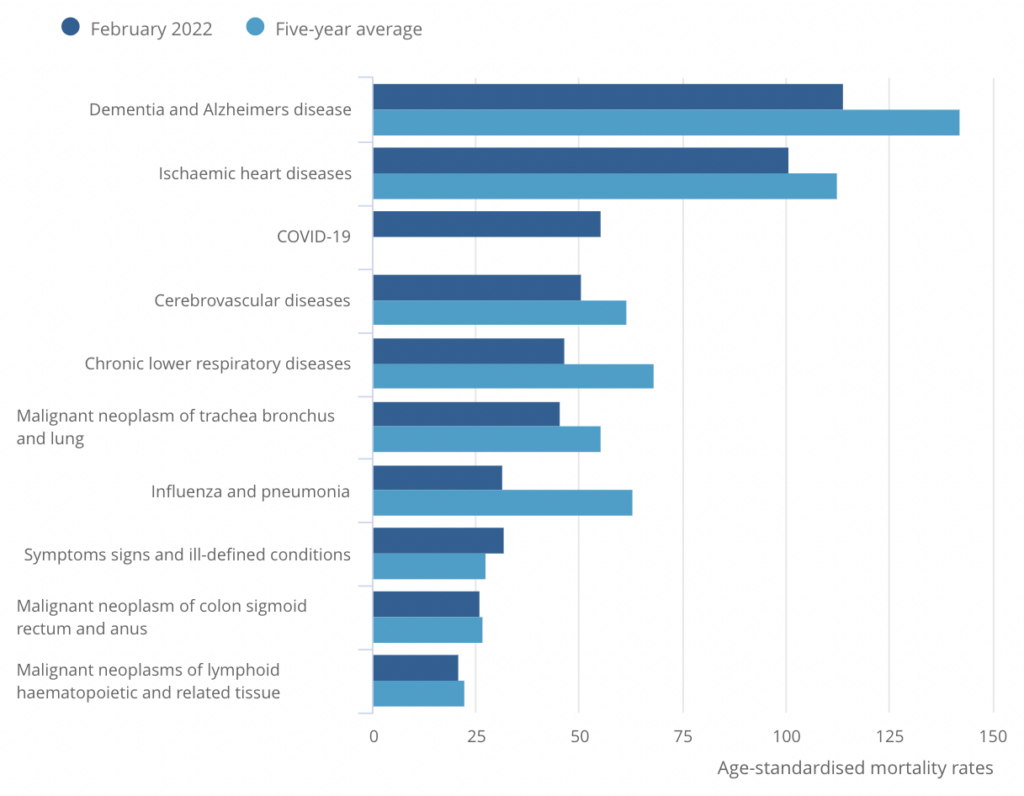
For the sake of consistency with previous posts, I will use the five-year average from 2015–2019 in the remainder of this post.
February’s overall age-standardised mortality rate was 10.1% lower than the five-year average, and the second lowest on record. This represents a continuation of the trend from January, which also saw the second lowest age-standardised mortality on record for that month. Here’s my updated chart of excess mortality in England since January of 2020:
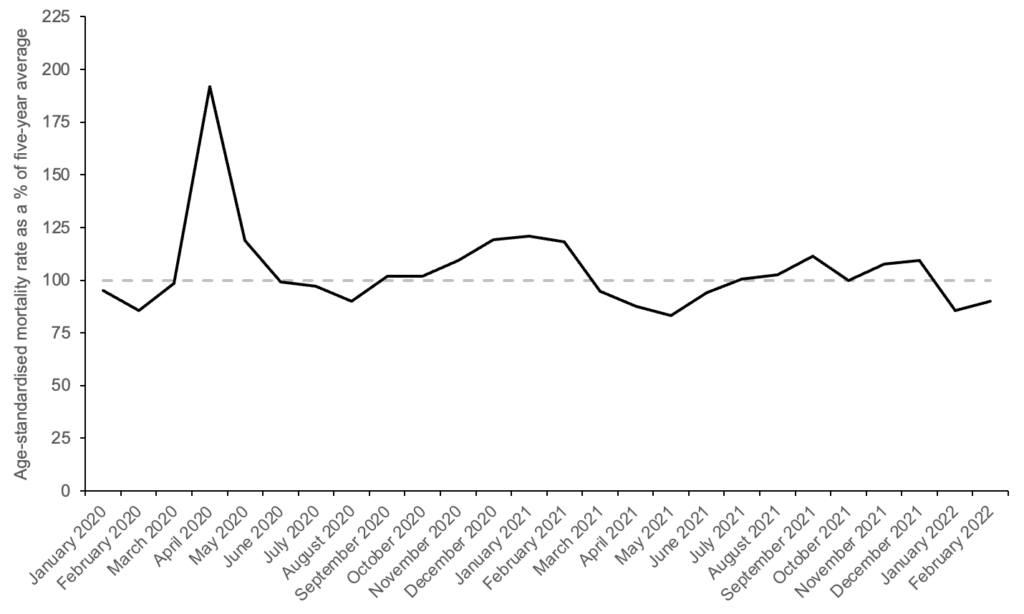
The fact that excess mortality has been substantially negative for two consecutive months is a strong indication of mortality displacement – that deaths were ‘brought forward’ by the pandemic.
