It is said that people can only worry about one thing at a time; if so, then I’m sure that few people are currently worrying about the recent increase in Covid cases in the U.K. This is a good thing – the hospitalisation and mortality rates of Omicron appear to be significantly lower than those of previous variants, so it’s surely time to just accept Covid as another type of cold that’ll give us all an annoying sniffle every couple of years.
But the sticky problem of the vaccines remains. Do they work or have they made things worse? Luckily, the UKHSA (just about) continues to publish the Vaccine Surveillance Report and as a result we can explore how the vaccines are impacting on Covid in England.
Cases
The new Covid wave, as defined by data from the Government Covid dashboard, appears to be gathering steam with new cases hitting 100,000 per day; it is easy to forget that the terrible Covid wave during January 2021 peaked at around 60,000 new cases per day (though this was admittedly before mass lateral flow testing had been brought in). We’re told that recent variants are nearly as infectious as measles – ignoring the surprisingly low household infection rate of Omicron variant, which doesn’t support the measles comparison. What do the data say?
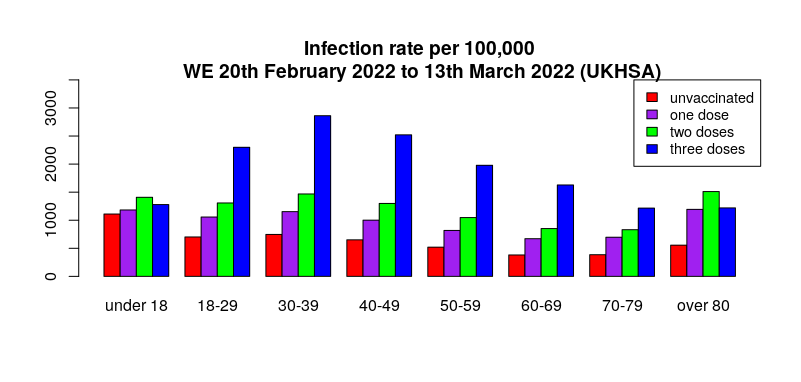
Yet again, the real-world data suggest that infection rates are generally highest in the triple vaccinated, with the lowest infection rates in the unvaccinated (see here for details on methodology and limitations). Could it be that the evidence for Omicron variant being as infectious as measles is only found in countries with high vaccination rates?
The delayed nature of the UKHSA data meant that in last week’s report there was no sign of the then emerging Covid wave – the question is, can we now see the latest Covid wave in the UKHSA data? Looking at all the weekly totals for all Covid cases there’s a hint of an uplift for most age groups in this week’s report.
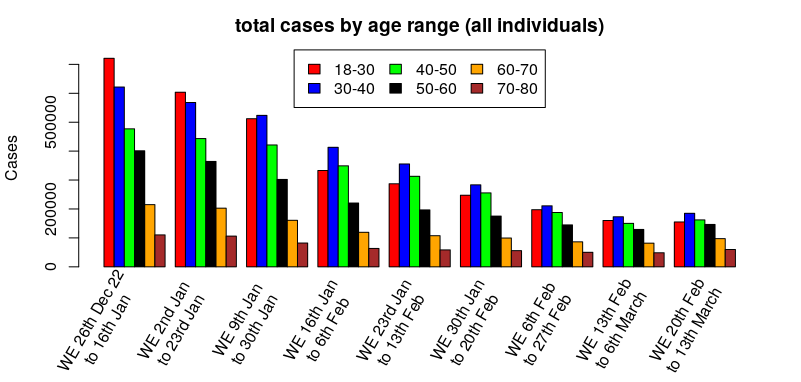
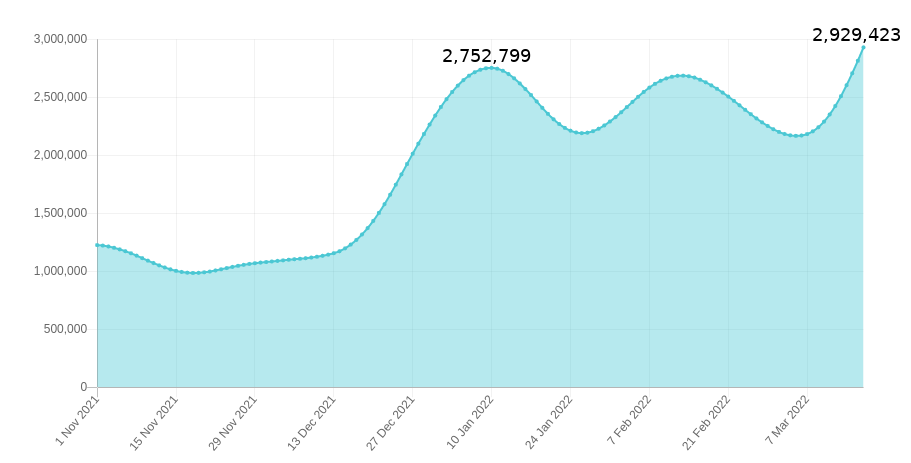
Hmm. The cases have definitely dropped significantly since the beginning of the year, but it’s a bit difficult to see if it is turning around – how about looking at the percentage change by week, that is, relatively how many more/fewer cases there are compared to the previous week:
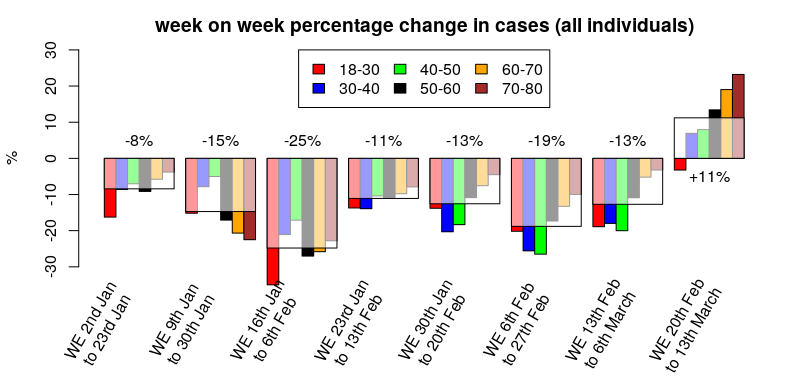
That’s better – cases appear to have been dropping since the start of the year, but this week’s report suggests that the reduction in overall cases has stopped and perhaps the start of the new wave can be seen at the far right.
What about by vaccination status?
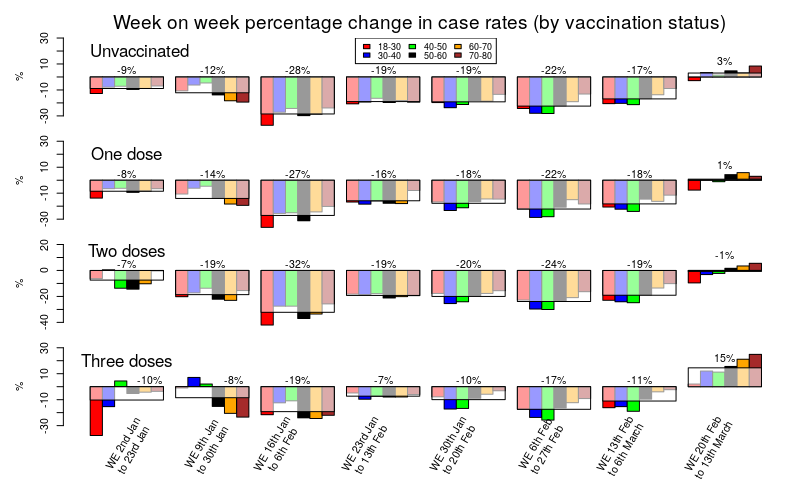
Hmm. That’s a busy graph, but perhaps if you stare at it for long enough a general pattern should become visible.
The change in cases for the unvaccinated, those with only a single vaccine dose and those with a double vaccine dose are very similar; a sustained reduction in cases since the start of the year, but with cases remaining broadly flat in this week’s data compared with last week’s.
Three doses of vaccine show a very different picture. Compared with the unvaccinated or those with one or two doses, the data for three doses show a much slower rate of reduction in cases, with generally about half the rate of reduction in cases compared with those that had taken fewer doses. Also note that this isn’t simply because the triple vaccinated had fewer cases; a glance at the cases graph earlier in this post clearly shows that case rates in the triple vaccinated are still higher than the unvaccinated, and previous posts have shown similar data for earlier time periods.
The big difference in the triple vaccinated, however, is in that final time period on the graph above (the column on the far right); in the latest data we can see that case rates have recently been broadly flat in the unvaccinated, the single dosed and the double dosed – but in the triple vaccinated we see a significant (15%) increase in case rate. It is noteworthy that the triple vaccinated make up the majority of the population for most age groups; are our new Covid waves being driven by the triple vaccinated?
These are still early days in the progression of the current Covid wave and this analysis should be regarded as preliminary – next week’s data should be interesting, if they provide it…
One more note on cases. I mentioned last week that the Zoe symptom tracker was disagreeing with the UKHSA and U.K. Government data on the drop in cases that we’ve seen over the last two months. The Zoe Symptom tracker has seen a sustained level of cases during that time (I have hypothesised that this is due to the 90 day exclusion period in the UKHSA data that would remove any reinfections). I mention Zoe because Thursday marked the point where the Zoe app’s estimate of the number of individuals currently infected with Covid in the U.K. exceeded the case rate during January, and with no sign yet of the increase in cases starting to reach a peak.
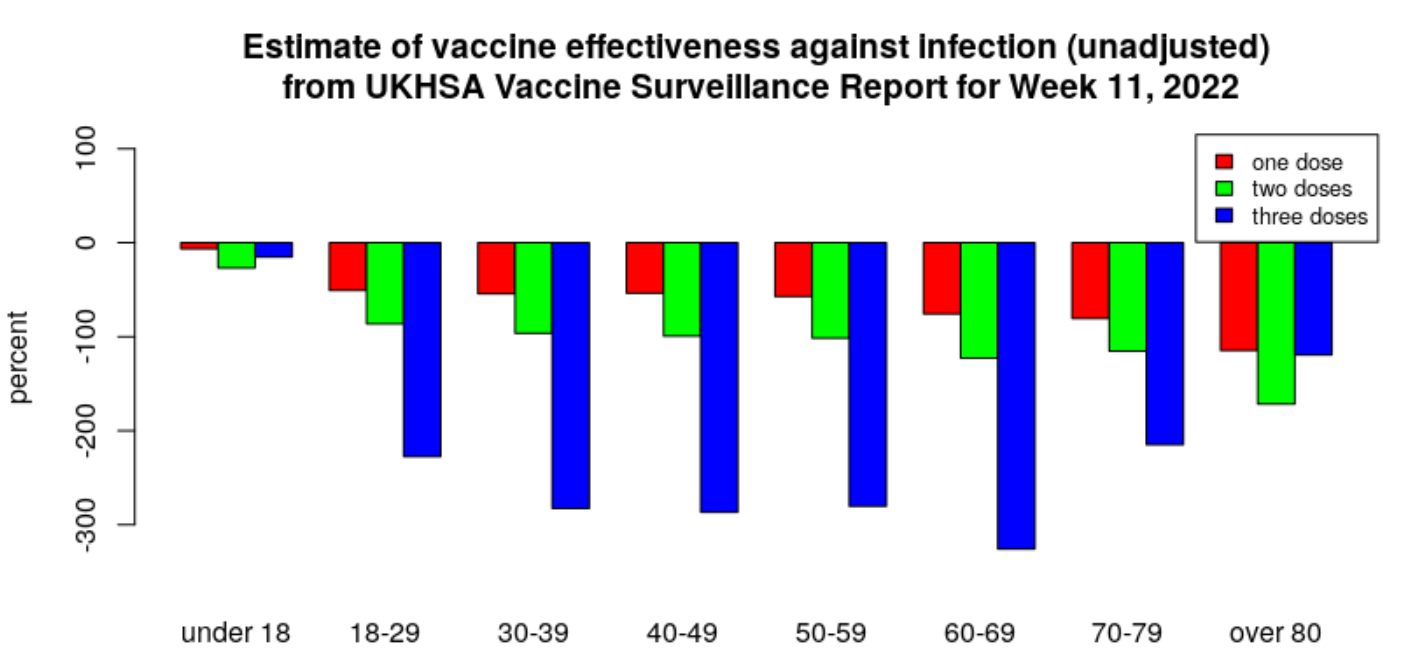
For the historical record, this is the current estimate of vaccine effectiveness according to the UKHSA data.
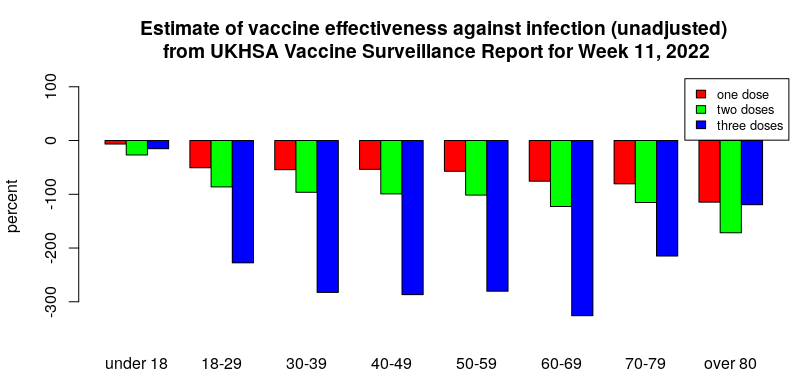
All are negative, meaning the infection rate in the vaccinated is higher than in the unvaccinated. It has reached as low as minus 300% for the triple-jabbed aged 30-70, with those in their 60s faring worst of all, meaning these groups are more than four times as likely to test positive as their unvaccinated counterparts.
Hospitalisations
The Covid vaccines appear still to be offering some protection against hospitalisation after Covid infection for those that were recently boosted, but the hospitalisation rate in those that stuck with one or two doses of vaccine is now much higher than that of the unvaccinated.
