
We’re publishing a guest post by our in-house doctor looking at the latest NHS data, including ICU data. Conclusion: Omicron hospital admissions in the community are declining and are unlikely to result in severe COVID-19.
Before diving into the numbers this week, I’d like to give a big shout out to Ms. Kate Josephs CBE, formerly the Director of the Cabinet Office Covid taskforce. According to the Telegraph, which broke the story of her leaving party, she “literally wrote the rules” in relation to societal restrictions.
Ms. Josephs took to twitter yesterday to apologise for attending a leaving drinks party on December 17th 2020, when she had been substantially responsible for putting the rest of the country under house arrest. She writes about being “truly sorry” for attending the event – she clearly means she’s sorry for being exposed.
The Telegraph has a helpful timeline graphic showing the dates of the many known social events in Whitehall against a backdrop of prevailing restrictions at the time. I had no idea being a civil servant was such fun! It is interesting that the parties all cluster round periods of maximum lockdown. The brief period in the summer of 2020 was a social desert for civil servants. Maybe they were all on extended holidays?
I love a good laugh, so I’d genuinely like to thank Ms. Josephs. I haven’t laughed so much since Dominic Cummings took a 20-mile drive to test his eyes. By being exposed, this formerly faceless apparatchik has performed a valuable public service. Her hypocrisy reveals the absurdity of what Lord David Frost calls “Covid Theatre” – pointless petty regulations enforced so that the Government appears to be “doing something”. If Kate Josephs really believed in December 2020 that covid was a serious threat to her health, would she have turned up to a drinking session in a cramped Whitehall office? I think not.
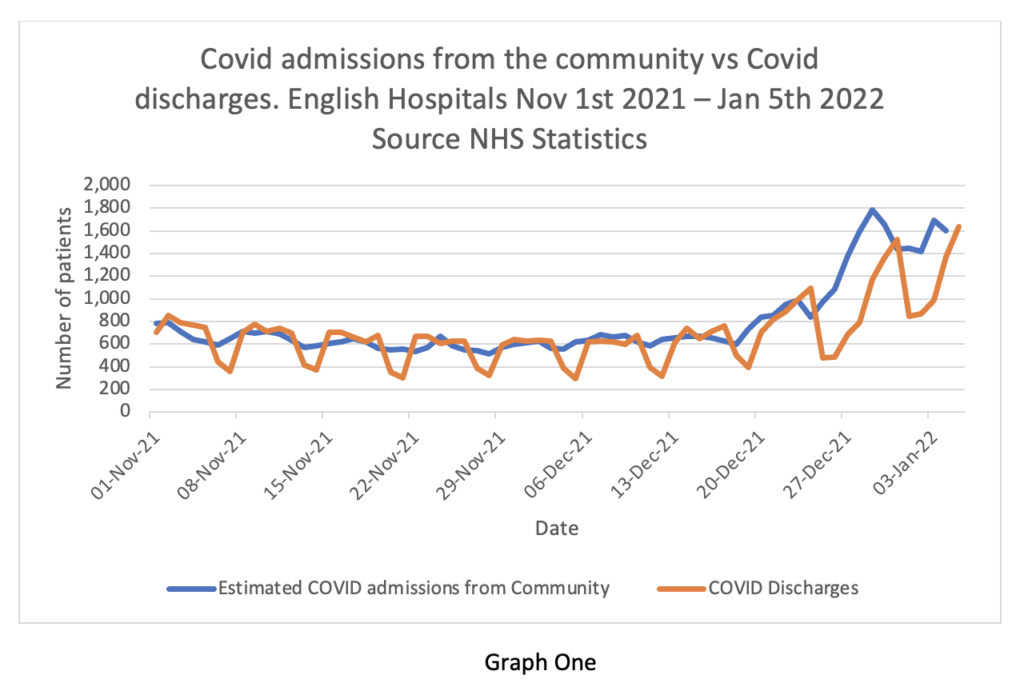
After a brief moment of levity, I turn to the stats. By now, we should be well into the ‘nailed on tsunami’ of cases which are overwhelming the NHS – but of course we are not. Covid admissions from the community are falling, particularly in London, where they have been on a downtrend since the turn of the year. This week we have the monthly data summary from the NHS. Graph One is instructive. It shows daily admissions (blue line) compared to daily discharges of Covid patients (brown line). The weekend effect of discharges is clearly visible, as is the lag over the festive period. But in general, discharges have kept up with admissions. As these two trends are in balance, there should be no problem.
