Our in-house doctor reflects on the year gone by, noting the Daily Sceptic’s excellent track record of identifying important issues about the NHS’s management of Covid months before the mainstream media.
As 2021 draws to a close, it is customary to reflect on the year gone by and to anticipate what the new one might bring. Looking back, it isn’t excessively hubristic to feel pride in the achievements of the Daily Sceptic community. We have established a good track record of identifying major issues around the NHS’s management of the pandemic before they became widely known.
We identified high rates of nosocomial infection. Denied by the NHS, then accepted. We spotted errors in attribution of deaths to Covid which were due to other causes. Denied, then accepted. We have exposed numerous public misrepresentations of data by NHS leaders. Often denied then reluctantly accepted, sometimes under pressure from the Office for National Statistics. False positives yielded by PCR Tests? Officially denied. Yesterday accepted by the U.S. Government.
Most recently we noticed a substantial proportion of hospital inpatients classified as Covid were in fact incidental infections. Denied, and ignored until this week when the rest of the commentariat suddenly discovered the Primary Diagnosis Supplement, published weekly since July. We have been analysing that data regularly since the summer. For much of the last 18 months I have been repeatedly struck by the observation by the American writer and politician Upton Sinclair – “It is impossible to get a man to understand something if his livelihood depends on him not understanding it.”
This helps explain why, for the last 12 months, the Daily Sceptic has failed to make much of an impact, but something has changed in the last couple of weeks. Even the Guardian now accept that the figures on ‘Covid admissions’ grossly overstate the number of patients acutely unwell, and if opinion polls can be believed, our points seem finally to be landing with the public at large.
Here on the Daily Sceptic, we have been stating the obvious for months, so why the abrupt volte face by lockdown enthusiasts? Before I consider this point further, let’s first examine the data update provided yesterday and what we have discovered about the Omicron variant.
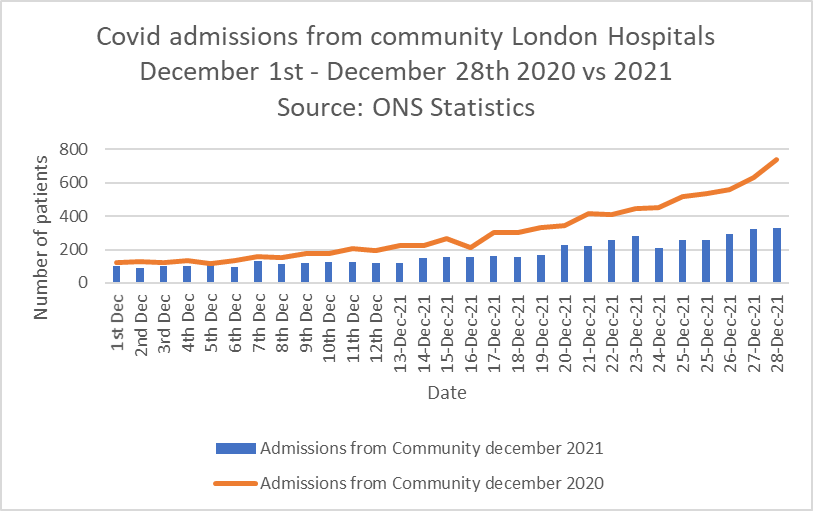
Graph one shows patients admitted from the community in London in December 2020 (brown line) versus December 2021 (blue bars). Cases are slowly increasing but are still about half of the numbers from last year.