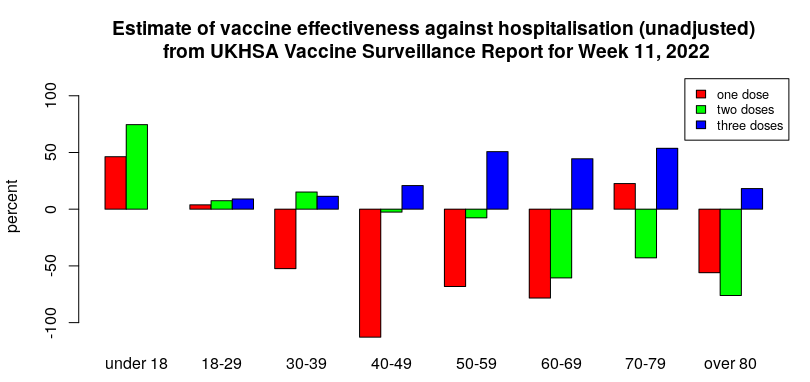
I’d note that it is possible that the higher risk of hospitalisation in those having taken only one or two doses of vaccine reflects them being more vulnerable than average (and thus passed over for the booster dose). If so, this ‘healthy vaccinee’ effect implies that the vaccine effectiveness against hospitalisation and death will be overestimated. That said, there remains the possibility that waning vaccine protection starts to be associated with increased risk of serious disease (possibly via antibody-dependent enhancement (ADE) mechanisms, which often only appear when the initial immune response starts to wane). It would be useful if some research was undertaken in this area.
An important aspect of the above graph is which age groups get the benefit of reduced hospitalisation after vaccination. The age group from 50 to 80 appears to have a reasonable level of protection (about 50%) and this might well support vaccination in that age range for those that are happy to keep on taking booster doses indefinitely (dependent on side-effect/complication rates). Protection in those aged over 80 appears to be poor – this is unfortunate as it is that age group that gets the largest share of hospitalisations and deaths. I also note that there appears to be very little reduction in hospitalisation in those aged under 50; it is questionable whether this level of reduction is at all relevant for younger individuals.
Deaths
The UKHSA statistics for deaths within 60 days of a positive test show a similar trend for the effectiveness of the vaccines to that seen for hospitalisations (only data for those aged over 40 are shown – Covid death rates are too low in those aged under 40 for meaningful analysis).
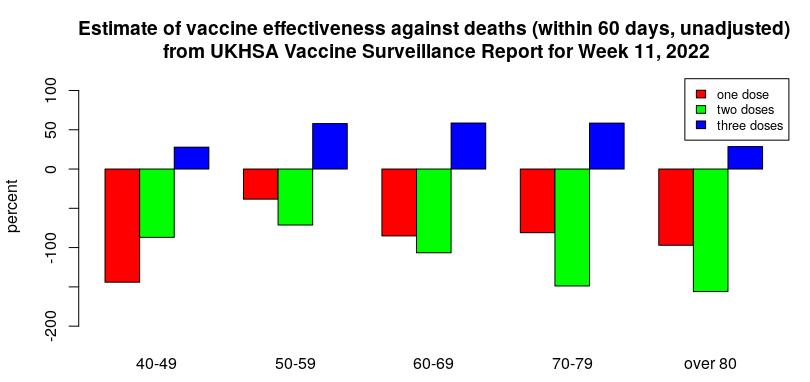
It is important to note that deaths with Covid have reduced significantly since the Omicron variant arrived. Thus, despite the apparent protection against Covid death offered by three doses of vaccine, it is questionable whether there is now much in the way of absolute, real-world benefit.
There is a worrying trend in the deaths data, however – the change in distribution between deaths within 28 days and within 60 days.
Historically, most deaths with Covid have occurred within 28 days of infection. However, there have been some additional deaths beyond this point; in general, each week’s report has seen an additional 20-25% deaths with Covid between 28 and 60 days after infection.
Over the past few weeks, the proportion of deaths with Covid in the 28 to 60 day period after infection has steadily risen until it accounts for approximately as many deaths again, as seen in the graph below.
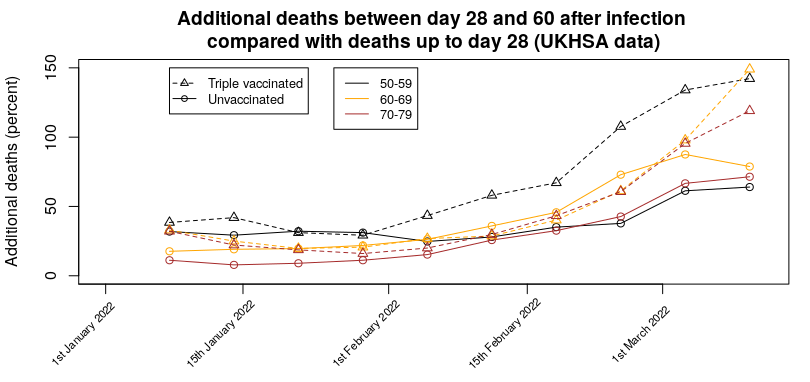
Even worse, there appears to be a vaccine effect, whereby there are more additional deaths in the triple vaccinated group (approximately 140% of the 0-28 day deaths in the latest report i.e., nearly one and a half times as many deaths occurred in the 28-60 day period as in the 0-28 day period) compared with the unvaccinated (approximately 70% of the 0-28 day deaths i.e, the number of deaths occurring in the 28-60 day period was around two thirds of the number occurring in the 0-28 day period). This means that in the triple-vaccinated we’re seeing more deaths with Covid in the 28-60 day period than in the 0-28 day period. This effect is also visible in the data for one or two vaccine doses. For the most recent week the day 28-60 deaths are 130% (single dosed) and 170% (double dosed) of the 0-28 day deaths.
It isn’t clear whether this effect is due to infection with the Omicron variant taking longer to get to the stage where hospitalisation is required, people remaining seriously ill inside hospital for longer, or more people dying outside hospital. It is also possible that this effect is due to changes in treatments being used in hospitals.
Given this effect, it is likely that the current ‘official’ death figures for Covid are now lower than they should be (though I note that ONS excess death estimates have also been low since Omicron arrived), and that official estimates of vaccine effectiveness against death will overestimate the protection offered.
Another interesting effect seen in the deaths data is the ratio between the deaths rate and the hospitalisation rate.
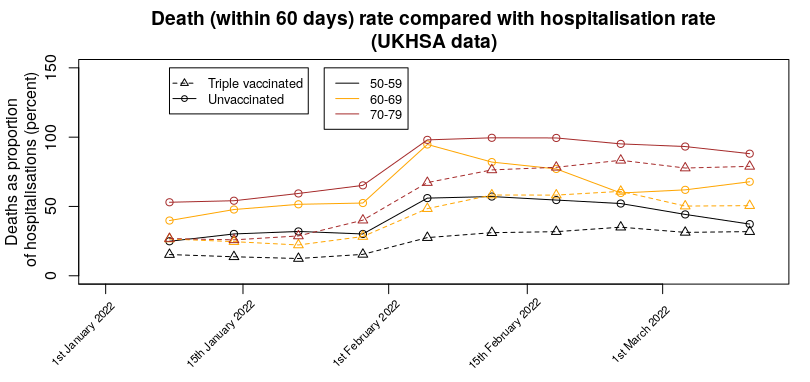
There does seem to have been a change in the number of deaths compared with hospitalisations over recent weeks, with a marked increase in February, so that more are dying per hospitalisation. It is unclear why this has happened. Note that is isn’t simply the hospitalisation death rate – many deaths with Covid appear to be occurring outside a hospital setting. This effect is seen most clearly in the proportion of deaths vs hospitalisations for one and two doses; for those aged 70 to 80 there are more deaths than hospitalisations (about twice as many for a single vaccine dose, about 50% more for the double vaccinated).
One more thing…
Arguably, the most important news in this week’s UKHSA Vaccine Surveillance Report was buried in the text (my bold):
From April 1st 2022, the U.K. Government will no longer provide free universal COVID-19 testing for the general public in England, as set out in the plan for living with COVID-19. Such changes in testing policies affect the ability to robustly monitor COVID-19 cases by vaccination status, therefore, from early April onwards this section of the report will not be updated. Updates to vaccine effectiveness data will continue to be published elsewhere in this report.
This was probably inevitable – the real-world data on the vaccines are consistently failing to support the Government’s position that the vaccines have actually helped significantly. While the excuse given appears reasonable at first glance, a few minutes thought reveals it to be weak – while there might be issues with overall cases and testing, testing at hospitalisation and to a certain extent death will continue. In addition, it is likely that routine testing of healthcare workers will continue for some time. It would have been trivial for the UKHSA to have continued to show data for hospitalisations and deaths and included a section on case rates in healthcare workers. But instead they’re using the occasion as an excuse to remove all data. I also note that the Zoe symptom tracker app has lost funding – their data were also going against the official narrative. Thus, like tractor production in the Soviet Union of old, the only statistics we’ll be allowed to see are those that aren’t inconvenient to the state.
Hopefully we’ll get at least one more set of data to see how the impact of the more recent changes outlined in this post have played out.
Amanuensis is an ex-academic and senior Government scientist. He blogs at Bartram’s Folly.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
*Not* Cassandras! As many of us pointed out yesterday btl, she predicted the truth but was doomed to not be believed. Sage etc are exactly the opposite. ( It’s us Sceptics that have been the Cassandras ).
NB. You need to edit; “poured” ( para 6 ) should be “pored”, and you’ve written “their” instead of “they’re ” higher up ( 1st para ).
That would be a quantum leap of progress.
So true! I remember posting on FB a while back asking if there were any other Cassandras out there, meaning – like US, not the SAGE scientists! Cassandra made ACCURATE prophecies (that weren’t believed).
Cassandra was cursed by Apollo for having spurned his advances. We can all relate, I’m sure, to the terrible burden of knowing what’s coming and not being able to get anyone to believe it. One of her first prophecies was of the Trojan horse. A gift which is received with gratitude but contains something deadly.
There’s a great comic strip in which Cassandra exacts a kind of revenge on Apollo. Sadly I can’t find the original.
I remember when Toby insulted us all for questioning the vaccine. In the end he changed the name of the site, Cassandras indeed.
You can just feel that they are going to impose restrictions again can’t you. It might be my usual negativity but there is no way they are going to let things continue like this and a lockdown will come once again.
The only thing we have in our favour is the fact that this will perhaps wake a few more people up .. Maybe…
I personally have the same sense of doom as in April 2020 when it became quite clear that the coronavirus circulating was not anywhere near as dangerous as governments and media were saying and still we continued on the same trajectory. The lack of course correction in the face of clear evidence made me realise something else was at play.
This winter feels the same. This thing being called Omicron is a joke as far as a threat to health goes and there is complete disconnect between the medical threat and the measures being imposed and the fear being promoted.
It just doesn’t make sense. What is behind it is mere speculation, but what we can say without any hesitation is that this just doesn’t make any sense whatsoever. And if I know it, those running the show know it.
I am absolutely certain based on reports from funeral homes in different parts of the country that the excess deaths we had in January and February of this year, were due to vaccinations of the most elderly.
A number of funeral homes reported their busiest ever months during that period, and it just coincided with mass vaccinations of the most elderly people.
The purpose of a lockdown now appears to be motivated by the order they have received to implement the vaccine passport, which will later become the CCP social credit system. You cannot introduce something like that unless you create a crisis. The issue they have is that just dont have the data to justify it, but that hasnt stopped them so far.
Not saying you are wrong but
I was out and about 7 days a week as a ‘key worker’ for 12 months from March 2020. There was no increase in activity by funeral parlours evident on the empty road. It would have been very obvious with the empty roads. Funerals were not banned, just the number of mourners greatly curtailed.
They never used the designated Super Morgu (an out of town coverd Go Cart track), nor the Covid Recuperation Hotel and the didn’t start the local Nightingale until late summer by which time the commandeered Nuffield still remained idle.
But they did other things to create a climate of fear, not least having empty ambulances cruising around with their sirens blazing for no good reason (empty roads).
Omicron was a bit of a damp squib – but just wait until you see the next one that will be 77% more contagious than Omicron!!!
It all makes perfect sense to those cashing in from all this. Although you’d think they themselves are subject to travel restrictions, and face mask wearing, and having to see the whole country in abject zombie misery.
You are localising the issue. The conspiracy is global and rest assured those directing operations are neither interested nor affected by the emiseration of national states.
Surely that is a mistake, it could be 66% more contagious or even 666% more contagious it all depends on Neil latest model.
Also as the next variant should be pi, it will be 3.1416….. times more deadly as well.
6pm yesterday. Accidentally caught 30 second intro of ITV 7pm news.
News guy kneeling off studio desk in mansplaining power pose
“New Variant Omnicon surges past (100k?) ! Wales and Scotland impious Xmas sanctions !
England holds firm !
Join us as 7 for the full story”.
What a load of obvious bollocks.
The panzers are coming. Bozo is ready to mobilise Dad’s Army.
“Stand by your beds.”
Bombs Away Monday December 27th.
I haven’t watched TV in over ten years. Doesn’t sound like I’m missing much.
Raise you by five years to 15 (same as BT landline).
As I said, caught by accident so the brazeness shocked.
People fall for this shite?
I remained confident for all of Lockdown Proper and most of Lockdown Lite that the worst was nearly over and that we were on a steady path, albeit slowly, towards Freedom.
Only as they introduced Tiers with the media constantly hyping up the supposed dangers of Covid did I realise there was no end in sight, just like now.
The only puzzle was why?
Only then did I begin to look at what, until then, had been conspiracy theorists and here we are again, over 12 months later.
I believe if Johnson goes for a shutdown anything like SAGE want it would set in motion the chain that would lead to his removal from power later in the year. He will do something to appease SAGE but it won’t be anything like a harsh shutdown. It will either be Sports stadiums or some hit in hospitality, where Rishy Washy again fire up the printers.
Perhaps people will get so angry they’ll write yet another e-mail to their local MP in the hope of getting another copy + paste standard reply.
I’ve noticed a marked change in the response from my MP. (All my communications with her have been courteous and considered.) Last year, she did indeed reply with obvious copy and paste jobs from the Whips’ Office but, this year, she’s simply not responding at all. It’s almost as though she recognises that the wheels are falling off and doesn’t want anything more on the record to embarrass her in the future.
The prewritten responses I get (from the whip’s office) talks of all measures going against my [planted] MP’s ‘natural libertarian’ beliefs and that they’re only temporary. Lots of bullshit about unprecedented times and killer diseases bla bla bla.