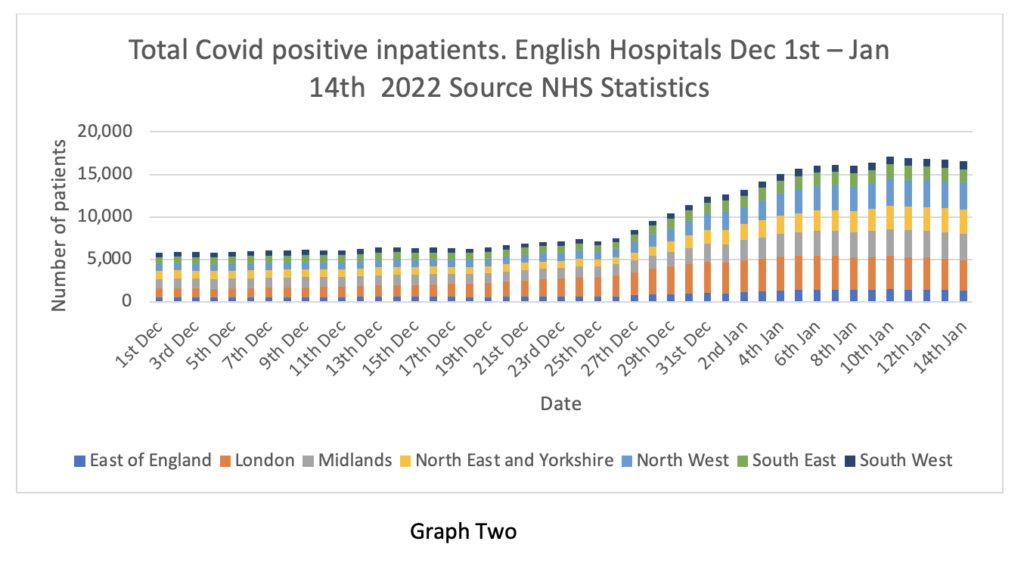
Graph Two tells a different story. Although Covid admissions and discharges are in balance, the total number of patients testing positive in hospital rose in late December and is now plateauing. This is the figure of over 16,000 patients repeated nightly by the mainstream TV news channels. How can this be?
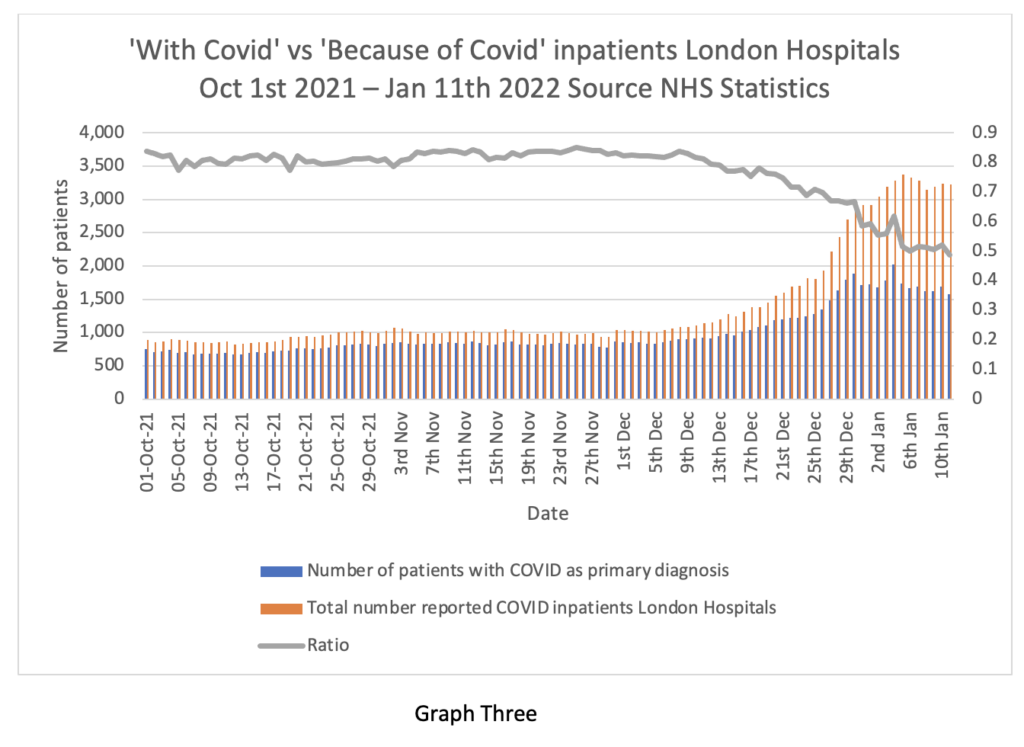
Graph Three explains. The Primary Diagnosis spreadsheet this week shows that the percentage of patients in hospital with incidental Covid is increasing. Graph Three shows the numbers for London. Over half of the 3,200 patients in London hospitals ‘with Covid’ are not actually unwell with Covid. This is most likely to mean that in-hospital spread is the main reason for increasing inpatient numbers, but this is of questionable clinical relevance, as most of these patients are asymptomatic.