If you take the average age-standardised mortality rate from August of 2021 to February of 2022, and compare it to the five-year average, there was zero excess mortality over this time period. In other words, there weren’t any excess deaths in the Delta or Omicron waves.
And if you perform the same calculation for the period since June of 2020, excess mortality was only 1%. This is despite the fact that England’s official death toll increased by more than 100,000 over that period.
Infections have been rising steeply in England for the past month, which could portend a rise in mortality. On the other hand, they’re still lower than the peak in January – a month when, as we’ve just seen, excess mortality was substantially negative. So it seems unlikely that March’s figure will be much greater than February’s.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Looking at that graph, what i can see is the absolutely normal slight rise in deaths during winter, and slight fall in summer, all clustered around the mean.
The only outlier, of course, is the pear at the beginning of 2020, when old folk were rushed out of hospital and rapidly killed off to make way for the expected rise in deaths which never materialised.
Interestingly, I cannot see any long-term rise in deaths due to the removal of cancer treatmants and other general NHS services yet. No doubt that will become obvious 10 years down the line….
Or maybe the NHS not only cures people but also kills them and the net effect is close to zero.
This isn’t a flippant comment. Many people die as a result of medical care. I wonder how hard they’ve tried to establish the net effect.
Actually, how much of NHS care has virtually no effect?
How many people visit the NHS who don’t really need any care or would have just got better at home?
How many resources are spent on short extension of life for people who are about to check out anyway?
And how much time and resources are spent on people who just have such destructive lifestyles that the care provided is almost pointless?
My anecdotal evidence from speaking to doctors I know is that the answer to each of the above is ‘a lot’.
I think there is a lot to this.
And how many resources spent on screening? The question never asked is how many screening tests to save just one life and at what cost? And when the screening turns up a positive, the individual just joins the queue and probably dies waiting.
I wonder if they have data on how many people must be fully vaccinated to save – well in reality, delay – one death where Covid is somehow implicated? And at what cost?
I believe the actuarial cost put on a life is £6 million, but will decrease with age. So if it costs more than £6 million to save a life, don’t do it.
The Pfizer trial (that they manipulted the living daylights out of to gloss the turd that is their product) claimed that one person died of covid19 in the vaccine group and that two died in the placbo group.
Ignoring the fact that these determinations of death were completely subjective we can say that you have to inject 22 000 people with this warp speed product to save one life from covid19, this is the best case scenarion giving Pfizer (a repeatedly convicted criminal organisation) the benefit of huge amounts of doubt.
So, where does that leave Nazanin Zaghari-Ratcliffe, and the £400M cost to the British taxpayer?
🤔
They didn’t pay up for Nazanin. They paid to get access to oil that might be in desperate need soon. Especially if the idiots start a conventional world war.
The bigger the organisation the more political.
They already shut off certain screening programs after a particular age. In my case, I just received a letter from the NHS bowel cancer screening program (which at least shows it’s back in action now), and it states that it is done between ages 60 and 74. So presumably, it’s not worth worrying about (financially) after 74.
I might have a long-term progressive neurological condition, which I have symptoms for six years. However there has been no progression in part because I have used supplements (and am reasonably otherwise fit). Many of the prescribed medications for this condition have horrendous side-effects – yet still these are prescribed due to no doubt some big pharma sales pitches and a few randomized controlled studies. The conclusion I have reached is that almost all illnesses are better controlled by diet and supplements than by anything that big pharma pushes. The recent vaccines and statins are the obvious examples of medicines gone bad. Omeprazole is another. Side effects include stomach cancer and low iron levels. But if you have reflux ( and many do) have you tried Orange Peel Extract? Works better and for longer.