He then goes on to vote in favour of everything the government wants.
I always remember the real response I got from him after I was particularly scathing of him and his party. Completely different writing style and a complete lack of professionalism.
It might have been funny had the subject of my email not been so serious; the suicide of a close family friend, undoubtedly due to lockdown/scaremongering.
I found an unsolicited message from my MP in my inbox!
It must have been because I thanked him for voting against VPs but he sent me Xmas greetings and thanked me for my comments.
I must be getting through, even as only a gauge as to what the Lunatic Tendency are thinking (and I’m always civil – I won’t give him an excuse to delete me)
They will mostly be happy to have been permitted a better Xmas than last year.
Canada has just gone into ‘one household at Christmas’ lockdown – exactly the same as last year when they locked down on Christmas Eve. One newspaper headline: ‘The best gift you can give this Christmas? Not infecting others with covid’. It’s so strange how much in parallel this year is with last year and with so many other countries in lockstep and yet nobody seems to remember. It’s as if the financial reset was supposed to happen then and has been put off till now. I’d guess there’ll be an announcement today that we’re reduced to one household from tomorrow – but we could just ignore it.
We can and must ignore it. I will be.
People really do seem have the memories of goldfish.
This past summer Israel pushed the booster shot on the basis that although the vaxx provided super-duper fantastic protection, Delta was a game-changer and necessitated a 3rd shot. Until November here in NL the OMT was still saying 2 shots would do. When this turned out to be nonsense (huge influx in hospital, half were vaxxed) they said a 3rd shot was necessary because of – Delta. Now, without batting an eyelid, the 3rd shot is necessary because of – Omicron.
Of course they will impose new regulations asap.Ruining Xmas was almost a step too far last year.
Now they will probably wait until the extra Bank Holidays, with many people good and sloshed, before cancelling New Years Eve since that primarily only affects younger people.
It would take a very brave Hotelier to have put on an expensive NYE base this year such was the risk of cancellation.
Of course they are going to impose restrictions. How else could they claim later that they “fought” and won against Omicron? In Germany the restrictions were already announced to come in force from 28 December – with no data to support them whatsoever. It’s not like they need any data. All they need is public support.
Yesterday John Campbell showed how Australia has decided to ignore the doom mongers and allow permissive spreading of Omicron in order to achieve herd immunity. Well worth watching.
https://www.youtube.com/watch?v=LVl5OkHcvf4
Sanity has now broken out in Australia, Japan, and South Africa. The results will most likely be dramatic and impossible to cover up. All very encouraging.
It wouldn’t be the first time a government leader makes encouraging noises about living with the virus only to go back and impose measures that look a lot like the pursuit of zero-covid.
Very true. Dutch approach March 2020 – December 2020 was stop hospitals from being overwhelmed, find better treatment, be better prepared. Shops were never shut, schools for about 2 months, primarily because parents refused to send their children, it was not the original decision of the government. No stupid face rags. Life was pretty normal, people who visited all commented on that. I remember the head of the OMT at some point saying it was never the intention to stop people from getting a cold, they just needed to keep people out of hospital.
Since December 2020 the face rages were imposed, there was a night curfew for a few months, shops shut for 5 months, etc. – all on the direction of Berlin/Brussels. I believe it is Germany that decided Europe should pursue zero covid. Let’s face it, not the first time Germany believes that as long as it persists it can overcome anything, no matter how impossible – this would appear to be a fatal flaw in the German character.
Yes Japan and sth Africa but NO Australia – That doctor knows nothing about Australian politics – it’s a federation – scott morrison is another fool who talks jibberish and knows he cannot control state law – there is nothing sane about Australian politics right now – most states have passed pernicious covid laws (especially Victoria) – citizens like me are prevented from entering the country to see my close family etc. without being stuck in a prison for two weeks on arrival and further heavily discriminated about what i can do and where i can go. It is as bad a Canada – some states put you in a detention facility for refusing a test (let alone testing positive)… it is out of control and we cannot stop fighting for our fellow humans. Please don’t misinform people more.
A taste of Covid regulations in Australia:
https://www.reddit.com/r/LockdownSkepticismAU/comments/rmmu3o/fuck_this_cunt_mandatory_masks_and_density_limits/
I rarely still watch John Campell. I found his earlier stuff, like vitD deficiency/covid.
However, he seems unable to deal with the ‘vaccines’ without his bias for them leaking through. Same with masks. And Ivermectin.
One example was the obviously elevated status of his eyebrows, when talking about the remarkable coincidence in reduction case numbers after Ivermectin take up. While being astounded at this very interesting coincidence, he then goes on to say that other things could also be contributors/responsible – the high level of mask wearing, for instance. But, looking at the graph displayed alongside him, as he says this, you think, “okaaay, but of course, they were wearing those masks prior to the Ivermectin uptake …. when the cases were sky-rocketing.
After some positive comments about Campbell recently I went back to have a look – after about two minutes – “our amazing vaccines.”
FFS I thought, must be watching the wrong John Campbell.
Man’s an idiot.
No, he’s not. He may be wrong about some things but he provides very useful information about others.
Bearing in mind, he’s a Nurse, not a ‘Doctor’ in the accepted sense so his analysis must be approached with a good deal of caution.
He accepts, almost unquestioningly, that official data sources are reliable.
Oops, forgot to complete that with the words: to be quite good.
Groan I really must finish my sentences: take up in Japan.
I really must finish my sentences: take up in Japan.
Will this become highly contagious though? We can only wait and pray that is does – obliterating people’s aquired imunity to it in the process.
I can’t see Dan Andrews rowing back on anything. For plenty of Aussies I would imagine he will remain a marked mine for the rest of his life.
‘Sage will look very silly indeed’. Sage have looked very silly indeed from the outset. But don’t worry they will all be Knighted for their services to the ‘Great Reset’. Pat will be double knighted and they will all bugger off with their big fat Pharma cheque.
I think the problem here is that the government will also look “silly” if they don’t have more restrictions now, because it will show that restrictions imposed so far have not been needed. They could use the cover of the jabs, but they could have used them before and they didn’t. Why not?
I really think this presents an opportunity for the government to say it wasn’t us, it was the science/ media who forced pointless lockdowns upon you. This presents an opportunity to highlight that locking down earlier and harder would have made little difference in March 2020, the disease was already endemic before we even knew it was here. It is a load of bollocks of course, but the government would far rather, at a public enquiry, fight a challenge that they did too much rather than they did too little!!!
They’ve had many previous chances and not taken them, though of course it’s possible that pressure from backbench MPs may be forcing their hand now.
However the fact that Omicron seems to ignore vaccines is a double edged sword. In the rational universe, it would be a reason to stop vaxxing people and get back to normal, in the covid universe it’s a reason to keep on vaxxing people.
My thoughts exactly. If you wanted to create a world in which people are vaccinated regularly and were expected to have to justify their “immunity status” with a health passport, you would want:
(a) Vaccines that don’t really work for very long – check
(b) New varieties of virus that “evade” the vaccines – check
Add a complicit media that stirs the public into a frenzy of fear when each variant appears and bureaucracy/government that plays along and you’re all set.
Exactly!
The trouble is Bozo has already stated how brilliant lockdowns have been. The public enquiry will be a white wash and tell us how brilliant lockdowns have been. They want more lockdowns in future for climate change and what ever the next big scarient is. Lockdowns have to be proven to be successful for the public to buy future lockdowns. Hence introducing restrictions when the infection rate is already falling.
Good point. In particular as the ‘scientists’ are trying to deflect the blame for overselling the gunk’s efficiency onto the politicians. Surely the politicians are not amused about that and now eager for a payback opportunity.
Moronic is essentially a common cold variant. ‘Everybody’ gets it. No one dies ‘from’ it. It doesn’t match the 3 genetic sequences of SARS-CoV-2 in contrast to all variants so far. The symptoms are runny nose, sneezing, headache, cough , etc.
To Toby’s point that is more about incompetence than anything deliberate.
What we can’t forget is that we haven’t had a functioning government in the UK for the last 40 years of the EU.
It’s been very clear since the referendum that they haven’t a clue what they’re doing.
Make no mistake, Johnson is a fully paid-up member of team NWO. So if the regime think they can get away with it (and by using that term I mean the entire cross-party political class who are committed to the ongoing coup) they will implement more controls and restrictions regardless of hard evidence or data – because that is what they have always done with the covid hoax, and what they have been doing for decades with the climate scam.
It used to be the case that when people got a cold in winter, they took some lemsip and carried on. If that cold developed into a chest infection, they stayed off work, rested and took medication. If it developed further into flu they would seek antibiotics and if in very rare cases it progressed to pneumonia they would be hospitalised and in some cases, particularly the eldery or vulnerable, they would die. This is still happening today, but the whole process has been co-opted and rebranded by authoritarians to serve ulterior motives, and the public are to shallow to realise this. Now a whole industry has grown up around the deception (from the lowest covid marshall to the Big Pharma executive) and so many jobs rely on keeping the deception going its going to be very difficult to steer the great covid tanker around to get it heading back to where we started..
SAGE and the modellers were already proved wrong this summer and autumn when their predictions about “Freedom Day” were spectacularly wrong.
And many times before that really. They have exaggerated and got it wrong every single time.
What makes anyone think this is the one that would discredit them?
If this crisis has taught us anything is that reality, data and facts don’t count for anything any more. Only power does.
Stewart,
I have been a “Man made Global Warming” realist for well on 40 years. Every single one of the warmists predictions have failed to materialise.
This does not stop the majority of rulers rushing to return the world to cavedwellers by destroying civilisation.
Science is ignored and fortunes are made with lies and propaganda.
Sadly this Chinese flu hysteria is just the second chapter of the scam, and I cannot see any sanity returning in the short term.
So enjoy Christmas, it could be our last.
Funnily I said that to the wife while putting an extra bottle of wine in the trolley and spoiling my self with some rum. ‘This could be our last Christmas’. She gave me a funny look and went to find some cranberries.
Covid will be over come spring/early summer.
Political attention will then zero in on NetZero and the costs are becoming clear. Assuming Boris is still around, there are a lot of back benchers gunning for him already. He would have been long gone were Starmer any good as opposition leader.
Thanks to covid, Boris has little time left to do much about NetZero before immediately facing a general election. He can’t face one with energy prices spiralling out of control and any recent history of black outs etc.
Then there’s China, India and Russia which are clearly not interested in climate change, and even the media are beginning to squeak about that. Biden is having a torrid time over his proposals and his personal position also looks unstable.
Now the green blob, of all people, is up in arms in Australia about wind turbines being built on undisturbed land.
Europe has slapped 19% import tariffs on Chinese made turbines which is not being received well and will impact badly on the cost of commission them, which will be subsidised with Taxpayers money, and the Taxpayers will notice that.
Sales of electric cars are not even close to what is required to meet any emission targets our government has set, despite the subsidies, which our Taxpayers are also beginning to notice.
Finally, there’s the cost of covid which we have no choice but to repay. We have a choice with NetZero.
I agree – I think that they want to ultimately deter people from celebrating christmas – stop the publicans and restaurateurs gearing up for it and offering christmas do’s after this years have mostly been cancelled and stop people making christmas plans by keeping the whole “will family gatherings be banned?” thing on a knife edge until the very last minute.
I am convinced it is deliberate. Religion and christianity, what are left of them now, do not suit the purposes of what is to come.
Well, and we now know that SAGE and the modelers only produce the models and results the politicians ordered.
Stewart, but, to take but one example, Professor Pantsdown Ferguson’ career for around a decade has been one of incompetent computer gaming ‘projections’ using highly improbable assumptions, in order to generate shroud waving and doom mongering.
He’s made a career of it.
That was well understood when he was picked for SAGE. And HMG also knew that “Stalin’s Nanny” Michie was a long term Communist Party of Great Britain Central Committee member. She was appointed and still permitted to piss both out of the tent and from outside the tent (Independent SAGE, the BBC), pissing in.
No worries, no complaints. Imagine the brouhaha if someone had suggested perhaps Tommy Robinson should be appointed…
I’ll believe Chairman Boris ZeDonkey realises he has blundered when, instead of printing more money, he starts printing P45s for those who have led or promoted this scam from the start.
Don’t hold your breath.
They predict the ‘worst case’, and the ‘worst case’ rarely happens. The worst case for a aircraft flight is a total crash and burn. That is so incredibly rare that people don’t even think about it. Almost all flights are totally inconsequential, delays excepted. The ‘most likely’ outcome of any flight is a perfectly normal uneventful flight.
Get SAGE to model airline flights and see what they can do to the airline industry …. oh wait …
Good analogy.
If Johnson holds his nerve he can destroy the argument that he should have “locked down earlier and harder”. If he holds his nerve he can Chuck every last one of Sage etc under a bus. Hopefully Rees Mogg getting off his charge yesterday will harden his resolve to hold the line!!!
What has Rees-Mogg done?
“Borrowed” a fortune against his company and been found by the bould Kathryn Stone to have done nothing wrong.
Ah ok, so you’re saying the him being let off will inspire the PM to see sense?
Reports suggest Rees Mogg, whose fortune is predicated on accurate financial modelling, was the man who really laid into Vallance over the pessimism of the modelling. Just heard some prick modeller on the wireless admitting that the “cases” aren’t rising “exponentially” which he says is down to change in behaviour, etc.
Rees Mogg has been pretty quiet so far and voted with the govts fascist shit every time. Be interesting if he turns.
Follow the money.
Down to change in behaviour – so how does that work, does the virus keep a list of who’s naughty or nice? Do these people really believe the carp they churn out? I’m expecting news presenters to start rolling their eyes when they read this stuff out, it’s becoming so predictable and lame.
I wonder why he did that?
Financial crash looming?
I am quietly hopeful
But, I expect the doom-mongers to say any plateauing of the ‘outbreak’ is due to the doom-mongering causing people to change behaviour – and that we will need lockdown in January to avoid a surge when ‘everyone comes rushing back to work’
Even Owen Jones!
Now we are truly a lost cause as that brain dead little shit weasel is wrong about absolutely everything so if he’s on our side……
He realizes and accepts that public opinion has turned against them, but his solution is to throw more money around to the little people and the beloved NHS and do them regardless.
Not really a convert.