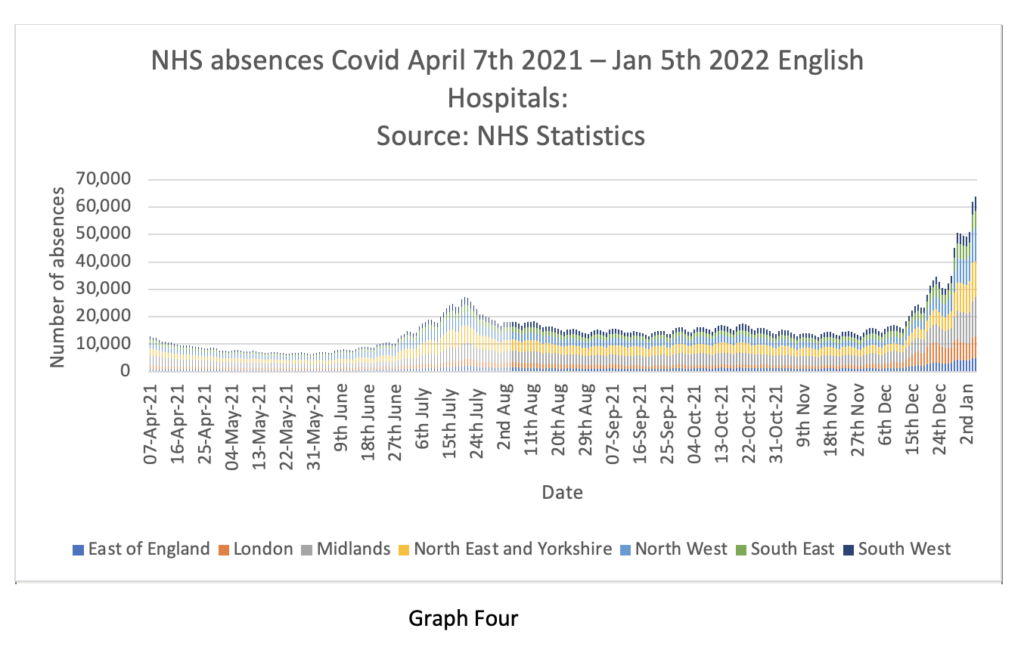
Graph Four from the monthly summary packet shows the real reason for the dramatic headlines. At the end of December, the NHS sent over 60,000 employees home to self-isolate. The majority were asymptomatic with positive tests or had merely been in contact with a person testing positive. If testing of asymptomatic staff and patients ceased tomorrow, this ‘problem’ would evaporate overnight.
The ICNARC database this week contains some interesting information about recent ICU admissions. There has been virtually no information released in relation to the variants of Covid infecting ICU patients. Colleagues tell me that all ICU patients are tested centrally for Omicron, but this information is not passed back to clinicians.
ICNARC has compared the clinical characteristics of patients admitted to ICU since December 30th (mostly assumed to be Omicron) with the prior cohort (assumed mostly Delta). The detail is outlined on tables 17-19 on pages 49-51.
In summary, patients admitted since December 30th are less seriously ill than the prior cohort – their oxygen requirements and respiratory ratios are lower than the presumed Delta cohort. It is revealing that only 72% of the patients testing positive for Covid since December 30th had Covid as the primary reason for requiring critical care – before December 30th, this figure was 93%. In other words, a third of the patients in ICU ‘with COVID’ are not unwell with the virus.
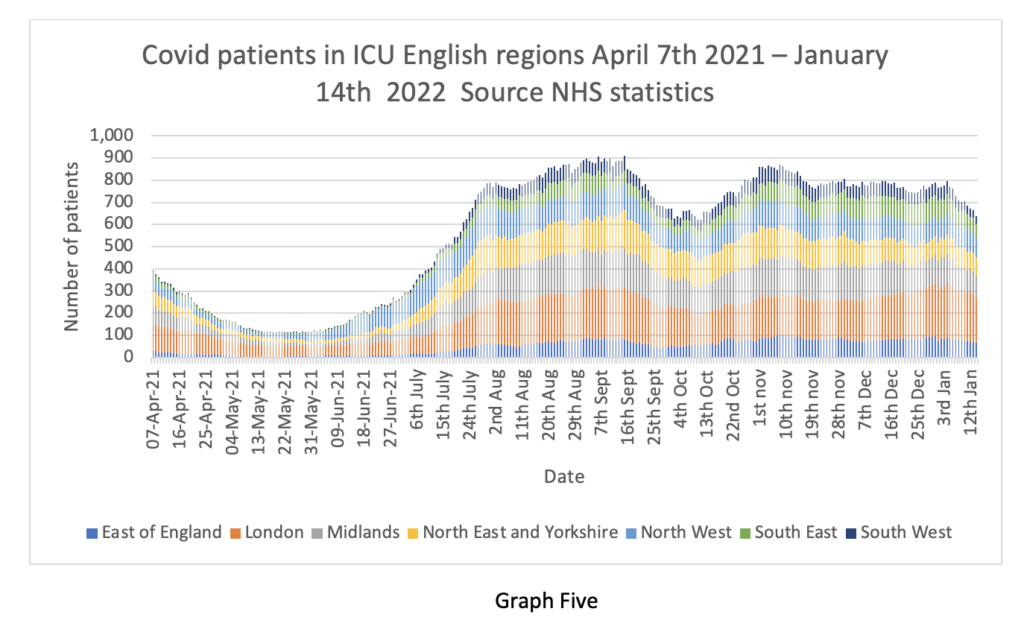
This is good news. Although we don’t have precise information about variants, it’s reasonable to conclude that Omicron is very unlikely to cause serious illness. ICU numbers continue to fall (Graph Five) and are not really any worse than a normal flu season. Dr. Mikko Paunio, writing in these pages, has calculated the Infection fatality rate from Omicron is lower than seasonal influenza using high quality Danish data.