It does make you wonder if trial costs are regulated higher in order to prevent competition to patent rent-seeking drugs.
No you are not flippant.
Waiting lists are the NHS preferred instrument of culling.
Most life shortening diseases come with advancing years: diabetes, dementia, cardiovascular, renal, cancers, for example.
Going through the diagnostic process in the NHS takes months/years waiting to get tests done, waiting to get results, waiting to see specialists cancelled appointments, and often people present with more than one disease. Then once there is a diagnosis, on the waiting list you go for treatment, often delayed, rescheduled.
Many die waiting, if not from the specific disease, then some other cause maybe just old age. The general rule is shove them on the waiting list until they become urgent, then they become emergency admissions and probably don’t make it or survive long.
This is well understood in the NHS.
Indeed, our Envy of the World is set up to create work for itself, not to deliver healthcare to patients.
There are many things to criticise in more commercial systems, but at their core they are in the business of actually providing healthcare services. That has its own problems with unnecessary over-medication, but it also means that when you actually need care, you’re more likely to get it.
Canadians are flocking to the USA to pay for treatment, for example.
It would suit a lot of “leaders” if the hoi polloi (useless eaters) didn’t live so long. Waste of the coming UBI and they already have a pension problem.
And in some places, if you can afford it, and/or have private insurance, you can often see the same specialist, almost literally next door, and come off the list, or not even go onto it. I can remember doing this when in a job where I did have private, and my GP referred me to such a person who worked for both hospitals in tandem.
Shhh… its the chemo and radiation that kills you just as much as the cancer but the chemo and radiation generates lots of profits.
My Mother put her foot down after her second chemo session and said “no more.” That was four years ago. She’s still here.
Cancer treatments and care homes are the preferred methods of stealing all the money from older people at the end of their lives, obviously we can now add covid vaccines to that list.
Non toxic anti cancer treatments have been developed but they are very cheap to produce, can not be patnted and the MHRA always prosecutes anyone that produces anything that risk replacing the chemo/radiation finacial bonanza.
https://www.ukcolumn.org/article/gcmaf-and-persecution-david-noakes-lyn-thyer-immuno-biotech
Here is a chart of ASM (age standardised mortality) for England since 2001. Much easier to see what is happening by looking at individual years rather than averages.
Certainly ASM running quite low at the moment.
Note ASM reflects mortality in the oldest age groups as that is where most of the deaths are, so changes in working age mortality don’t really visibly show up in the ASM.
Reflects that many older people died in 2020 and 2021 due to the disastrous pandemic response, and to some extent genuine covid in April 2020.
Replace genuine ‘covid’ with injection of Midazolam in the older folk and you’ll be closer to the truth!!
This seems to point to dry tinder effect. What this doesn’t seem to show though is excessive vaccine-related deaths, and yet in the US, I’ve been lead to believe that there is very significant excess mortality amongst millennials..? Why would that not be true here?
I wonder how the charts would look separated into age bands. It may be that there is excess mortality in younger age groups that is offset by a dry-tinder effect in the elderly.
It would be more than offset: v few people die per 100k in younger age groups. You can double the number of teenage boys dying and it’ll be like 100 extra deaths or something (that order of magnitude anyway – it’s a tiny fraction), while just under 1pct of all people in the UK die each year – the vast majority over 65 and a lot much older than that
Maybe it’s the calm before the storm. We are behind Israel
That’s the worry.
Only time will tell if the vaccines are as dangerous as suspected. But … that assumes access to good data without that we will never know unless people are dropping like flies. There does seem to be a lot of unexpected deaths but it could be because we are sensitised to it.
You have to look at excess deaths within an age group and for the conditions, such as cardiovascular deaths, associated with vaccines. It is possible to have a headline no change in all cause mortality but changes within categories. For example, if 10 fewer die of X and 10 more die of Y, the overall figure is no change.
Younger people tend to have higher accidental death rates, but if young people are dying from vaccine injury, then clearly they won’t live to die accidentally.
I think Freecumbria’s comment is a likely explanation: you can have a large excess of deaths in the lower age ranges, but because the absolute numbers are greatly outweighed by the elderly dying, it doesn’t show up in the overall charts, especially when the lower deaths among the elderly push the line down.