Jones is the ultimate weather vane. Very loose and easily moved by the slightest breeze.
Talking about South Africa, here is an interview of Nick Hudson, founder of PANDAS. The clarity of thought exhibited in this interview is wonderful to hear. For example, his explanation of the motivation of the global elites neatly bridges the Toby/James divide and should really become the position of both.
https://odysee.com/@TLAVagabond:5/NIck-Hudson-Interview-10-7-21:1
I’ve got everything crossed that you’re right Toby.
“not least because senior members of the Cabinet are actually pouring over real-world data for the first time instead of just reading SAGE’s memos.”
If, true (and I don’t doubt it) that is an absolute disgrace. These Ministers are supposed to challenge the Experts and if they have just been meekly accepting the garbage produced by SAGE they have failed the country and are not fit for purpose.
There’s only one thing which will stop Johnson imposing more moronic restrictions …. and that’s the fear of an ever greater rebellion by CON MPs and the possibility of another Ministerial resignation. He’s a coward ….. but a coward who wants to stay in No.10.
Meekly accepting garbage is par for the course – it is exactly how the US Task Force operated under Fauci and Birx (chaired by VP Pence) last year, according to Scott Atlas.
A disgrace, yes. But perhaps a hopeful sign that they now see the writing on the wall and are repositioning themselves to escape blame “well, until Dec 2021 it looked like ….., but now things have changed …..”
Ideally we want these b******s strung up (metaphorically, I assure you) but first, we have to break the cycle.
Bozo is caught between a rock and a hard place. If he gets booted he loses his sinecure, he won’t be popular inside or outside the party and a wilderness beckons.
Bliar has made a fortune but only via wholesale treason. Is that where Bozo is headed assuming the Davos mob will even have him?
I am not for new restrictions however I cannot understand waiting to bring them: if it is that serious, why the wait!
I mean really why?
On a separate note, my husband is going to his family on Christmas Day. I will be with an elderly parent who is alone.
His bloody sister ( think this warrants a mild expletive) wants him to take an LFT test. I despair I really do- if she’s that worried just cancel!!
But that’s not the best bit: she wants him to take it when he’s ALREADY at her place!!
That’s right he is expected to make a 2 hour journey + petrol only to be presumably sent home if it’s positive on Christmas Day!!
I had to be put my foot down on this: a compromise has been reached where he takes one before he leaves.
I’m now working on talking him out of it as there’s no effing way I’m losing out on Christmas at her bequest.
Her initial suggestion was nuts. So nuts I’m actually asking you good people if indeed there IS sense to it that I’ve missed.
Probably so that she can see for herself that he actually took the test, and what the result really is. Her demand makes sense in the paranoid and divided/divisive world of covid, a world in which she doesn’t trust her brother to tell her the truth about covid-stuff.
That makes sense, thanks.
I ‘d thought that myself but, of course, he still has to be sent home if it is positive AFTER he’s actually met people at her’s.
He wouldn’t lie, anyway.
I think she wants to call Christmas off really and he doesn’t particularly want to go so I’ve suggested he just use omicron as an excuse.
Where did she want him to do this test? Outside, before he was even allowed to enter the house? If not, it makes even less sense!
Yes, it is unhinged behaviour.
No covywovy – you’ve missed nothing – your partner’s sister is unnecessarily concerned.
All any test does is to indicate whether someone might have SARS-CoV-2 which can be present in someone who is not necessarily ill and infectious with the disease – Covid-19. In your partner’s case, if he has no symptoms, even if he tests positive on arrival, he won’t infect his sister as he won’t have anything like the required viral load to be infectious. Slice ‘n dice it every which way, if he feels fine when he sets off to his sister – she’ll be fine. The one caveat is that if he’s staying any length of time and there are other guests at his sister’s house, he could catch if from one of them or develop symptoms if he caught it not long before setting off. If he’s just there for Christmas day, his sister has absolutely nothing to fear from him. Furthermore, unless she’s elderly and/or has a comorbidity, the only thing she’s infected with is fear itself; the virus presents minimal danger to her as her chances of survival if she caught it is well in excess of 99.7%!
There is a bigger dinner party on Boxing Day. But he has actually suggested to her that he leaves early on Boxing Day. She said no to this so go figure.
I’m still annoyed, though.
These LFT’s are not particularly accurate and I believe that people should either just go ahead and enjoy Christmas free of Covid- related stuff or just cancel it if they’re that bloody bothered.
Taking LFT’s on Christmas Day for heaven’s sake!
Is this a class thing? They’re very, very middle class – betcha working class and upper class people won’t be taking LFT’s on Christmas Day!
Disclaimer: I am NOT saying ALL middle class people are like this but the ones who WILL be taking LFT’s on Christmas Day are.
Hold on. He’s chosen his sister over you? I’d pack him more than an overnight bag.
If you mean he’s chosen to spend Christmas with her as opposed to me, that’s wrong as he’s only really going to see his elderly mother.
We agreed all this months ago.If however you mean he’s meekly going to take an LFT test at her bequest thus ruining my Xmas for no good reason if it happens to show positive but he’s asymptomatic you may have a point.
Not forgetting the isolation period.
I’m beginning to hate this woman.
I don’t see why he can’t leave on Boxing day morning, though! His sister says no! It should be his decision, should it not?
He’s happy to stay.
“I’m beginning to hate this woman.”
Join the club – my partner’s two daughters and their husbands are Covidiots too. It’s usually people you knew to be not very intelligent who have fallen at the first hurdle, those who have questioned ‘Covid’ from the beginning seem to be more intelligent. There are many well-written and coherent posts on this site, for example. I don’t believe such intelligent people are all ‘mad’ and ‘conspiracy nutters’. Some take it too far (nanobots in the vaccines!) but many keep a level head and have sussed that ‘Covid’ is a con.
Well if it’s anything to go by this woman would be perceived by many to be extremely intelligent. A graduate from Oxford University no less.
I’m not really sure this is about intelligence though: more about an inherent wisdom.
I think there are 2 kinds of intelligence. The ability to learn and the ability to think clearly and see through the mist of irrelevant/false information. The more the world is bombarded with this information the fewer in number clear thinkers become.
The whole woke culture thrives on this mist. Which engulfs some very clever learners. They don’t have the clarity of thinking to see through it all.
Same here, a sibling with PhD from Cambridge who wears a mask even when not required, is jabbed, and is worried about OhMy.
I think that a lot of conventional success stories, professional and/or academic, have jumped through so many hoops, had to think a certain approved way etc, that literally cannot question this sort of thing. Very sad and shocking.
I also find it’s often the ‘highly educated’ who think they are too clever to accept there is a conspiracy occurring.
I’m predicting my SIL will insist on LFTs for Christmas Day.
My response will go down well I’m sure….
I’d tell her to get lost. If she’s that bothered, she should just cancel – as should every Covid paranoic.
These LFTs are all Made in China. Nothing quite like continuing to hand the Chinese all our money! Thanks for The Virus, China!
The importers of the LFT tests are those who need to be looked at.
China will probably only get 10% of the cost. The rest will disappear in markups by the interminable list of insider middlemen.
I think I have to agree with you – I think there is a class element to it. Worried, hand wringing middle class people who don’t want to be accused of “doing the wrong thing” or even worse, breaking the law, are taking the ‘testing’ approach.
I have written on this issue before. The relative hosting christmas this year for my family has issued an edict in the invitation that all attendees must do a LFT that morning and only attend if they test negative. I have no intention of doing a LFT as I think it is A) a scam B) likely inaccurate anyway C) absolutely DISGUSTING – it is small wonder there are so many people sick if they are constantly sticking those swabs around their tonsil area and then UP THEIR NOSES – ewwwww and D) I have a deviated septum so it would be positively dangerous for me to try to stick any kind of swab up my nostrils.
I’m not going into this with them – I’m simply going to lie and say i tested and it was negative. I take 4000iu of vitamin D every day, a gram of vitamin C and on days where there might be more risk to me [than I would likely pose to others] from being in close proximity to a lot of double and triple jabbed people I take quercetin. My daily diet is rich in good quality fruit and vegetables and is highly nutritious and well balanced – far superior to that of the seriously obese host who contracted a bad case of covid and then followed it up by getting jabbed.
Another relative’s christmas plans lie in tatters because of a positive LFT in another member of their party despite the fact that she travelled a long way to join the other guests.
I think the whole thing is utter madness.
In days of yore, colds and flu (remember them?) would be in circulation at this time of year. If you were highly symptomatic and unwell you didn’t attend a gathering. The idea that people’s christmas festivities should hinge on the outcome of a highly dubious LFT or PCR is just another ruse so that the testing contractors can make more profits and the little people can be further controlled.
I would imagine that working class people who have possibly invested a lot of time and money which they have had to save up and set aside to fund their celebrations wouldn’t let their plans be derailed in this way. They would likely assess the ‘risk’ and go ahead.
The wine and cheese parties in No 10, both last year, and in May 2020 did not, I imagine, hinge on the outcome of a LFT or PCR test. And that was when the covid ‘pandemic’ was supposedly at its height, unlike now with the Omicron variant which is so mild people do not even know they have it. I rest my case.
We’ve allowed a generation or two to grow up thinking the world revolves around them.
Until people asking for unreasonable things like this start to lose out on income and life nothing will change.
It’s time the Nervous Ninnies were sent to their room and excluded until they find some strength in their spine.
Yup.
Why wait? It’s all political theatre, has been from the start.
Hubby needs to grow a pair and tell his sister where to get off. She has the effing nerve to tell HIM how to run his life. His bloody sister. Not you his wife.
Grief.
Seems perfectly reasonable to me
There’s always one. Lol.
I’d love to believe you’re right Toby, but, this site being for sceptics ‘n all, I’m a tad – well – sceptical! The following comment was posted btl by Jon Garvey on another article a few days ago, and it’s one we would be wise to keep in mind when deliberating how this might all play out over the coming weeks . . .
“As Sarah Knapton pointed out in the Telegraph today, the death figures are bound to rocket, if Omicron harmlessly infects millions, because of the way that Covid deaths are defined (within 28 days of positive test), and the normal death rates at this time of year – she quotes 0.9% usual death rate for January.
If a sizeable proportion of the population gets Omicron, many thousands of deaths will get falsely assigned to the Covid deaths by definition. You could have zero Omicron deaths (not too unlikely) and still have the worst pandemic winter on record.
The only saving grace would be that excess deaths wouldn’t be that high, and the non-Covid deaths would plummet. But you can bet your life Whitty and Co would forget what they knew about excess deaths and pandemics in 2019.”
I fear this is a more likely scenario and Prof. Lockdown and his fellow doomsters at SAGE will finally have a prediction that comes good.
Agreed that will be a difference compared to say South Africa which is having it in summer.
They would count as ‘with’ not ‘from’, which the UK regime has already acknowledged in their desperate attempt to find an omicron fatality – grudgingly noted as ‘with’, not ‘from’. Vaccine status inferred to be fully dosed up on the grounds that an unvaxxed status would have been just what the covidians want and would have been shouted from the rooftops with no concern for patient privacy. ‘Patient privacy’ these days, like ‘national security’, is the first refuge of the scoundrel.
Italy had a similar proportion of ‘from’/’with’ as the UK and has officially, but quietly, downgraded its covid fatality count to about 10% of the earlier figure. Too late of course.
Any excess deaths will more likely be the result of ADE but attributed to Covid and whatever the current flavour is.
This comment sat on the Telegraph website for the best part of yesterday and crept up the list of ‘most liked’ until it was taken down for violating their rules. I was expecting it to last no more than five minutes – hence the screenshot. Hold the line guys. Truth shall prevail and we shall be victorious. Happy Christmas one and all.
What I want to know is why was it taken down?!
“It never happened, and even while it was happening, it never happened.” Harold Pinter on propaganda during during his Nobel Literature prize acceptance speech.
Amen to that
I have heard it is already done and dusted
I have felt this for the last few weeks too, just being out and about, seeing more non compliance with mask wearing, old folks not caring a hoot in supermarkets as they squeeze by you to grab the last punnet of blueberries, it just feels like people are no longer terrified. There are still those of course who have it well lodged in their nature and psyche, the snide Benjamin Butterworth types who just enjoy telling folk how to behave, the virtue signalling Esther Ranzten types who just know better and the angry fat shouty middle aged man types like James Whale and that John Gaunt fella, who has lost his mind, and is sadly just terrified. When I see these folk on TV now they are starting to sound like delusional extremists, they really are not sensing the mood of the nation. One of my most zealot lockdown loving, rule following, triple jabbed, kid jabbed friends told me the other day that even she was running out of steam and couldn’t face another lockdown. We are reaching the end of this road.
yes and no – I’ve seen the same in supermarkets (trains too), but went for a wander round the town centre yesterday evening and it was absolutely dead – some of the pubs and restaurants hadn’t even bothered to open, and those which had only had a handful of customers. No way normal for a few days before christmas.
Very true, it is not at all like Christmases past, but to see as many folk in Glasgow town centre not wearing masks is really something, compliance has always been near 100%. Plus I just have this feeling in my bones, 2022 could be our year
Tesco at 5am this morning and i didn’t see any other non-mask wearers. Which i’m afraid has been typical round here, even though no one, member of staff or public, has ever challenged me. Maybe because i tend to go very early in the morning, the shoppers are the terrified because they think they will be ‘safer’ then as there will be fewer people around.
But masks may now just be an easy sign of conformity for people and they are becoming more willing to ignore other restrictions quietly and behind the scenes.
M&S, and probably Waitrose, are ground zero for the mindless zombies and wannabe fascists who would sell out their neighbour / relative to the Brownshirt Covid Police.
The people on the front line actually working/delivering goods etc know it is BS (M&S staff wear masks only ‘cos some fscking masked Karens complained). The top level know it is BS because they are running the show. It is mostly only the pampered pandered mediocrities who fall for the BS. The ‘not wanting to rock the boat’ / ‘be different’ aspects also play a big part, thoroughly exploited by the Nudge Unit (aka SPI-B).
Check out the #Waitrose hashtag on Twatter. Especially “blue tick” Simon Day (him from off of The Fast Show). Ironically, his bio is “Do not live in fear” https://twitter.com/simonday
The figures for deaths in care homes show a sudden sharp rise in England in week 17 of 2020 (week ending 26 April). Then deaths fell and rose again in the winter of 2020/2021.