I have seen no commentary from senior NHS leaders on this encouraging news. Readers may wish to consider the following counterfactual: had the numbers shown Omicron to be worse than Delta, what sort of media coverage might the ICNARC data have received?
Minutes of the SAGE meeting 102 on January 7th reveal that all the points I have made today were recognised by SAGE last week. Lower severity of disease, lower rate of admissions, shorter hospital stays. SAGE also acknowledge in this meeting that societal restrictions are unlikely to have any effect on reducing hospitalisations at this stage. This was reinforced in a consensus statement from SPI-M-O.
Yet coverage in the media continues to emphasise the risks of removing lockdown measures. The Financial Times reports that “scientists warn on dropping England’s Plan B Covid curb too soon”. It’s puzzling that the FT journalists have read the same literature as I have and come to such radically different conclusions.
The Mail reports that Warwick University modellers predict an ‘exit wave’ in the summer with 10,000 daily hospital admissions. How they came to this conclusion is a mystery to me – for comparison, hospital admissions peaked on December 29th 2021 at 1,783.
At the risk of sounding flippant, had these numbers been analysed in connection with an upper respiratory virus in 2019 we would probably have concluded there was a nasty cold going around. In 2022 we look at the same data and conclude there is a deadly virus which will overwhelm the health service. Misinformation seems to spread even faster than Omicron.
Misinformation aside, one of the more troubling aspects of the recent past has been the distortion of normal medical practice. Drs Mordue and Shaw writing in these pages have contributed fine articles on this point – chapeau to both of them.
Readers interested in discovering how doctors are expected to behave may consult the General Medical Council’s document Good Medical Practice. I entirely endorse everything in this pamphlet and strive to demonstrate these principles in my professional practice.
Readers will discover many references to respecting patient choice, even if it is different from their doctor’s advice. Doctors are specifically prohibited from discriminating against such patients. There are cautions about assessing the risks of harm from treatment and explaining these before requesting consent. There are detailed injunctions around declaration of conflicts of interest, acknowledgment of mistakes and transparency around analysis of harms. There are explicit passages in relation to respecting colleagues and the rules around personal conduct.
Readers may wish to consider to what extent these rules have been followed by public health doctors in relation to lockdown advocacy and vaccine mandates. Where guidance has not been followed, readers may wonder why deviation from professional norms has been tolerated and even encouraged by non-medical managers and politicians.
The history of the NHS over the last three decades can be interpreted as a power struggle between unregulated professional managers and groups of clinicians for control and influence. The managers have overwhelmingly triumphed and Covid has been the apotheosis of that victory.
Medical practice is now subservient to demands of management. Doctors are becoming functionaries of the system rather than independent clinicians. Medicine is at risk of becoming a profession in name only, with a primary duty to the NHS as a whole, rather than to the patient as an individual. As Steve Baker MP has noted, the recent past has seen a fundamental reshaping of the relationship between the citizen and the state. Doctors are morphing inexorably into civil servants.
Party on.
Stop Press: Daily Covid cases fell by 44% week-on-week, dropping to 81,713, with deaths dropping by 8%. MailOnline has more.










To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Good news about Covid/Omicron. And now that Kate Josephs, Johnson, Starmer et al., have all been exposed for the lying and deceitful hypocrites they are, I think I’ll never abide by a Covid restriction ever again. What’s good for the goose is good for the gander, and all that…
Once everyone knows that (as Neil Oliver said recently on GB News) the great and the good have NEVER feared COVID (because they know the reality of the situation), the fear amongst the vast majority of the general public will disappear.
If the power that be and their string-pullers from global businesses, the WEF et al try to push back by ramping up the authoritarianism and not doing the opposite, the backlash will be swift and severe.
Somehow I doubt if all those ‘remote retreats’ the billionairres are now buying up will be safe – they will eventually all be brought to justice for their crimes, unless they top themselves first, the coward’s way out.
I read that New Zealand is proving very popular for possible ‘remote retreats’. Imagine – communities of very wealthy socialist leaders/scientists/politicians/modellers etc., surrounded by their personal armies, living in isolation from normal society, in fear of The People, ruled over by the Godless Jacinda.