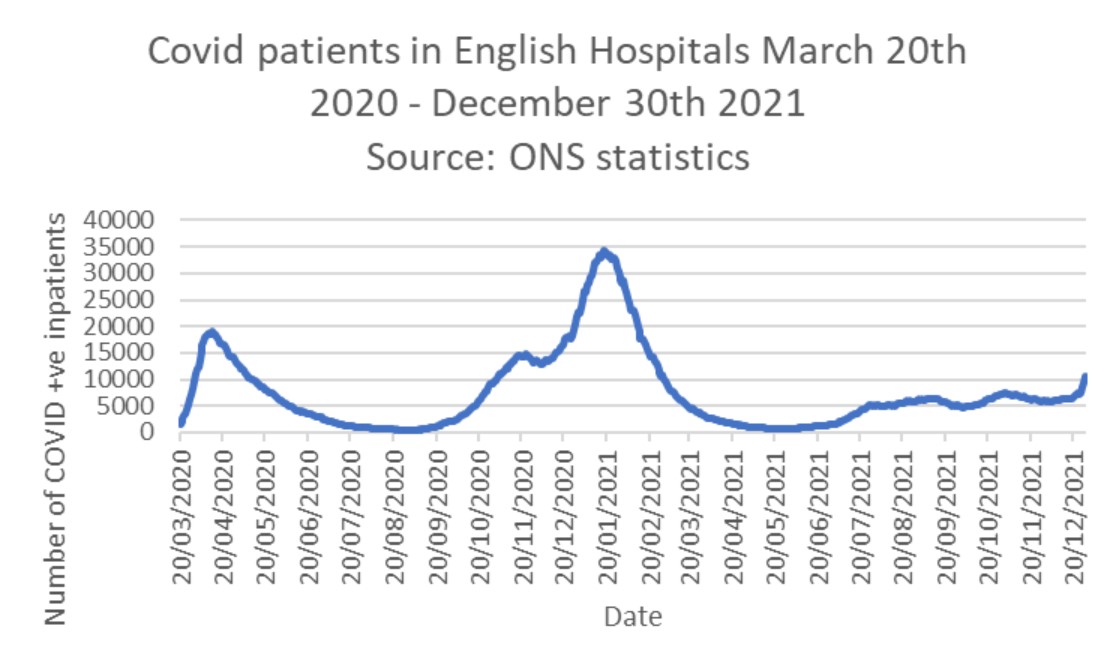
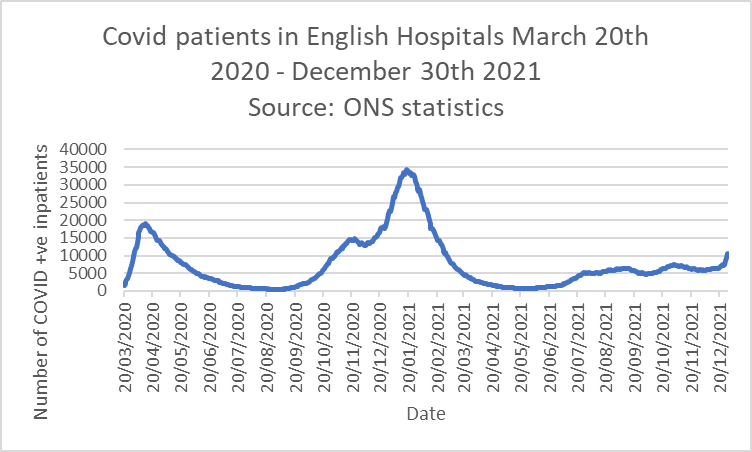
Hospital cases continue to rise. Despite the alarming looking uptick on the right of Graph Two, it’s hard to interpret this data sensibly in the light of reporting lags around Christmas and the difficulty of discharging patients from hospital over extended bank holiday weekends. What we can say is that the number of inpatients designated as Covid in England today (11,542) is about half what it was on the same day last year (22,713).
The disparity between cases admitted from the community and cases diagnosed in hospital still suggests 25-30% of Covid patients are contracting the illness incidentally in hospital. The Primary Diagnosis Supplement is delayed this week for some unexplained reason, so I can’t comment at this time, except to reiterate that the latest info revealed that 29% of hospital cases recorded as Covid were in fact incidental findings. Given the transmissibility of Omicron, this figure is likely to rise further.