From The Exposé:
Beds occupancy in NHS hospitals for the periods of April to June in 2017 to 2020 inclusive:
In the April to June period in 2020, at the height of the SARS‑CoV‑2 “pandemic”, bed occupancy in NHS hospitals was down 30% when compared to the same period the previous year. NHS bed occupancy was also down about the same percentages when compared to the same periods in 2017 and 2018.
Visits to NHS A&Es for the periods of April in 2018 to 2020 inclusive:
Attendance at A&E in April 2020 was down a whopping 57% compared to the same period the previous year.
But yet figures show that deaths of old people in UK care homes took a sharp rise at the very same time that the NHS bed-occupancy work-load decreased by 30%, and the A&E workload decreased by a whopping 57%.
An alarming footnote to this is that a directive was sent out on the 19th March, 2020 to the NHS which required them to discharge all patients who they deemed to not require a hospital bed.
(The link will bring you to a page that informs the document has been removed because it was out of date. I’ve included a screen-grab of the original document below, thanks to The Exposé. But how on earth can any authority issue a directive and then after the event claim it is out of date?)
Follow this link to hear Matt Hancock confirm on video that the government had a “big project” in place to source drugs like Midazolam. Also, note the psychopathic countenance of Dr Evens in the video – if ever an actor is needed to play Josef Mengele, Evens would fit the bill fine.
Directive to vacate hospital beds. Hospitals and A&Es at least busiest for years. Large numbers die in care homes at the time hospitals are less busy than they ever were. Matt Hancock confirms to a psychopathic looking Dr Evens that large quantities of horse-strength sedatives are on the way.
I really don’t think there is any option but to go with Occam’s razor on this one.
However, to keep perspective,it is worth bearing in mind that there has always been a problem with discharging fit patients from hospital beds, and the use of A&E for non-serious complaints.
That said, the proposed framework for discharge is unrealistic IME.
Over the past couple of days I’ve seen a number of Covidians using this to try to justify their locktivism:
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1043095/COVID-19_Data_Briefing__21_December_2021_.pdf
Particularly the graph on page 13. Has anyone analysed the data behind it to see what this actually shows in reality – i.e. which of the many definitions of ‘unvaccinated’ is in use, what proportion of those are already so ill with something unrelated that they can’t be ‘vaccinated’, etc…
‘Vaccinated’ is a political status, not a medical one, though those exploiting it pretent it is purely medical.
pandemic, case, infected, cause of death, vaccine, vaccinated – all words that now mean whatever the Queen of Hearts wants them to mean, varying as needed to suit the desired outcome.
Agree – but try telling that to a BBC news swallowing total covidian. They believe that those words actually still mean something now.
The idea that a ‘case’ might be no more than a fraudulent positive test result is just totally beyond their comprehension.
Very frustrating.
100% agree with Toby here and but Johnson may hedge and throw in a token gesture like shutting sports stadiums, rather than fully reject the doomsters. That may keep the Tory mp’s quiet. Anything can happen the PM is an imbecile.
The chain has been broken by prior immunity the fact that Faucism rejects. Our Health secretary Mr Malteser Head is a disciple of Fauci. That could be the biggest problem of 2022 and the MAIN reason people won’t get injected is they have already had the virus and in that case the experts you can trust expect immunity to last a long time from CCP Virus.
“Or Boris could just look at the actual data.” – the only figures he’s interested in are those on his Cayman Islands and Swiss bank accounts.
Anyone care to predict how 2022 is going to go? I think it’s going to be much of the same, only by next Christmas the adults and fossils will be on their 5th jab, and the 12-18 year olds will be on their 3rd jab. The 0-11 year olds will also get jabbed during 2022.
By December 2022 people will still be wearing face masks in shops and on public transport, and people will still be testing themselves often to see if they’ve got lucky with ‘The Virus’. There will be a new ‘variant of concern’ wheeled out this Spring, and maybe another ‘mutant strain’ to add more mayhem during or after Summer.
Protests may still be allowed as it allows people to let off steam – the Police know protesters turn up around 1230pm and go home four hours later, and they have everyone on file anyway. Internet discussion forums will be even more tightly controlled and people will have to be very careful about what they post for fear of ‘the authorities’ come knocking on their door.
Let’s see if I’m wrong. All a bit grim, but look around you. I remain hopeful that things will get better, but at the same time I have to look at the reality.
How much tat have we bought Made in China for Christmas? …is that a sort of “Thanks for releasing SARS-CoV2 onto us!”
Unless there is quiet push back.
Which there won’t be as the vast majority of people have swallowed the propaganda.
I’ve said before that the Government and SAGE can have even more of a laugh once they’ve got so many people hooked on these ‘vaccines’ in order to keep their ‘vaxx passes’ valid. All they have to do is invent a ‘technical problem’ and ‘shortage’ of vaccines… say, the 5th Jab… and watch the people scramble to get one!
Fisticuffs outside the NHS Jab Centre! The surveillance cameras can feed directly to the televisions at Downing Street and SAGE headquarters. It will be like the Romans watching gladiators, only a bit more like this:
https://www.youtube.com/watch?v=4g2Rt-1hfbA
All of this presupposes that Johnson and his chums are sensible. But they’re not. They’re fanatics.
I think some of them are becoming more sensible according to reports of Cabinet discussions. Others are fanatics. As for Johnson, i think he is just ‘a reed shaken by the wind’.
AEP nails it
https://www.telegraph.co.uk/business/2021/12/23/prof-lockdowns-apocalyptic-omicron-claims-undermine-faith-vaccines/
“Academic etiquette restrains direct criticism, but immunologists say privately that Professor Neil Ferguson and his team breached a cardinal rule by inferring rates of hospitalisation, severe disease, and death from waning antibodies, and by extrapolating from infections that break through the first line of vaccine defence.
The rest are entitled to question whether they can legitimately do this. And we may certainly question whether they should be putting out terrifying claims of up to 5,000 deaths a day based on antibody counts.
“It is bad science and I think they’re being irresponsible. They have a duty to reflect the true risks but this is just headline grabbing,” said Dr Clive Dix, former chairman of the UK Vaccine Task Force.”
“Dr Clive Dix, former chairman of the UK Vaccine Task Force.”
Former chairman? Easy to say these things when you’re not working there anymore!
The ‘Good German’ defence.
At least he opened his gob and had a go.
I know it’s not directly related to the article but what is the basis of the claim that 9/10 in hospital with Covid are unvaccinated?
Also headline in the mirror claiming it’s young people dying in hospital who are unjabbed. Really??
More importantly, why do the jabbed care if unjabbed die? Why don’t they have the same zeal for “saving” the obese or heavy drinkers or drug users from themselves and from taking up valuable NHS resources?
Why do the jabbed mask wearers care if I’m wearing a mask? If they at triple jabbed and have a mask on (should be ffp3 if they are really scared but is usually what amounts to a soiled pair of pants) then they are protected.
The other good one is obese smokers dutifully replacing their mask after inhaling tar!
A particularly stupid step relative of mine is in favour of concentration camps for the unvaccinated, smokes and has been hospitalised several times with asthma induced pneumonia….
A cousin of mine, a keen motorcyclist, follows the Piers Morgan and apparently mainstream dogma that the unvaccinated should be refused hospital treatment. I told him while sitting beside him at dinner that he and people like him should be hanged from the nearest tree.
And then hopefully also told him he would not deserve hospital treatment, as he had, most definitely, brought it upon himself
A very polite and considered response.
Read Will Jones’s article on this yesterday (Dec 22) it’s titled No, the NHS is not being overwhelmed by the unvaxxed, and he goes into this 9 out of 10 claim in some detail. I haven’t seen anything about unvaxxed kids dying. Maybe they have other major health issues and that’s why they havent had the vaxx?
It all depends on the meaning of ‘unvaccinated’ Today’s vaccinated are tomorrow’s unvaccinated.
Ah, but the thing is, the ‘data’ coming from S Africa is ‘real-world’, and inferior to actual Data derived from the Computer.
In the same way, natural ‘immunity’ is a quaint, but out-moded belief, that some still harken to. The abundantly clear reality, however, is that true immunity can only come by way of Synthetic immunity.
They are also a younger population so we have to be very scared still. Come on keep up
That’s right.
Science is useless, unless it is genuine THE SCIENCE lovingly purchased (with your money) by HMG.
Policy based Evidence making at its finest.
The Anti brexit EU gravy train riders have been strangely silent, for quite a while now, are they on the Jaboree gravy train now, where tax payers money is being redirected from services, including the NHS, to be used to buy jabs, ppe, testers etc, to solve the nhs problem one way or the other.
Covid mania is imposed by Brexiteers.
Just a fact to counteract imaginary assumptions.
Sigh. There you go again Rick. What silly, silly nonsense.
I suspect that your feelings about the covid havoc pales to insignificance compared to your apparent absolute contempt for the crime (as you probably see it) of Brexit.
Your ‘fact’, that: “Covid mania is imposed by Brexiteers.”, is just deranged obsessivenes.
Shame we left the EU – if we had stayed, we clearly would not have to suffer covid mania. As a Leave voter, please accept my sincere apologies for playing any part in the resultant Brexit-induced covid mania.
Still, one more thing to blame on Brexit I suppose.
FF’S!
This article is predicated on the belief that all actions so far have been motivated by a concern for the nation’s health. Unfortunately, the last last 20 months haven’t been about health.
The economy has to be flattened – expect another lockdown.
Look at us in South Africa. We have had zero changes to our so called lockdown measures which as it stands consists of a midnight to 4am curfew and masks in shops (believe me when I say 80% of the population ignore those rules anyway). The case numbers went up very fast and they are coming down very fast. We probably have about 30% vaccination rates who mainly consist of the same middle class who have been the only ones obeying these restrictions for the last 20 months. The majority of the population have no interest in vaccines or any of the rules imposed on them. Our medical advisory council seems to have finally agreed that the whole testing, tracing and quarantining of people is a waste of resources and must be stopped. I went to a big schools provincial tournament last weekend and the rules and regulations that they were trying to follow lasted about 24 hours by the time the finals arrived the venue was packed to the rafters with most people having given up on all the masks and other rituals of the terrified class. I sense it is over here you guys just need to realize that for yourselves.
All this confirmed by my friends and family there. I should’ve joined them.
You should its still an amazing place to visit especially the Cape.
I agree – beautiful. Spent quite some time in Cape Town when I had family living there for a few years. I’d happily move if you guys could keep up what you are describing [covid over] and I could live there. Staying in UK isn’t very palatable the way things are going.
confirms my post above Jock – it is a middle class conformity/anxiety thing.
Just had to post this…says it all.
The funnier version has “Free Coffin”.
That’s not the funnier version, that’s the true version.
And there is nothing funny about it. It means that all the people I love will be gone.
Do you know what alw, sadly this isn’t far wrong – based on the latest UKHSA study published in the MSM today, where booster effectiveness ‘wanes’ after 10 weeks and they announce that they intend to maintain “flexibility” over the booster programme, that means a booster 3 times per year minimum (until the PHE is declared ‘over’, scheduled for 2025 based on current info). Wonder if people who decide they don’t want to be ‘boosted’ that many times, for a cold, should look into ivermectin.
The positive rate for test results is not going up so how can Omicron be spreading at all? The increased cases are just becausevof increased testing aren’t they?
Always have been. Testing asymptomatic people with an imperfect test is guaranteed to produce a pseudo-epidemic. This is a well kmown phenomenon.
I see a massive epidemic of asymptomatic broken arms. I just happen to have a test for this condition. It isn’t perfect, but is good enough. A 4lb lump hammer. The amazing thing is how often people develop symptoms after being tested. I’m sure that is evidence of the value of the test, catching people just before they become symptomatic. I am sure with the right marketing, this could save the NHS millions.
“debunk irrational nonsense in the media with your incisive comments below the line”
Thank you for the encouragement – but it probably isn’t needed!
Thank you to all contributors both above and below the line for providing a beacon of light over the course of this diabolical period.
The current battle may be turning in our favour but there is still an awful long way to go before we can say we are winning the war.
This is probably not the beginning of the end so much as the beginning of the middle.
At least China was right, at the start they said this would lead to people falling down dead in the streets, on the sports fields and on live TV.
Should have never doubted them…
People falling down dead in the street, with a film crew in place at exactly the right moment. Colour me sceptical.
Western MSM presentation
The bigger picture
Tank man was stopping the tanks leaving theTiananmen Square, not entering it.
Merry Christmas everyone.
And I don’t care what Johnson and his cronies say, I will be meeting friends and family throughout the festive period and indeed I may even party like it’s 1999!
good for you – have a good one!!!
call me cynical, and frankly I think I am now the biggest cynic on the planet, I think we are all being treated to a bit of a Christmas pantomime. If we look at Johnson’s political situation he is on the skids, with a possible leadership challenge in the New year. He needs something to save him. So, why not send out all the little demons (sorry advisors)to spread fear and doom and gloom regarding anothe Lockdown in January, Will he do it? Oh yes he will, oh no he won’t etc. Then in January he will show strong and decisive leadership against Satans little minions and say NO, we will not heed you, we will carry on, Omnicron is not the plague. The back benchers will jump for joy, they will claim that Boris has been brought back to life, the media will love him once more. Primeminister Johnson will remain and the confected Omnicron will be put back in the cupboard for a feww weeks until Mr Johnson needs to bring out a new scariant round about February.
I agree. We are being played.
We have been played since Day 1.
As I said to my equally sceptical son this morning, next year there will be a new film released, “Boris saves Christmas”
Boris saves Christmas – only a year too late!
Still, better late than never…
Without sounding flippant, ” the end of the world is nigh ” could become a reality if… Russia, China or Iran made a bad mistake of lobbing nuclear weapons around Even a conventional war in Ukraine, Taiwan or Iran/Iseral would cause millions of young lives.
Russia has no need to invade or ‘lob nukes’ into Ukraine. The Ukranian military was once part of the now-defunct Warsaw Pact. Russia knows where all the weapons stores are (it still has serial numbers of anti-aircraft missiles supplied prior to the end of the USSR), what the stores contain (weapons sold to ISIS aside), where the fuel stores are, the routes of the secure comms lines, the secure bunkers, the airfields, the logistics centres, locations of the US outsourced bioweapons research labs (all 16 of them), etc, etc. It fired Kalibr cruise missiles 1200km from the Caspian to ISIS targets in Syria with ~100% target strike rate. The most distant part of Ukraine is ~900 km from Crimea. Ukraine can be trashed militarily without Russian ground forces having to leave their bases 100’s of km from the border. The shreyed invasion is a Ukranian/NATO wet dream.