What fun we could have cutting off all their energy and supply routes, shooting their carrier-drones out of the sky.
Argentina was the Nazi post-war escape route, is NZ the chosen Utopia for the Covid-Nazis? They’d do better to admit they’ve lost and fall on their swords, show honourable intent for once in their pointless, wretched lives.
I agree – cut off their supplies and services and starve them out! Make their lives hell just as they’ve made ours.
Kate Josephs – typical civil servant. Spent her working life in meetings talking bollockology but never did a day’s real work and creamed a fortune off the tax payer. Now sitting on a glorious pension and reflecting that perhaps she got out just in time.
Horrible people.
Correct.
Still creaming it in on at least £190k per annum at Sheffield City Council.
Ah, the tree shoppers…
Aw, how unkind. This lifelong server of the people, Duchess Josephia, has had the decency to get a lackey to post an apology on
a toilet wallTwitter. Do we want blood or what? She deserves treble the pension and everyone to bow and scrape when she walks past, for the rest of her days.That’s an uptick for you Mr Piggles simply for the word bollockology.
Marvellous!
If we’re into new words, a friend commented the other day that Boris Johnson was ‘testiculating’ – waving his hands in the air whilst talking balls.
That’s a cracker too.
Think he nicked that from Viz’ Profanasaurus
That’s made my Sunday morning 🤣🤣
Thank you very much.
I must say it is a word of my own devising – too many hours spent listening to wannabee Hitler’s talking nonsense.
If any of my ex work colleagues are on here – very unlikely – they will know who I am just by my use of that word.
One of the finest words to grace my eyes. Wish I’d have worked with you.
Very kind. Thank you very much.
Sounding suspiciously like an anti-authority ideologue, there, Hux….
Cheers 🙂
There was – and I don’t know if it is still the case – a perfectly legal way to recoup “funds” from what were called “approved” and what are now known as “registered” pension schemes.
The device was/is a “lien” clause and catered for recouping the funds/costs of what might have been legally described as “negligent acts or omissions” on the part of the member. It should, if it was included in the documents of the pension scheme, have been used against Fred Goodwin, for example.
It is a rarity; HMRC has a protocol to enable this but the burden of proof is high, and may only be feasible if criminality is involved (I am out of touch with this) . But if “equity” as a moral concept were used, these apparatchiks should have to go through a formal defence of their actions, if deemed negligent, where they are superannuated by the taxpayer – the list therefore, from 2016 onwards at the very list, is theoretically very very long from SAGE/CS remainer Project Fear/politicians …including the PM whose pensions is better than his “civil servants”.
I would love to serve on the body to assess these people; payback would not come into it, and they would have to pay for the costs of the investigation even if it found in their favour, the costs to be deducted from their retirement tax payer funded pension. But I do want these bastards to suffer something akin to the sustained existential pressure they have inflicted on the UK….
To misquote Gimli “forces against us – overwhelming; chances of success – non existent; what are we waiting for?!!!
…spent her working life in meetings talking bollockology.…. – excellent HP ! I might borrow that phrase if you’d be so kind ?
Bollockology word of the month. It describes what people falsely in power learn to make decisions effecting others that they have absolutely no knowledge about and have studied nothing about. It defines the knowledge of most members of paliament and how much appointed ministers know about their remit. Matt Hancock was a prime example.
As to the opening gambit of this plandemic Great Reset chess game, GloboCap’s done very well, over two years in with no viable pushback to its core narratives. Germany, Austria, Italia and France all well along with entrenched digital trak-n-trace control matrixes… Canada, Australia and NZ too acquiescing to full totalitarian Stormtrooper control.
All part of the lockstep coordinated societal and economic demolition, riding on the coat tails of coronaphobia for the greater good.
Bozo of course has been dawdling, sensing the English Brits have become virus fear porn fatigued… and around Xmas was clear too many of us were increasingly becoming unblinkered from the mass hypnotized Covidian cultism… I sense alt and social media may be the future target for the predicted WEF Cyber Polygon attacks.
I’d bet money too on the Davostokracy not having foreseen the black-swan that is Omicron. It’s a damp squib snifflete highly infectious variant, that renders all draconian interventions and Govt legitimacies of LFTs, PCRs, Masks. Boosters, VaxxPassports and quarantines the whole Covidian panopticon shit-show redundant.
Why? Good old fashioned, old normal mass herd immunity. This is a BIG problem for them. In a sane moral, ethical world Covid tyranny should be done, dusted and buried for good by no later than this looming Easter.