ICU bed occupancy both in London and England has not changed significantly. This is not just important from the point of reduced disease severity, but reflects tighter infection control in ICU. General ward figures have now been widely acknowledged to reflect substantial nosocomial spread. This is less likely to occur in ICU’s as most patients are cared for in individual rooms or bays.
I am grateful to the Spectator for crunching the stats on length of stay for Covid patients and discovering this has shortened substantially. For some reason SAGE and the NHS are reluctant to publish this important information, even though we know they assess it on a daily basis. Why might that be?
On the scientific front, there have been several papers published in the last few days assessing comparative data from Omicron and Delta waves. The Steve Biko Hospital in Tshwane has published a paper in the International Journal of Infectious Diseases showing a more rapid rise and decline of Omicron hospitalisations, with a peak occupancy 51% of the delta wave and markedly lower mortality, length of stay and oxygen requirement for Omicron patients.
Further South African data suggests that T cell responses, whether from vaccination or prior infection, hold up well against Omicron. Several studies in mouse models support the thesis that the spectrum of disease is milder and Omicron does not infect cells in the lower respiratory tract.
On the epidemiological front, the latest ZOE app update suggests that positive cases in the community are increasing, but the rate of increase is slowing in the 0-55 age group. On the other hand, cases in the 55-75 age group are rising more sharply. I am bemused by the recommendation that as 75% of people with ‘cold type’ symptoms are likely to have Covid, Government advice should be updated to include symptoms of sore throat, headache and runny nose as being symptoms requiring self-isolation. Being something of an old-fashioned doctor, I would be very grateful if one of the experts could explain to me why we aren’t simply reclassifying the variant as a common cold rather than treating it as a deadly pandemic, if the major symptoms of Omicron are as described?
At the time of writing, the NHS has just announced the initiation of ‘mini-Nightingales’ in hospital car parks and the like to care for patients recovering from Covid. This is certainly a much more sensible idea than trying to set up ICUs in warehouses, but is likely to run into the same obstacle – namely, lack of staff. Dr. Stephen Powis, the Medical Director of the NHS, says that the service is on a “war footing”. To the best of my knowledge, Dr. Powis has never been in a war.
The papers and airwaves are filled with commentary about NHS staff absence rates as a consequence of positive Covid tests or mandatory self- isolation from close proximity to a known patient. Again, perhaps I am being obtuse, but could one of the experts please explain to me why this problem would not immediately vanish if we simply stopped testing asymptomatic people?
Aside from data analysis, I have also been reflecting on the professional performance of the public health community over the last 12 months. I am reluctant to castigate colleagues, being all too aware how easy it is to make mistakes in clinical practice, but medicine is, by necessity, tightly regulated. Systems are in place to spot poor practice and prevent unnecessary harm to patients. These systems are imperfect, but they function reasonably well. Even when criminally minded doctors such as Harold Shipman and Ian Paterson evade detection, they only manage to harm relatively small numbers of people.
Where are the equivalent systems to regulate the decisions and actions of public health doctors? The quantifiable harms of constant lockdown advocacy have been demonstrably greater than the benefits, as has been regularly pointed out on these pages in the last 12 months. Decisions taken as a result of advice provided by SAGE have damaged far more people than a rogue clinician can do. Simply put, the cure has been worse than the disease.
I note that Professor Chris Whitty, giving evidence to the House of Commons Health and Social Care Select Committee was dismissive of criticisms around the adverse effects of lockdowns on cancer diagnosis and treatment. He described such views as being “an inversion” of the truth. I beg to differ – and I do not think I’m alone in my dissent.
Lest readers misunderstand, I am not equating SAGE with Shipman or Paterson. Nevertheless, the system of checks and balances in clinical medicine does not appear to be replicated in public health. When repeated mistakes are made by clinical doctors, prompt regulatory action follows and sanctions are imposed. When can we expect the same standards applied to the healthcare modelling community, who have been demonstrably in error so often in the last 21 months?