So age banding, as TheBluePill says, is essential – though life insurance figures and so on can also show the effect.
“This seems to point to dry tinder effect.”
If you look at the 18 months prior to Spring 2020, that’s exactly what you find. Ie, the uptick in April 2020 pretty much soaked up a lot of earlier dry tinder (the numbers had been below the long-term trend for whatever reason).
I’ve no idea why people don’t make more of this, and always start the data analysis in Spring 2020; that seems to me to be deliberately misleading if one is trying to put Covid into some sort of wider context.
Was covid a societal emergency?
No.
Covid was a profit opportunity.
So, on the one hand, claims about life insurance payouts; on the other hand there’s this stuff. I am beginning to suspect a fiddle with the age standardisation process.
If we’re talking about the significant rise in deaths among younger people noted by actuaries, bear in mind that in absolute terms it’s still very small. It’s still mostly oldsters who are failing to dodge coffins.
That’s not an excuse for the crime of each and every clot-shot or coronary-jab, mind, just that the numbers are low enough that we should be doing proper autopsies and calling murder most foul on them.
There is a lot of the virus about and it will still carry off the infirm, so negative excess deaths is welcome but surprising – and does point to mortality displacement. The 10 years life lost per death on average often quoted was always going to be too high (the paper was fundamentally flawed). I expect mortality to run significantly below the historical average for summer – as this latest ‘wave subsides’. Cancer missed treatments and the effect of health of the economics might show over 30 years.
I do not know if it is possible, but I would be intrigued to see the age-standardised mortality rate for 2020-22 vs 2015-2019 but only for under 65’s
How deadly exactly was Covid for working-age adults and children. I think I know, but it would be good to have the data.
It became a lot more deadly after the magic sauce was injected into them.
Without some record of how much the ASM typically varies from the 5 year average, to say it is 10.1% lower is fairly meaningless. Noah’s chart suggests that there is nothing particularly noteworthy about the Jan, Feb figures.
This represents a continuation of the trend from last month, which also saw the second lowest age-standardised mortality on record for that month.
So one month’s data was a trend? A second month which has a slightly higher excess ASM is a continuation of the trend?
I guess it’s just underlining that nothing exceptional is going on, which other than a brief spike in 2020 has been the case all along.
I always thought those in power would have a problem with putting on a pandemic show.
Given that medics are a leading cause of death, often thought to be the third leading cause of death, scaring people away from hospital would probably result in lots of people that the medics would have normally killed living.
This is a nuisance when you are putting on a pandemic show as you want the deaths but you also want people to be afraid, what to do?
‘Doctors withdrew their labour, in the different strikes analysed, from between nine days and 17 weeks. Yet all the different studies report population mortality either stays the same, or even decreases, during medical strikes. Not a single study found death rates increased during the weeks of the strikes, compared to other times.’
https://www.huffingtonpost.co.uk/dr-raj-persaud/when-doctors-go-ostrike_b_1513689.html
I suppose they just have to offset the lack of normal killings the medics would achieve by cranking up the deaths from ventilators, midazolam and overdose prescriptions of HCQ, there just is no other way around it.
Granted, losing the medical profession does get rid of a major cause of death. But that was balanced by the introduction of a lethal vaccination which everyone had to take….
A cynic might observe that they will use it as an excuse, or reason, to cut back expenditure on the health service, on the basis that the ‘cure’ is worse than the problems.
SAGE, the MHRA, the WHO and the UK government all realised that a disproportionate number of the vaccinated are dying so they have redefined death (for the vaccinated) as being a really big lie in.
There we are, problem solved.
The down side is the UK productivity figures are looking worse than ever.
‘Damn those work shy Brits’ said Boris.
Getting everyone to stay at home did limit the normal spread of cold and flu viruses.
Now that people are going back, I see that almost everyone is coming down with sniffles and sore throats of some description.
This whole episode is a big mess….
And this is how future historians will judge us: morons like Sturgeon still claiming an “emergency” with the lowest ever death rate.
How much of the Covid-19 is mis-diagnosed influenza and pneumonia??
A breakdown by age for mortality would be of interest. We keep reading about the 20-60 year olds dying post vaxx from cardiac incidents. Life insurers seeing a significant payout in this age bracket. Would appreciate your thoughts Mr. Carl.