Fortunately for us here in the UK, in part due to our special relationship with good ole Merikha, its key to note that the Supreme Court’s legal crush down of Biden’s federal vaxx mandate for businesses last week is already impacting corporate OEMs.
https://www.zerohedge.com/covid-19/general-electric-abandons-bidens-vax-mandate-after-scotus-ruling-while-nike-doubles-down
This bodes well for us, with many of the very same businesses operating here forming precedents. I sense an inflection point, right here, right now… just as the anti-vaxx desperation is reaching breaking point.
https://twitter.com/JimmyKimmelLive/status/1480777671076311042?s=20
Finally, methinks it benefits us to have Bozo as the current Tory figurehead, his hedging/dawdling style is aiding the cabal collapse cause, god forbid bankster backed slick Sunak, Jabbit or ghastly grovelling Gove gets the slot. Heaven forbid!
Have a great weekend all.
Superb analysis.
I am totally puzzled why corporates have taken on the responsibility of trying to protect people from an airborne virus. Presumably it is being done under some misguided application of H&S, guided by know-nothings with no knowledge of risk mitigation. I guess the fear of being sued by someone claiming to have caught the disease through their negligence may play a part, though I cannot see how the claimant could prove the disease was caught at a specific time and place.
Their interpretation seems to be to eliminate any conceivable possibility of transmission, irrespective of consequence, whereas simple evidence-based risk mitigation would suggest ‘do not come in to work if you have symptoms of the disease” would be sufficient.
On the vaccination front, I came across a report of a Puerto Rican (US colony) healthcrare provider segregating vaccinated and unvaccinated employees in separate buildings. The vaccinated are dropping like flies, while the unvaccinated work as normal. I suspect this was not the intended outcome!
Any credible conspiracy theorist would believe someone super smart deliberately released Omicron to fuck off all the parasites.
Well possible. Thank you to that gof lab which created an vaccine variant as a quiet act of rebellion.
or Hunt?
He just misunderstood the title ‘Party Leader’
What’s worse than Emperor’s New Clothes?
Forcing men, women, and children, to walk about naked for two years.
Why so bad? There’s hardly anyone left to laugh at them!
Mr or Ms In-House Medic – Are you aware of a single case where omicron has caused Covid?
Notes
1) Delta and “original” variants would have to be absent.
2) Covid requires double pneumonia.
Just received a council leaflet saying that if you test positive for Omicron you there is no need to isolate if you have been vaccinated but must if you haven’t!!!
Ignore their tests, job done.
“Latest NHS Data Suggest Omicron No Worse Than a Bad Cold”
Well, duh!
Whitty said SARS-CoV-2 had mutated to an endemic form about a year ago. Endemic means simplistically that everyone gets it and almost no one dies. The symptoms of omicron are coughing, sneezing, headache, runny nose and have been from day 1. Omicron is and always has been a common cold variant, forming the fourth such variant of coronavirus causing the common cold. The PTB knew it was mild, as confirmed by SA medics from the time it was declared a ‘variant of concern’ but pimped the fear (and boy did it work) to push more drugs as demanded by Big Pharma.
Edit: A while back, the government also used some excuse to extend the emergency by another three weeks, as required by the 1984 Public Act ‘significant and imminent threat’ clauses regarding a state of emegency. It would seem that the common cold is now a significant and imminent threat!
“Whitty said SARS-CoV-2 had mutated to an endemic form about a year ago.”
Could that have been March 2020 when it was officially downgraded from a highly infectious disease……just askin…..
How to account for the cumulative insanity of society fearing a common cold for two years as though it were a Black Death?
I need not continue. But they will forever insist THEY GOT IT RIGHT.
Almost over now? It’s ‘too big to fail’…
Not sure about the deification of democracy – destruction would be better.
With ‘democracy’ on a pedestal, its outward form could be used to justify its practical subversion.
Democracy has been in decline for some time was my point, since it could never be reformed. Whatever the public were presented with was ‘democracy’: even their house arrest and manipulation. Few questioned this.
Certainly people didn’t question the diktats – my aged mother told me that the government had told us all to hide away so I wouldn’t be able to see her until at least August 2020. I ignored her, she is still alive.
She also told me I was pig-headed and stupid for not being jabbed; she is still my mother so I continue to love her and visit her, despite her total belief that the Telegraph, Government, maybe BBC, wouldn’t lie to us all. One day she will realise that I was right and she, and millions of others, have been psychologically manipulated.
the Telegraph, Government, maybe BBC, wouldn’t lie to us all”
Ask her if she ever fund Saddam Hussein’s WMD capable of being launched within 45 minutes. That claim was used to justify a war of aggression against Iraq, resulting in >500,000 excess deaths – mainly women and children.
No, that would be too cruel
and directly led to the outing of a very honourable man, a process aided and abetted by two of the worst examples of humanity – Blair and Campbell.
Well Bliar, the price of your elevation to the Garter is the immediate release of ALL official documents relating to the investigation into the death of Sir David Kelly and an inquest opened and adjourned; any finding of culpability on anyone’s part in the enabling of Dr Kelly being identified to result in criminal proceedings….no plea bargainings…
Ms. Kate Josephs CBE? Hello; I’ll be your helicopter pilot for today. Please step aboard… no need to bother with the seat belt….