Finally, I ask for readers’ patience as I outline my final point of 2021. Over the Christmas period, I have been re-reading Democracy in America by Alexis de Tocqueville. Aware that not everyone shares my fascination with analytical history, some background may help. De Tocqueville travelled to America in the early 1830’s. His mission was to discover what the French could learn from the infant United States and its novel political system. The United States had recently extended the voting franchise to all white males – a radical experiment for the time.
De Toqueville writes: “On my arrival in the United States, I was surprised to find so much distinguished talent among the subjects and so little among the heads of the Government. It is a well-authenticated fact, that at the present day the most able men in the United States are very rarely placed at the head of affairs.”
A prescient analysis, which could have been written this week rather than in 1836. This fits with my belief that the skills required to get elected in a democracy are quite different from the skills needed to govern well. It is essential that our senior politicians are able to critically evaluate advice and hold ‘experts’ to account but sadly these skills are not currently manifest.
Accordingly, here is my wish for 2022. That the Daily Sceptic community resolve to get Toby Young into the House of Lords. Not just for his work on this website, but for his consistently inspirational leadership of the Free Schools movement and the Free Speech Union.
I don’t propose this audacious ambition so Toby can swank around wearing ermine, but specifically so we can put him to work (in typically forthright fashion) representing an important strand of public opinion in the seat of our legislature – providing the skillset that our elected representatives either lack or are too afraid to express. Of course, that will never happen. Or could it?











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Rep. Jim Jordan, who inquired to the former Trump administration official: “When the government told us that the vaccinated couldn’t transmit it, was that a lie or is it a guess?”
“I think it was hope that the vaccine would work in that way,” Birx replied.
https://naturalnews.com/2022-07-04-vaccine-mandates-predicated-on-hope-rather-science.html
Cut the excuse making wankers:
“Yes but ‘long-covid’”
“My granny deferred seeing her GP because she didn’t want to overwhelm the NHS”
”Tory underfunding”
What’s one more death jab sneaking onto the market? We’ll be expecting an official investigation into the excess deaths/injuries from the deployment of these gene therapies any day now, obviously…
”Bimervax, the COVID-19 vaccine developed by HIPRA Human Health, has today been authorised by the Medicines and Healthcare products Regulatory Agency (MHRA).
It becomes the 9th COVID-19 vaccine to be authorised by the UK’s independent medicines regulator.
Bimervax combines a part of the SARS-CoV-2 virus spike protein with an ‘adjuvant’ – an additional ingredient designed to trigger a stronger immune response. It can be given as a booster injection in the upper arm, to those aged 16 years and over.
The clinical evidence for this authorisation is based on data from a study of 765 adults who had received primary vaccination with 2 doses of the Comirnaty COVID-19 vaccine and who were given a booster dose of either Bimervax or Comirnaty. The vaccine demonstrated a strong immune response, and the most common side effects were mild, and self-resolved within a few days of vaccination.”
https://www.gov.uk/government/news/bimervax-covid-19-vaccine-authorised-by-mhra
Just a reminder of the now infamous June Raine’s ”..from watchdog to enabler” clip, so as we can all feel rest assured, you know?
https://twitter.com/BandyGit/status/1686685964557545472
So we are still on emergency approval, although there is no emergency? That is doublkethink of the worst kind. 1984 here we come, and it is almost complete! This is a me too response to a manufacturer from an alleged regulator that is so far as to be fit for purpose as to be criminally liable. So much for Quangos, ban the lot!
Nick, thank you for putting pandemic in inverted commas. So important.
If SAGE estimated that 75% of COVID admissions where because of COVID and not because of a positive test upon entering hospital for an unrelated reason, it’s a safe assumption that the real number was close enough to 25% (probably from below) that they had to admit something to muddy the waters. And then, there’s of course the estimated.