Yes listen to the data please Boris, but also…don’t! Because what are we saying if we advocate that the degree of restrictions we accept should be proportional to the severity of the variant? We are tied into this nightmare forever!
There should be no restrictions placed on our lives in order to help the NHS. The only incentive to staying healthy should be good health. I don’t even care about the so-called “spread”. If people are scared then they can stay home or wear PPE.
As for Boris, it makes no difference if he “holds his nerve”. Respiratory infections will peak in the UK in the 3rd week of Jan, the same as they do every year, and he is on his way out whether it’s for imposing new restrictions too late or never.
I hope that someone behind the scenes is already planning which of the Covid Recovery Group members has the best shot at a leadership challenge. Is it too late for me to join the party so I can vote?
I’m still waiting for the photographic expose of the sage Christmas parties that most likely happened last year.
There must be tons of examples of Ferguson, Vallance, Michie, et al, breaking their own rules.
Constantly showing Pfeffel breaking their rules concerns me that it is an effort to replace him with someone who’s more strict. That’s certainly the direction the corrupt MSM have been going.
I rather hope the government, SAGE and the rest of them go on a two week bender, if they are all pissed or hung over at least they are out of the way and less likely to make decisions that might harm us. The photos can be used at a later date.
5000 deaths a day? So half a million over 3 months? The man’s insane, or he’s been sniffing something, any tool can see that “the virus” is relatively benign, unlike the actions of our government.
Quite frankly, the best use for SAGE is to mix them with onion and shove it all up the arse end of the nearest large turkey. At least we wouldn’t be able hear the incessant whining.
I guess I am very slightly optimistic. We might take some comfort from the fact that ministers are now demanding hard data. Also, apart from mad Nad and Javid, who has fallen under the fatal mesmeric control of the NHS, the cabinet are more sceptical.
At the moment, however, I think our gratitude should go to thise Conservative backbenchers who voted against plan B. Johnson is wary of being a Tory leader with a big majority who needs continually the support of Starmer’s pusilanimous Labour MP’s to get something through the house.
Further, the mood of the country is changing. Many in my experience who previously went about with a ‘keep safe’ in their heart and a mask on their lips now openly questioning why, when the country is jabbed up to the eyeballs this shitshow is still going on. Why Whitty, Ferguson and their ilk still keep appearing through the floor like the Demon King in a Pantomime with graphs of insensible woe.
We can but hope that scales are falling from eyes.
I was in a large and absolutely packed city centre German-themed bar/restaurant yesterday. I was sitting next to a large window looking onto a main pedestrian thoroughfare to the Christmas markets. It was really interesting to see how many muzzled morons were coming up to the window to observe that life was completely back to normal inside. What must have been going through their addled minds to see a bustling warm environment full of cheery people living their lives. The expressions on their faces weren’t disapproving, they just looked completely confused. On either side of their route they would have seen a heaving Christmas market (despite the wet weather), and a full Christmas ice rink. Seeing something like that when the telly has been telling you there is a deadly plague has got to eventually get through the layers of brainwashing.
As for scales falling from eyes – yesterday we met up with brother in law and wife in a pub for lunch – we haven’t seen them since this nonsense started. We noticed as we drove through their Leicestershire village people were masked walking in the street!! We walked into the pub unmasked as were the staff but everyone who came in were wearing masks until they sat down, including brother in law and wife. He took off his mask and put it on the table I said ‘they don’t stop you catching a virus you know’ – he never replied – so whilst some may see the light others will never do.
“He took off his mask and put it on the table “. That about says it all. You take off a rag soaked in bacteria from mouth and nose and put it on the surface you are about to have plates of food and cutlery placed on. Food hygiene 101 – not. How many people are getting ill from precisely this sort of stupid behaviour. Who needs the “killer” covid to fill the hospitals..
I would love to believe that might be a possibility for the tide to start turning. However just like before each previous lockdown was a political decision to cover up the social economical disasters of Brexit and corruption in the government isn’t it?! Every single one of them … so at the moment Boris government credibility with all “leaked” media stuff is not looking that great is it?! So perhaps once more lockdown will be used to crank up fear once again and deviate once again the public from what is really going on. But coming January 2022 and the collapse of financial market… the pocket of many will be truly felt…. Then Covid or not people will feel across the world …. Where things really hurts… the pocket with no money!
The next step ‘may’ help prove that this is about the virus or something far more sinister. Interesting time.
I recommend Robert Kennedy’s latest book on Fauci – lots of useful information in it and one which made me sit up more than others was Fauci took his lead from Ferguson’s computer modelling! And there you have it!!
Fergusoon et al,. have always played a leading role in all this. The largest contingents to WHO meetings have always been from the UK.
A lockdown sceptical tune (with a US focus). Hold the line fellow amazing lockdown sceptics.
https://www.youtube.com/watch?v=R7KFjB51p7o
The reality is, right now ;- regardless as to whether i actually want to or not, but i am barred from flying, visiting a theater, going to a large football match, going to a nightclub or working within “our” nhs .
I expect it might be difficult for me to even sit in a cafe next year at some stage.
I have written assurances from my own MP (who actually voted with BJ last week) who has insisted he wanted no more restrictions and he hates the idea of further lockdown- he voted in favour of medical apartheid has meant he and his party has lost my vote forever,
For now, for UK use, order some LFTs, then when you need to go to a fascist-run event you just go to gov.uk and register the serial number of one of the tests. No photo required so just chuck it unused in the bin ready for
landfillrecycling. They send you a text so you can even show it on your Nokia 3310. Obviously if there are non-fascist venues then favour those, but when you must, this is an easy open goal.I personally will not ever do or pretend to do a test or show a medical pass, unless in very extreme circumstances to protect me or my family’s physical or mental health.
Look, you have a choice. Suffer the oppression or defraud the system. As I said, prefer places where you don’t need to do this bullshit, but if it is a choice between you having to suffer at home or to cheat and go and live a meaningful life then cheat. Doesn’t mean you can’t fight in other ways.
Either way I suffer. But I can live a meaningful life without cheating. But I am not judging others as we are all different.
Agree with you on this. I’ve never taken any Covidbollocks test. Cheating with them is playing their game, so should be avoided – refusal to co-operate is the way to go.
The clue is in the first two words of your justification… “for now”. Do you mean like many did for three weeks only? The only morally acceptable position is non-compliance. This will never end otherwise.
It is non-compliance. Cheating is non-compliance. Locking yourself at home and avoiding entertainment is compliance.
Do not do any tests, do not participate
I’m not doing tests. In fact I am binning tests without them being used.
Ive only done a test once and it was in order to cross a border.
I think a sensible rule is to do the least we can possibly get away with, in our own circumstances. So it’ll vary a bit. Piers Corbyn can probably get away with cooperating less.
If I recall, Dolores Cahill said a year or so ago that she knew how to take a flight abroad without cooperating with ‘the regime’.
I thought it was the big football stadia you can’t get into without a vaxport. Find a smaller local club to support! I believe some have removed seats from their stands to get below the 10,000 number. Sensible.
I can’t believe you still think Boris exercises his own will and judgement in making these decisions.
Good to see Toby putting exponential growth in quotes as if it did do that it would break the laws of Maths https://www.linkedin.com/pulse/why-epidemics-never-grow-exponentially-zeb-mason/
The term ‘exponential growth’ is meaningless without mention of the exponent. Doubling every day and doubling every millenia are both examples of exponential growth. For ‘cases’ doubling every day, the number of ‘cases’ exceeds the UK’s population with 26 days and the planet’s population within 33 days – a clearly impossible and meaningless situation.
For anyone who hasn’t seen this. Tedros made a Freudian slip and admitted that
“Some Countries Are Using Boosters to Kill Children”
No, this is a myth. He clearly started to say “kids” and changed it midway to children.
Our cause doesn’t need lies and dubious insinuations like this, all it does is discredit us. Live by truth.
That’s what Snopes says. You can judge for yourself the reliability of that group. But the fact is that this is clearly what Tedros says. I’m very familiar with his speech pattern and his accent (similar to other East African accents) and thre is no ‘stumbling” here. Of course, he didn’t mean to say it. It is what is called a Freudian slip, similar to Sir John Bell’s statement to John Snow (last year) that the vaccines wouldn’t “completely sterilise the population”.
There is also another lie. He compares the deaths of SARS-CoV-2 – essentially a one-ff 1 to 2 year event with anuual deaths of malaria, HIV, etc. These other diseases are on going, year in, year out.
Compare the total SAR-CoV-2 deaths with the total malaria. HIV, etc deaths and the picture is totally different.
He also claims (with/from unspecified) 50,000 deaths in the world every week. There are about 10,000 deaths every week in the UK, so there will be about 1,000,000 deaths every week in the world (based of pro-rate projection). SARS-CoV-2 isn’t even in the top 10 cause of death (at a guess).
Good point. But without a purified isolate of SARS-CoV-2, as well as controlled studies looking at its pathogenicity, i’m not sure sure how anyone can attribute any deaths at all to it
There is only one thing that will beat this nonsense, SaRcAsM
the twitter accounts of “Wayne the Covid Marshall” and “Hatt Mancock MP” make me laugh anyway
Think sounds like a cry for help Toby – is the truth setting in?
Fraser Nelson of The Spectator asked Graham Medley (of the London School of Hygiene & Tropical Medicine) why he didn’t include the scenario of Omicron being less virulent in his modelling – Nelson was referring to modelling which Medley had presented government, and on which further lockdowns, mask wearing and other life and economy destroying dictates are to be based.
Graham Medley’s verbatim response:
So, there you have it. Graham Medley has admitted that government officials basically tell him and his team at the London School of Hygiene & Tropical Medicine what they want the Omicron modelling to predict.
And I assume Medley and his team obeyed orders, and designed the algorithm to predict what the officials asked for it to predict.
So, I think I’ll back the horse that’s called “Lockdown in January”. And then I’ll put the winnings on the nag that’s named “Mandatory Vaccines in April”.
And if these two horses come in, I’ll spend the winnings trying to get asylum in Hungary.
Same as polls
Interesting reading the Twitter exchange that a policy of ‘Do Nothing’ does not appear to exist.
From those in the know lockdown will be on the 28th. Looks like James is going to be £50 better off.
For once I am dubious – because of Frost and the 100 (not even half as many as the famed 300, but certain to grow if pushed)! I don’t think Bozo can dare to do it again.
My money is on about 2nd or 3rd Jan. I was talking to a friend who’s fairly senior in a charitable NGO and at least 3 weeks ago they were asked to assist with mass testing from 4th Jan. As he said “there is concern that children won’t of been tested over the holidays and require testing before they return to school”. Nothing like attacking chlidren for their nefarious ends.
And this is exactly why Johnson will not be permitted to let omigod run its course. More internment must be imposed so that it can be claimed to have saved us.
And it needs to happen fast. Mechanical ventilation bed demand in England has been falling since a peak in early November, and is down again this week. Eventually the good news will slip out despite all that MiniProp can do to suppress it.
Bozo is not interested in the data or the nations health, just his image.
I spent Tuesday/Wednesday in a hospital holding pen while they decided where to put you. 8 beds, most occupied for less than a day so perhaps throughput of 15-20.
Every single one a Gammon, some younger than other, some more in sound mind than others.
Not a single one bothered to access the free individual tellys available; probably glad of a rest from it.
On Tuesday 6pm, as I ventured toward the loo by the Nursins station, their TV was broadcasting his
“I’m not cancelling Xmas”
This was greeted with a prolonged round of applause from the combined Staff which was precisely the desired result.
To be fair, if you had nearly completed 7 × 12 hour shifts the last thing you would want to hear would be your 2 day family Xmas ruined again.
That man is nor always stupid.
https://www.youtube.com/watch?v=ynesjwEOAqQ
I’ve listened to the arguments. And pored over the data. The carefully considered question that I would like to ask Boris and his SAGE advisors is ‘would you ever away and take a flying fuck at yourselves’
if you look at the all cause mortality around the world its hard not to come away with the feeling its the lockdowns doing he killing and covid is just ‘present at time of death of old age’
Peru had the hardest lockdown in the world and doubled its annual deaths
https://ourworldindata.org/grapher/cumulative-excess-mortality-p-scores-projected-baseline?tab=chart&country=PER~SWE
I have been sick of being told to save our Notional Health Service for 22 months. They must love being pinged ads they have nothing to do in empty hospitals.
We need the lefty public sector to be reined in. If Doris doesn’t know by now that they will never vote Tory, he never will.
I got a surprising amount of support for this comment in the Guardian yesterday.
I think the Health lobby have gone too far with COVID and will pay a heavy price. Appetite for reform of the NHS is going to grow. People don’t take kindly to have GP appointments or cancer checkups denied to them.
They could do all of that as long as long as it wouldn’t make the shares plummet because IMO, at the top of this pile of * its all about the money
The Central Banksters can’t keep printing money forever. Their usual m/o is to trigger a war, timing known to them so then can cover themslves to take advantage. Russia’s ultimatum to NATO has pre-empted that so the central banksters are now facing the consequences outside of their control. More and more Asian countries are side stepping the USD for international trade (currency swaps being preferred) so soon the USD really will be toilet paper. China is disposing of part of its nmassive holding by running massive infrastructure building projects, converting paper to assets. The western USD dependent economies are heading in a very unpleasant direction.
Off topic, but has anybody else noted in the free online Daily Telegraph they use to have a bar graph showing the numbers of “boosters” given against the target number. The last time I saw it, they were lagging about 30% behind target. Now it no longer appears, strange that.
It reminds me of how the UK government stopped reporting ‘recovered’ statistics shortly after the start of the lockdown in early 2020. Apparently, the message was you caught covid and died … at sometime in the future. … but only in the UK.
If we put to one side the possibility that quite a few senior politicians have been bought by Big Pharma and the vaccine lobby and just assume for one moment that Toby is right and the last 21 months has been all about cock-up, then one huge factor in contributing to the cock-up has been the absolute dearth of politicians from a numerate, scientific or engineering background who are sufficiently grounded in reality to question the so-called experts like SAGE.