Testing, schmesting….
So for nothing more than a mild cold everyone rushed out to get a booster shot with a vaccine that has not been throroughly tested yet? Absolutely incredible!
Shortly after the governments statement about omicron last year and the reintroduction of mask mandates in shops again (which I now believe was Johnson just trying to keep partygate off the front pages) the following day I witnessed huge queues of people lining up for the booster shot outside NHS covid drop-in centres that usually would have only had a handful of people waiting outside on most days – but immediately after Johnsons announcement there were suddenly huge queues appearing outside drop-in centers and pharmacists everywhere – all risking a possible severe or even fatal reaction to the untested mRNA jab for a virus that before covid19 would have been shook off as nothing more than a common cold.
Christmas came early for Big Pharma. Possibly the last big splurge before the wheels fall off.
Someone must take the pruning shears to the Civil Service. It is bloated, highly politicised and lazy. All this on the public purse including gold plated pensions and excessive holidays.
It opposes checks on immigration and seeks to do everything it can to wreck Brexit.
It is the enemy within, the Fifth Column, and must be tackled head on.
“Before diving into the numbers this week, I’d like to give a big shout out to Ms. Kate Josephs CBE, formerly the Director of the Cabinet Office Covid taskforce. According to the Telegraph, which broke the story of her leaving party, she “literally wrote the rules” in relation to societal restrictions.”
The whole purpose of the ‘why now’ release about politico partying is to reinforce the idea that imposing random meaningless rules is good. People are encouraged, sorry nudged, to criticise the ‘unfair’ nature of breaking of the rules rather than their imposition in the first place.
Yep, the Globalist’s own the MSM. Every breaking “news” story is geared towards psychologically conditioning the sheep.
Politicians are on record as having openly and shamelessly lied through their teeth about everything in relation to COVID-19. Everything. There’s no doubt about it, politicians and their advisors have the blood of many dead people on their hands. And they don’t give a hoot. They couldn’t care less.
So, how on earth can people now swallow the tripe that they are worried and apologetic about people knowing they attended parties?
I also believe the Globalists are getting two birds with one stone via these partying revelations. They want rid of Johnson. Note the recent official utterances about COVID-19 being now normalised and that it has now suddenly morphed into nothing more than a flu.
The Cabal are moving on to the next step, but to do this successfully, they have to condition people to both normalise the last step and frame it in an historical perspective. As you’ve so brilliantly pointed out, the political apologies for breaking the outrageous and needless rules, actually formalise and sanction these very same needless rules in people’s minds.
To get people to consign the last step to an historical perspective, something tangible and deeply embedded in people’s psyches has to be used as the vehicle to carry it and all the hurt it represents into the past.
I suspect Boris Johnson will be that vehicle. I think he’ll be going soon. And when he does go, the Cabal will gain the advantage of many people psychologically consigning lockdowns, nursing home deaths and dangerous vaccines to history with him. In the UK, COVID-19 is Boris Johnson and Boris Johnson is COVID-19.
Then it will be onwards to the next step for the Cabal, with, perhaps, the smarmy Keir Starmer being the puppet in 10 Downing St.
The puppeteer – SAGE/NERVTAG/MHRA/JCVI………”but who is pulling their strings?”….
Check out the photograph of the Queen and world leaders socially distanced for a photo shoot at the G7 summit in Cornwall.
Then minutes later, when the photos are taken, the lot of them gather together in a bunch to shake hands.
The shameless hypocrisy of this. You really would not know whether to laugh or cry at it.
The total abscence of faux media outrage over this is telling. The BJ ‘breaking the rules’ nonsense is clearly a politically orchestrated coup aimed at getting rid of BJ in favour of <whoever is the worst prospect for the person on the Clapham Omnibus> or <whoever is most amenable to Big Pharma>
Then it will be onwards to the next step for the Cabal, with, perhaps, the smarmy Keir Starmer being the puppet in 10 Downing St.
Starmer has been a big disappointment. For a trained barrister he has failed utterly to consider the evidence on lockdowns, masks, and jabs. At least Boris was a journalist by training where you are not obliged to consider the ‘other side’ of the story, but Starmer’s approach would have seen him ambushed in court and his clients convicted.
Disappointment – no way; acting to type – certainly.
He is first , last and always a politician even as AG – he needs to curry favour with his electorate to keep his position; ergo analytical brain function locked away and out comes the voter base pandering knee jerk ( an apt term for him) reaction brain function….if it is coming from his brain and not his arse.
Starmer blocked the prosecution of sex-selection abortionists (for not being in the public interest) after an excellent sting op by the DT :
http://www.ministryoftruth.me.uk/2013/09/06/sex-selective-abortion-and-the-public-interest/?share=google-plus-1
https://www.bbc.co.uk/news/uk-24430356
http://www.sunday-guardian.com/news/fury-in-uk-as-doctors-let-off-for-abortions
Even the Labour shadow AG, Emily Thornberry, called the decision “scandalous” and demanded an urgent review of the decision. Good for you Emiiy.