If records had been kept proberly, nobody would need to have estimated the number as it would have been known. This is a tacit admission that – at no point during this ‘pandemic’ – the pandemistas really knew the number of COVID hospital admission because they really didn’t even want to know them. Which – in turn – implies that the pandemic of headlines and restrictions never coincided with a mass-outbreak of a highly infective and very dangerous disease. Otherwise, it wouldn’t have been possible to turn a blind eye to reality.
The shocking bit here is how cheaply done all of these fabrications where. Eg, people listening to Ferguson despite his record of gross mispredictions on anything. If you really want know what’s going to happen in future, ask Professor Pantsdown and bank on the polar opposite happening.
Remember too that a PCR test did not show active infection, just that there might have been some contact. Remember 40 cycles is useless for diagnosis of active, 20 is more reasonable as an active infection indicator. Everything was lies from top to bottom. The figure was more likely to be 1%.
It will be interesting, if that’s the right word, to see what happens in future.
Shouldn’t we have seen a reductiion due to seasonality, dry tinder already gone and herd immunity?
It sems as though “covid” is still very prevelant and circulating widely, entirely as GVB predicted, due to the criminal folly of jabbing erstwhile fit populations with a none sterilising jab.
GVB also says it’s a myth that virus always mutate to a more benign/more transmissible state. Their apparent seasonality effect is mainly (obviously lack of warmth/sun/vitaminD3 are factors) due to herd immunity being achieved in the general population during winter exposure – which we can’t achieve due to the jab.
If he’s correct on the latter point, the jabbed world is in big trouble.
‘I confess that as time passes, I forget just how bonkers it all was. For example, in addition to our own Sages, we had Albert Bourla, Chairman and CEO of Pfizer, along with Gates, Biden, Fauci, et al., telling us throughout 2021 that vaccines stopped transmission. I’m sure, like me, you’ll still hear people say, “But they never said that vaccines would stop transmission.”’
Would you believe that a trusted expert speaking on the trusted BBC, as long ago as three days ago, is still claiming that the Covid vaccine prevents transmission?
If you find that hard to believe, listen for yourself, if you can bear it:
Dr Sarah Pitt – a “leading virologist” and “a microbiologist at the University of Brighton and fellow of the Institute of Biomedical Science” – clearly suggested on BBC Radio 5 Live on Sunday night that the vaccine prevents transmission. Talking to Stephen Nolan, 2:47:00 to 2.47:37 into the programme, here:
https://www.bbc.co.uk/sounds/play/m001p6ys
Dr Pitt said that if anyone is offered a booster vaccine:
“then they should definitely take it, because it’s much better not to get Covid, because it’s a really really nasty infection, and can have some very serious consequences for you, and you also don’t want to be passing it on to the people around you for the same reason, so definitely have the vaccine, if it’s offered to you.”
A couple of minutes earlier – at 2:45:40 – she stated that the vaccine is “very safe and very effective” and that if you “unfortunately experience quite severe side effects”, if you get to the hospital in time, you not only might be okay but you also have protection against Covid!
So that’s all good!
Anybody still proclaiming this codswallop after this long and after all the evidence that has been compiled which refutes these claims just sounds like they’re in the tight grasp of religious fervour, because it really has become more of a belief system for these cult figures now, in my opinion. They make baseless claims with nothing in the way of scientific evidence to back up their statements. They’re just saying words, basically. Pitiful really and should amount to career suicide if it weren’t for the fact we’re living in

Anybody with vaccine damage should sue her, come on lawyers, this is a good class action opportunity!
Absolutely brilliant thankyou, I needed a laugh. Good to know there is an alternative universe. I might apply to Brighton University to see if I can also pick up a clown Phd, will they accept my village idiot Bsc and my fuckwitt Msc as entrance?
Undoubtedly. You simply need to write a meaningless thesis praising every one of these “Covid experts”. You can copy their data, I’m sure they have so much supporting this!
Bourla, Fauci etc said it stopped transmission. The Pfizer study itself was never designed to test for transmission.
They cannot remeber saying this, now known as the Biden excuse!