We BADLY need to chuck out a large proportion of the PPE graduates who populate the benches of the House of Commons and elect a new cohort who can count, understand statistics and are capable of spotting bullshit.
Good luck with that, Common Purpose type graduates have been rolled out for at least 30 years
Cock-up? Only in a Ferguson/Handcock sense. This situation has been planned for over many years, overtly with the change of definition of pandemic to exclude a requirement for deaths, and also the explicit legal immunity granted to Big Pharma following to 2009 “flu vaccine gives kids permanent brain damage” PR issue. Zika was an early example of a disease affecting poor countries that TPTB hoped would spread to the west allowing Big Pharma to go ‘kerching’. It fizzled out fortunately.
Or Boris could look at the actual data, as several members of his Cabinet have been urging him to do.
I am not sure there is much benefit from Boris looking at data. Data and facts are not his thing. But others might do so on his behalf. They should do it intelligently, not just leap on press stories that support their position.
Currently most regions in the UK are a mix of Delta and Omicron, but London is reputably close to 80% Omicron – so it is worth looking at its data separately, as well as the national picture, to see what might lie ahead.
Now let’s look at each of Toby’s claims in this paragraph.
The data suggesting that, far from doubling every couple of days, the number of daily infections is plateauing.
That was based on a couple of days data and already looks overoptimistic based on yesterday’s record number of cases. If you take a 7 day moving average, which is the statistically sensible approach, I am afraid there is no sign of a plateau. If you look at London they are doubling every four or five days.
The data suggesting that, for whatever reason, the link between Covid infections and hospitalisations has been broken, with Covid hospital admissions remaining largely flat over the past two weeks in spite of the uptick in daily infections.
Of course the link was largely broken in the summer when vaccination programme was widespread. However, it is not totally broken so enough cases will produce more admissions. At the moment the rise in cases is largely in younger age groups so we don’t see much hospitalisation. However, in London this is changing. The rise is beginning in older age groups and hospitalisations have started to rise.
The data on the length of time Omicron patients stay in hospital, with one South African study showing the average hospital stay had been reduced from 8.5 days to 2.8 days.
Any other studies on this? The South African population is much younger than the UK population and they routinely test every hospital admission for Covid. So people coming in for quite minor procedures may be recorded as Covid cases.
The data – endlessly reproduced on this site – showing that non-pharmaceutical interventions do little or nothing to suppress Covid infections, with every wave following exactly the same trajectory, regardless of the severity of the restrictions, or whether any containment measures are imposed at all.
This is highly debatable! Covid waves only follow same trajectory in the sense that they go up and eventually come down. They vary immensely in the height of the peak, the duration, and the shape of the curve. Just look at the UK waves – picture attached. Look at this failed attempt by a Daily Sceptic writer to predict the waves in various countries. If you look at what happened afterwards it bears no resemblance to his prediction.
The most pessimistic scenarios from LSTM and Imperial will probably turn out to be false. They aren’t intended to be predictions anyway – just illustrations of what might happen given certain assumptions. That doesn’t mean we should swing wildly the other way and base policy on selected press stories that happen to support our preconceived position which will also probably turn out to be false. The fact is we really have little idea of what will happen next, but unfortunately decisions have to be made in the face of uncertainty.
Yawn. Certainty – covid was and is not an exceptional threat to society and NPIs do nothing to affect it anyway. If you’re worried about covid, get quadruple vaxxed, wear three masks, hide at home, and let human beings with a properly functioning brain get on with their lives as they always have done.
The key statistic is how many patients with COVID are there in hospital, since that is where the demand on the NHS can be measured, and the answer is around 7400, or an average of about 5 per UK hospital – the level it has been at since July.
If “is COVID overwhelming the NHS?” is the measure by which we should, or should not, introduce any further measures, the data is clear that we should not.
Yes. But the key question is how many can we expect to be in hospital over the next couple of months. As I indicated, the number in London is already beginning to rise. “On 22 December 2021 there were 2,036 COVID-19 patients in London hospitals. This compares with 1,372 patients on 15 December 2021″
Now compare this with previous years – can you find any where the number aren’t rising during December?
I don’t see your point. There has only been one previous year of Covid. Cases went up last December and peaked in January. So what?
I’m not talking Covid – I mean hospitalisation rates generally. Trying to isolate “covid” cases is meaningless due to the persistent lack of clarity between ‘with’ and ‘of’.
The perennial NHS winter bed occupancy issue – courtesy the Grauniad for that extra wholesome truthiness.
You persist with various fantasies – one being that things the government does in relation to covid have any influence on people getting covid or going to hospital, and one other being that the figures for “covid-19 patients” are meaningful and related to people suffering primarily from covid for which hospital care is required, as opposed to people who are in hospital for other reasons who happen to test positive. You are an apologist for lies and fascism.
You can never escape, from The Ministry of Fear!!
https://youtu.be/wXHHkvPPN9I
Is that so? And the absolute certainty of other outcomes outweighs the uncertainty does it? Here’s a little sum for you. The govt have spent £400bn so far on covid measures. That’s twice the annual nhs budget. Now if prof lockdown was right on report 9 and he’s “saved” 355,000 lives so far that’s cost £1.12m per life saved. The QALY tariff is £30k per year so each one of them better live another 40 years to make it break even. Oh but the average age of death “with” covid is 82.4! So they’ll have to make it to 120. Take that certainty and place it somewhere the sun don’t shine.
Brilliant!!!!!
And don’t forget to subtract all the lost life years caused as a direct result of the NHS not providing timely treatment for genuinely serious conditions (cancers, etc).
This argument is so strange. Do you think hospitals would have been able to provide better treatment for other conditions if Covid had been allowed to let rip?
Have a look at Sweden or South Dakota or more recently Texas and Florida. Or lots of poor countries.
Do you think those countries/states did nothing to limit Covid? Here is Sweden for example:
https://sweden.se/life/society/sweden-and-corona-in-brief
It is based more on voluntary response than mandatory – but what matters is what people do not what they are told to do.
Note that they are on the point of introducing restrictions again for Omicron.
https://www.reuters.com/world/europe/sweden-tightens-covid-restrictions-cases-mount-2021-12-21/
What they are doing now for Omicron is irrelevant. I was in Sweden last year and while it was quieter it was fully open for most things, no social distancing, no masks, no school closures. No comparison to here. South Dakota. Our lockdown in the UK made cases in Sweden drop!
Obviously I can’t comment on your personal experience – when were you there?
Here is an edited version of the Wikipedia summary of some of the Swedish government responses.
On 16 March 2020, the agency recommended that people over 70 should limit close contact with other people, and avoid crowded areas such as stores, public transport and public spaces. At the end of March, 93% of those older than 70 said that they were following the recommendations from the health service to some extent, with the majority having decreased their contacts with friends and family.
On 16 March 2020, they also recommended that employers should have their employees work from home. One month later, statistics showed that roughly half the Swedish workforce was working from home.
The following day, the agency recommended that secondary schools and universities use distance learning, with schools following suit all over the country.
In April, many of the organisations running the public transport systems for the Swedish counties had reported a 50% drop in public transport usage
The same day as the first Swedish death to COVID-19, 11 March, the Swedish government passed a new law at the request of the Public Health Agency, limiting freedom of assembly by banning all gatherings larger than 500 people, with threat of fine and prison.
On 27 March the government announced that the ban on public gatherings would be lowered to include all gatherings of more than 50 people … the ban would apply to arts and entertainment events including theatre, cinema and concerts, religious meetings, demonstrations, lectures, competitive sports, amusement parks, fairs and markets. … The ban on large gatherings had no end-date, and as of late April, the Health Agency was reported as having no plans for when the ban should be lifted.
After being lifted for a period in 2021, private gatherings were limited to a maximum of 50 people and public gatherings of over 500 people were required to implement vaccine passports from December 2021.
On 18 March, the Health Agency recommended that everyone should avoid travelling within the country….. Telia, a Swedish multinational mobile network operator, did an analysis of mobile network data during the week of Easter, and found that most Swedes had followed the agency’s recommendations to avoid unnecessary travels during the Easter holidays. Overall, travel from the Stockholm region had decreased by 80–90%, and the number of citizens of Stockholm travelling to popular holiday destinations like Gotland and the ski resorts in Åre had fallen with more than 90%.
On 18 December 2020, Stefan Löfven, the prime minister of Sweden, announced new and tougher restrictions and recommendations including the use of face masks in public transportation, closure of all non-essential public services (like swimming pools and museums).
October last year. Of course Wikipedia is 100% accurate. It’s beyond dispute that Sweden last year had many fewer restrictions than the UK, a fact which was pointed out incessantly when lockdown satanists were rubbing their hands with glee at the death toll and predicting doom.
I don’t care what Sweden are doing now, their government is as bad as the rest.
Ah, we’re back to the old ‘let rip’ catchphrase are we! The reality is that none of the NPIs can be shown to have made the slightest difference to “covid” case rates. Meanwhile, it is undeniable that many people with serious health conditions could not access the healthcare they required.
The hospitals were not overflowing – for much of last year they were below normal occupancy.
Allowed to let rip? Like it did in Belarus? They manged quite nicely there without destroying normal life.
As we’re looking back on some of the more puzzling early death rates, can anyone tell me why San Marino was from the beginning and still is the number 1 country for deaths per million? I know it’s a very small country but should that really skew the figures to such an extent? It also happens to be the European country chosen to be the hub for the earliest rollout of 5G towers starting in 2019 I think. In terms of the old con theories, I guess we’ve come full circle!
“let rip”
What? like Sweden ‘let rip’?
Probably, since the approach would have been reality based.
‘let rip’ eh?
Of course – you start off with a flawed premise – that government measures have had any significant impact. Which has been disproved multiple times.
I am not a supporter of full lockdowns. I just want the decision making to be done on a rational basis that reflects the uncertainties and possibilities, not press headlines selected to support a campaign.
The only rational decision was to do more or less nothing, beyond
1 Informing the public calmly of the likely risks
2 Provide extra capacity if possible, and improved infection control
3 Investigate treatments
4 Longer term, consider vaccines
None of these were done, in fact the opposite of these were done, plus a load of other shit which cost trillions and made everything a lot worse and ruined billions of people’s lives for nearly two years, and some forever
With number 2, they went way overboard on theatre to give the impression of infection control – none of which was in any previous pandemic plans, and none of which appears to have made the slightest difference to infection rates.
yes but no-one ever presented a cost benefit analysis did they, so all the data mining mining in the world isn’t going help you make that decision. A rational basis of a decision has to include the cost and this will have been the most costly pandemic in human history. It’s been known since summer 2020 that the IFR is around 0.15% – compare that to other pandemics. The headlines have always been dominated by the lockdown/anti-libertarian fanatics and not by the sceptics who have been side-lined, closed-down, cancelled. I just want sanity.
“I am not a supporter of full lockdowns”
Great. In what way would you like to partially imprison me and my loved ones, indefinitely?
There are lots of NPIs that do not involve being restricted at home and allow most businesses to function:
(Incidentally most of these have been tried by Sweden – not sure about the tests.)
No doubt you will claim they are not effective. Unfortunately there isn’t time to go over all the arguments. So I will just say that is what I mean when I say I don’t support full lockdowns.
I don’t give a fuck what you call the above, full, partial or any other kind of lockdown or NPI – there’s no real world evidence that any of them “work” and even if they did, covid is not exceptional at a societal level and therefore does not justify any mandates like the above. If you’re worried about it, distance yourself, wear bio hazard masks, take hourly, get injected with experiment drugs every few months, work from home, for as long as it pleases you. Leave me and my family the fuck alone.
No masks or social distancing when I was in Sweden, no requiment for tests.
Obviously I can’t speak for your personal experiences. Here are details (edited version of Wikipedia) of the measures Sweden has taken and some estimates of the public response. My emphasis.
Social distancingOn 16 March 2020, the agency recommended that people over 70 should limit close contact with other people, and avoid crowded areas such as stores, public transport and public spaces. At the end of March, 93% of those older than 70 said that they were following the recommendations from the health service to some extent, with the majority having decreased their contacts with friends and family.
On 16 March 2020, they also recommended that employers should have their employees work from home. One month later, statistics showed that roughly half the Swedish workforce was working from home.
The following day, the agency recommended that secondary schools and universities use distance learning, with schools following suit all over the country.
In April, many of the organisations running the public transport systems for the Swedish counties had reported a 50% drop in public transport usage In Stockholm, the streets grew increasingly emptier, with a 30% drop in the number of cars, and 70% fewer pedestrians.
Ban on gatheringsThe same day as the first Swedish death to COVID-19, 11 March, the Swedish government passed a new law at the request of the Public Health Agency, limiting freedom of assembly by banning all gatherings larger than 500 people, with threat of fine and prison
On 27 March the government announced that the ban on public gatherings would be lowered to include all gatherings of more than 50 people, to further decrease the spread of the infection. The ban would apply to arts and entertainment events including theatre, cinema and concerts, religious meetings, demonstrations, lectures, competitive sports, amusement parks, fairs and markets. The ban did not include gatherings in schools, workplaces, public transport, grocery stores or shopping malls, health clubs or private events. The agency also recommended that plans for events and gatherings of fewer than 50 people should be preceded by a risk assessment and, if necessary, followed by mitigation measures. Additionally, they recommend that digital meetings should be considered The ban on large gatherings had no end-date, and as of late April, the Health Agency was reported as having no plans for when the ban should be lifted.
After being lifted for a period in 2021, private gatherings were limited to a maximum of 50 people and public gatherings of over 500 people were required to implement vaccine passports from December 2021.
TravelOn 18 March, the Health Agency recommended that everyone should avoid travelling within the country. They also called for the public to reconsider any planned holidays during the upcoming Easter weekend. Telia, a Swedish multinational mobile network operator, did an analysis of mobile network data during the week of Easter, and found that most Swedes had followed the agency’s recommendations to avoid unnecessary travels during the Easter holidays. Overall, travel from the Stockholm region had decreased by 80–90%, and the number of citizens of Stockholm travelling to popular holiday destinations like Gotland and the ski resorts in Åre had fallen with more than 90%. Travel between other regions in Sweden had fallen as well.