But Keir is such a nice chap, isn’t he ?
The number of people being treated FOR COVID in the specialist ICUs on ventilation (i.e. the most serious cases) has been dropping for a good 2-3 months, now down to 777 as of 13th Jan 2022.
Apparently the overwhelming majority of ‘in hospital’ stated with COVID are low-criticality patients, those who didn’t know they were positive until a test in hospital because they were admitted for other reasons (not related to COVID-illness), both already seriously ill (including those not/late diagnosed because of the shutdowns) and those just having regular treatments.
That after 2 years the NHS cannot differentiate officially between ‘with COVID’ but has little to no impact on their hospital stay or death elsewhere and those unfortunates who perhaps have died mainly/solely of COVID isn’t incompetence as Toby often suggests but IMHO a deliberate act to hide the reality of the situation from DAY ONE.
That the Italian authorities admitted months ago that 85% of ‘COVID deaths’ were not REALLY from COVID but just the ‘tested positive’ and died of something else rather puts things into perspective, especially as all the fear whipped up by the government and MSM propagandists surely put many vulnerable people into a worse state of mind/health, which likely contributed to their immune systems being depleted – stress is a major factor in the ability (or not) in fighting off illness and disease.
Of course if you Google the Italian admission, most of the hits are from fact checking
liarssites saying that it wasn’t true. On the other hand we have the CDC back in 2020 saying 94% were ‘with Covid’ and 6% were ‘of Covid’, and added to that we have fatalities everywhere averaging over 2 co-morbidities. I think I know which source I trust.This pandemic is melting down faster than Fukushima.
And those responsible need to be fired off inside nukes!
“Colleagues tell me that all ICU patients are tested centrally for Omicron, but this information is not passed back to clinicians.” Then what is the point of gathering the data?
…and why aren’t clinicians demanding the information?
The lesson isn’t that the rules were wrong the lesson is that those making the rules knew the rules were bollocks.
If these people in Government believed there was a terribly dangerous virus going around they would not have been meeting up in large social groups and getting pissed on a near daily basis.
They would have not risked infecting themselves and others, they would not have risked taking such a virus home to their children and loved ones.
That they acted as they did proves they had no fear, they had no fear because they KNEW the claims they were making about a deadly virus was bullshit right from the outset.
The entire thing has been a hoax used by Boris and the Tories against the British people.
So the next question is cui bono and that isn’t particularly hard to work out.
Ah, reminds me of the St. George’s day part that some of us had in April 2020 (I think). Apparently there’d never been so many people in the flat!
Quite brilliant as always.
If science can’t be questioned it’s not science anymore. It’s propaganda. They want to rip on people for taking Ivermectin. I researched and saw the evidence on the internet. Research papers are on the internet for those who wants to see. Top respected world doctors are being under defamation by MSM and vaccine manufacturers. I won’t back down recommeding IVM. You can get yours by visiting https://ivmpharmacy.com
Love you Toby – a knighthood should be yours for the taking – but please please please don’t be an Around Merchant:
“There are detailed injunctions around declaration of conflicts of interest, acknowledgment of mistakes and transparency around analysis of harms. There are explicit passages in relation to respecting colleagues and the rules around personal conduct.”
We’ve said it from day 1. Where’s the common cold gone, where’s pnuemonia. It’s bloody obvious.
In fact if someone is in hospital, intubated and unconscious with covid the doctors call that state “covid pneumonia”.
That should tell you everything you need to know.
I’ve not followed the stupid rules since the beggining and never will.
You don’t say?
Jut read Mindspace 2010 it’s all in that document
On March 20th 2020 I posted a poem on my blog (https://bamjiinrye.wordpress.com) predicting that for most of us coronavirus infection would be no more than a cold. It’s taken a while…
“Latest NHS Data Suggest Omicron No Worse Than a Bad Cold” But listen, Dr Angelique Coetzee, one of the very best of South Africa’s GPs told us that weeks and weeks ago.
Down in SA, people shake their heads and ask “Why don’t the “Crazy English”
listen to us ?”
Omicron is mch easier to catch, but it is much, much less serious to suffer and deaths are very rare. But honest BJ does’t want us to know that, we must go back to being fearful, worried, depressed and deeply concerned.
I jusr wonder why ?
Answer : the MSM will not allow it, in particular the lying BBC.
I suspect one part of the problem with the NHS is that trained doctors, specialists, clinicians and nurses are all to much in short supply or busy to get involved in decision making or administration. Unfotunately this means that unqualified or poorly qualified people are in the roles that really need experience and expertise in these areas are people without those skills resulting in poor decisions and reporting of issues. There needs to be more consultation with the clinical and medical scientific eperts on the front line before decisions are made. Perhaps there should be a minimum level of clinical qualification for anyone in important decision making positions.