Mask wearing
On 18 December 2020, Stefan Löfven, the prime minister of Sweden, announced new and tougher restrictions and recommendations including the use of face masks in public transportation, closure of all non-essential public services (like swimming pools and museums).
Exquisite!
The graph is a perfect illustration of the ‘casedemic’ phenomenon – i.e a fiction.
You’ve been consistently wrong so far, however, so why change now?
It is the same figures that Toby et al use to make their case that cases are plateauing – just presented in a different way. Maybe you should take it up with them?
We’re not joined at the hip to TY. “Cases” are meaningless.
The agenda pushers are anxious, England is falling behind the curve.
They are going to push more restrictions, Boris is irrelevant in this decision.
A small internal cheer when I read Toby saying “for whatever reason” the link between infection and hospitalisation was broken. And also, elsewhere, that the vaccine may have been “oversold”.
I can’t tell you how infuriating it is to see even sceptics in the media say “of course the vaccines are working but-“ as though they were witnesses at a witch trial, terrified of defending their case too much in case they too get accused of witchcraft.
Its time for sceptics – whatever their profile – to start standing up and saying what is clearly the case: that while, if you trust the people providing the data, there might be some evidence the vaccines are useful for the most vulnerable, the reality is that in every single metric that was put forward in support of their use the vaccines have unequivocally failed.
Sadly though the gene therapy has been immensely successful in enabling those really in charge to mandate the introduction of a digital ID system without barely a murmur – which is their end game.
It’s almost as though they’ve been planning this all along.
I mean, if the jabs had actually provided sterilising immunity – there would be zero zilch nein case for any digital ID system – not that there is anyway ( well, only if you’re a sheep).
It’s almost as if they’d been designed to fail.
Designed to fail? That depends on their long-term purpose. That will, unfortunately, become increasingly apparent over the next few years (the rise in mortality rates will conveniently be blamed on ‘long Covid’).
A repurposed fly virus / saline solution instead of vaccine / terrify people to make them ill: that would work. And by the way, the CDC is going to stop using the PCR tests from 31st December because they ‘can’t tell the difference between SARS viruses and flu’.
The article was going so well and then we got the news that the odious twonk Owen Jones has come over to the dark side. Oh dear, that does not bode well. However, on the positive side I definitely see a difference in comments on news sites and Facebook. People are, very definitely, coming over to our side and are starting to say “Hang on a minute”. Why they were incapable of seeing the blindingly bleedin’ obvious before I have no idea.
I now feel dirty knowing that twit and I agree on something.
He went from being pro Corbyn to being anti Corbyn and then pro Starmer pretty seamlessly.
If you ever feel inclined to buy Jones a present, send him a weather vane.
People go mad in crowds but recover their sanity one by one.
I think two things have changed – 1. a lot of people who were double jabbed and thought “OK, I’ve done my bit”, have been shocked to see that they are a) required to have even more jabs and b) are still restricted in what they can do; and 2. people can see that omicron has been vastly oversold, for which we should be thankful to the South African medics for standing up for the truth and for the UK journalists who rather belatedly have allowed some sceptical voices onto their front pages.
This is a pretty good reflection. I wonder if we’ll witness a sudden swing in opinion, rather than it just slowly turning?
As per Prof Mesmet, there are probably around 30% of people who have gone along with the narrative for a quiet life rather than because they are true believers – I think it is they who are starting to wake up. The 25% of diehards may never wake up, sadly for them.
I think the publicity about the No. 10 parties has had quite a big effect too. Perhaps not the effect the leakers may have planned – that people would be angry at the politicians for their hypocrisy. I think many people have seen the pictures and thought “hmmm… if they weren’t worried about a deadly virus, why did they introduce all those rules?”
it’ll be led by the MSM (other than the BBC) who will smell a great opportunity to sell more of their crappy newsprint with headlines like “It’s Over”.
My original estimate was that would be early spring, then Boris (assuming he’s still around) would eventually emerge in early summer to crow over the success of his covid policies.
By the looks of it, this could move much faster than that.
Whatever you think of Jones, he’s listened to by many on the left – if he’s changed sides that has to be for the good as he’s in a position to influence some of the most extreme bedwetters out there.
If the whoopsies turn against the narrative then Boris is knackered, the queens always get their way.
Or Jones gets an envelope from Bill
From the OED Political Section:
Jones (n): an object for determining which way the wind blows.
I did think this, then I read the comments and its still Guardianista bed-wetting central. Here are some of my personal favourites, with my emphasis:
“That isn’t the case with Omnicron. All evidence points to this variant being far less dangerous than previous variants”
Yes, but that was because it evolved in rural Africa where there wasn’t much contact between people, so it had to be less lethal or it would kill its host before being passed on.
Now that it’s circulating in big cities the selection pressure not to kill people before being passed on is less. So there’s no reason it can’t hybridize with the Delta variant and become a Tau variant which is as lethal as Delta and as infectious as Omicron.”
“I think you’ll find drowning in your own juices in a plastic tent, or watching a loved one doing the same, is substantially more ‘bleak’ than missing out on the pub for a couple of weeks and wearing a bloody mask.”
“There seems to be a cognitive dissonance/inability for many people to realise that we are living through a global respiratory pandemic, of the sort not witnessed for almost a hundred years. Despite the monumental scientific achievement with respect to the vaccines, there are still enough not vaccinated (and importantly, poorer countries with very poor vaccination rates) that some social controls are going to be needed during these peak waves. We either accept that, that some (limited) controls on personal freedoms and high-spread activities are needed, or we accept that it’s fine to clog up hospitals with people suffering from the virus, preventing other vital care from taking place, aside from those injuries and deaths caused by the virus itself.”
You can practically smell the shit in those people’s pants from here. Are ya scared yet, are ya?!
I suspect Boris Johnson will manage to get Graham Medley to come up with the modelling needed for a post-Christmas lockdown.
no need. As the Corona dashboard states “no reporting on 25 and 26 December, Retrospective numbers by publish date for 25 and 26 December to be added to 27 December”.
Then all it takes is for the BBC, Sky etc to fail to mention this to stoke up demand for a new lockdown.
OK – the original super mega killer strain of Convid which saw the world turned upside down in its name had a survival rate of 99.85pc – or 99.9pc as your teacher would have said to round it up to – according to the worlds most highly regarded and decorated epidemiologist Professor John Ioannidis – and the British government also confirmed it was only a low mortality rate virus in writing – if “it” ever truly existed at all which is questionable – yet somehow this strain is 80pc less deadly. Got it.
Merry Fascist Communist Convid Christmas everyone. Enjoy the tyranny
BREAKING NEWS ! Prof Dr John Ioannidis Stanford University On Real Data On Coronavirus Pandemichttps://www.youtube.com/watch?v=btvDL6kIDsA
Welcome to The Internet of Bodies
https://www.bitchute.com/video/eqHqp6t1n7ob/
Related:
Klaus Schwab and his great fascist reset
https://winteroak.org.uk/2020/10/05/klaus-schwab-and-his-great-fascist-reset/
Of Convid: “its mild” said Klaus Schwab
Status of COVID-19
https://www.gov.uk/guidance/high-consequence-infectious-diseases-hcid#status-of-covid-19
But I think we can all agree, its all been worth it.
Enjoyed the cartoon.
For anyone who needs some seasonal light relief Damian Thompson has a unique humorous take on all this:
Eccles is saved: The Book of Covidicus 22: passports, please! (ecclesandbosco.blogspot.com)
“that will leave the gloomsters of SAGE looking very silly indeed.”
Will it – really?
The only consistency in SAGE pronouncements has been their utter absurdity. In October 2020, I did my own ‘informed guess’ about mortality after Whitty’s absurd predictions of Armageddon. It was (needless to say) far, far more accurate than the modelling-based crapology.
… and this is the consistent record of the SAGE predictions – nonsense. But are they seen as ‘very silly’???
In my experience, the GBP are happy to return to the stale sick and lap it up as if it were nectar. I have been amazed at the sublime general ignorance about the ordinary winter virus that is ‘Omicron’.
It’s pathetic. People mostly don’t understand ‘critical thinking’.
In gloomier moments I ponder that the Soviet regime lasted 74 years and Communist China. has been going for 72 years. The Warsaw Pact took 45 yrs to fall apart. I’m 68 and don’t have that long to wait for democracy to return!
Scotland, 17302 infections in 20-59, 15 hospitalizations (p.18)
https://www.politico.eu/wp-content/uploads/2021/12/22/Scottish-Severity-Study.pdf
Ferguson & Imperial changing course
https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/report-50-severity-omicron/
Overall, we find evidence of a reduction in the risk of hospitalisation for Omicron relative to Delta infections, averaging over all cases in the study period. The extent of reduction is sensitive to the inclusion criteria used for cases and hospitalisation, being in the range 20-25% when using any attendance at hospital as the endpoint, and 40-45% when using hospitalisation lasting 1 day or longer or hospitalisations with the ECDS discharge field recorded as “admitted” as the endpoint
This is the most pessimistic scenario, as in 204,000 cases already (Omicron & SGTF) there are 195 hospitalizations. Quite ridiculous
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1043466/20211222_OS_Daily_Omicron_Overview.pdf
Enough with the ‘worst case’ modelling already. What is the ‘most likely’ outcome?
Model that you corrupt fsckers.
as Graham Medley told Fraser Nelson they are not asked for “most likely” outcome. I suspect that Twitter exchange is the real reason the Cabinet did not choose one of three options presented
Boris needs to pretend that this Omicron thing is super terrible so he can extend the covid passport mandates, so more lockdown is guaranteed.
If there is no lockdown, how is the mad modeller going to get away with it again by claiming the “counter-factual” argument, namely that without his lockdown, the doomsday worst case scenario would have happened? We let him off the hook with Sweden, but I don’t think we’ll be this forgiving a second time around.
It’s time the government asked for a new deck of independent sage, the current lot can’t count dominoes let alone provide correct information for this pandemic.
Sage need to grow some onions.
You do realise they’re called iSage for short (ice age – get it?). Could be a covert message to let people know we are currently in a Grand Solar Minimum and aren’t heading for global warming – far from it. Is it another acronym joke like Spi-B and Nervtag?
Kim Jong Johnson will have his mind made up for him, either by those threatening to oust him or by those trying to terrify him into restrictions.
He has no ideas of his own.
Johnson does not have the courage to do what is right and just say no – he will fall into line with the rest of bullying cowards like Drakeford and Sturgeon who are both on a power trip.
I was recently talking to a virus and they informed me that COVID-19 was an imposter! At first this news was difficult to comprehend. I asked for proof that I wasn’t talking to myself. What proof do you need? Confused and not having a clue on how to answer that question, I said, a graph or something, not knowing how it would be presented or how I would even begin to interpret it, or some statistics, I blurted out, equally unsure whether this would be useful knowing how easily I give up trying to check a receipt from Tesco’s! They said and this is where they lost me completely, that they were one of 380 trillion viruses living on or in my body, the conversation then began to gravitate towards profanities…….ending with, unconsciously you know it’s all bollocks’!
I remember saying this in March 2020 on Facebook and having my post banned and someone calling me a clear and present danger. Mmm, I thought, really following the science?
I am relieved as anyone to hear of the relatively positive news from SA data and can feel the panic subsiding a little in todays news stories. It’s good news for families for Christmas and it’s hope for the New Year.
BUT, I’m afraid I won’t forgive or forget the villification of vaccine skeptics in a hurry. Those people who DARED to suggest that people who for whatever reason have not yet got their first jab should be denied healthcare are DESPICABLE and I will never forget the names of those who suggested such an atrocity.
The data has always been clear to anyone with a grasp of the difference between percentage, proportion, and absolute and relative risk of both covid and the vaccines. The fact that these differences were NOT made clear to those who do not understand the significance, and to my mind outright misrepresentation of the data for people to draw erroneous conclusions, is one of the biggest failings in this whole sorry mess.
We are not out of it yet either, with people now convinced of vaccine effectiveness against any variant, no matter how extinct or benign, it is going to be very difficult to get rid of the scourge of vaccine passports. Notice how all todays ‘good news’ was given in relation to vaccinated people, with no information on the rates for unvaccinated, DESPITE the fact that the SA data is biased towards UNvaccinated people. So now having created pure hatred against them, the MSM has now erased them from the narrative completely. Bah humbug.
Here is some of what happens next in that story…
A million deaths a day by the end of the year – that points to pretty much the entire country by the of Jan. Even a double-plus-exponential growth rate runs into a limiting factor — it runs out of people to infect. Sajid expects us to die several times over to keep up the numbers!
I’ve not noticed anyone in the gov or media mention it’s summer in South Africa. Surely that would have been a good argument for scaremongering. Is that because they want maintain the myth this can’t possibly be seasonal?
They will surely lockdown this winter. Otherwise it will be more difficult to lockdown next winter.
More and more I’m convinced they are trying to isolate people so they can divide them. Is it any co-incidence woke appeared at the same time directly targetting minorities while pretending to be their supporter?
If I were black I’d like that not to be the most defining thing about the way people see me. I might prefer they see I am kind, smart, fun etc. Not allowed any more – BLM says the defining thing about you is you are black.
Same for LBQTI(etc). Unvaccinated are ahead with all this and the public will be against other minorities before long.
Fear, isolation and hate of minorities. It’s not been this bad since the last time they tried it and because it’s centralised there isn’t a nation to have a war against this time.
Sorry, chaps, but I appropriated the Cassandra moniker a while back, many of my prophesies having been proved correct.. However, Galileo remains open. He is perhaps more apt, as he was persecuted like some of the sceptics of 2021. He would doubtless have been no-platformed in today’s world.
I suspect pubs and restaurants will be ordered to close for a few weeks and then allowed to reopen but with the use of “certification” to “keep people safe” thus achieving their end goal, the introduction of vaccine passports into every day life. I hope I’m wrong.
“See! We’ve saved the day once again. Just as well you listened to us, Prime Minister.”
Perceptive comment by Toby re: the ICL ‘modellers’.
From day 1, they’ve made hugely exaggerated claims based on dodgy models, invited every kind of NPI insanity, and then given themselves a huge pat on the back when it does fizzle out. That is exactly why they can make crazy claims: they can always say the models worked because the correct preventative steps were taken, and catastrophy was avoided.