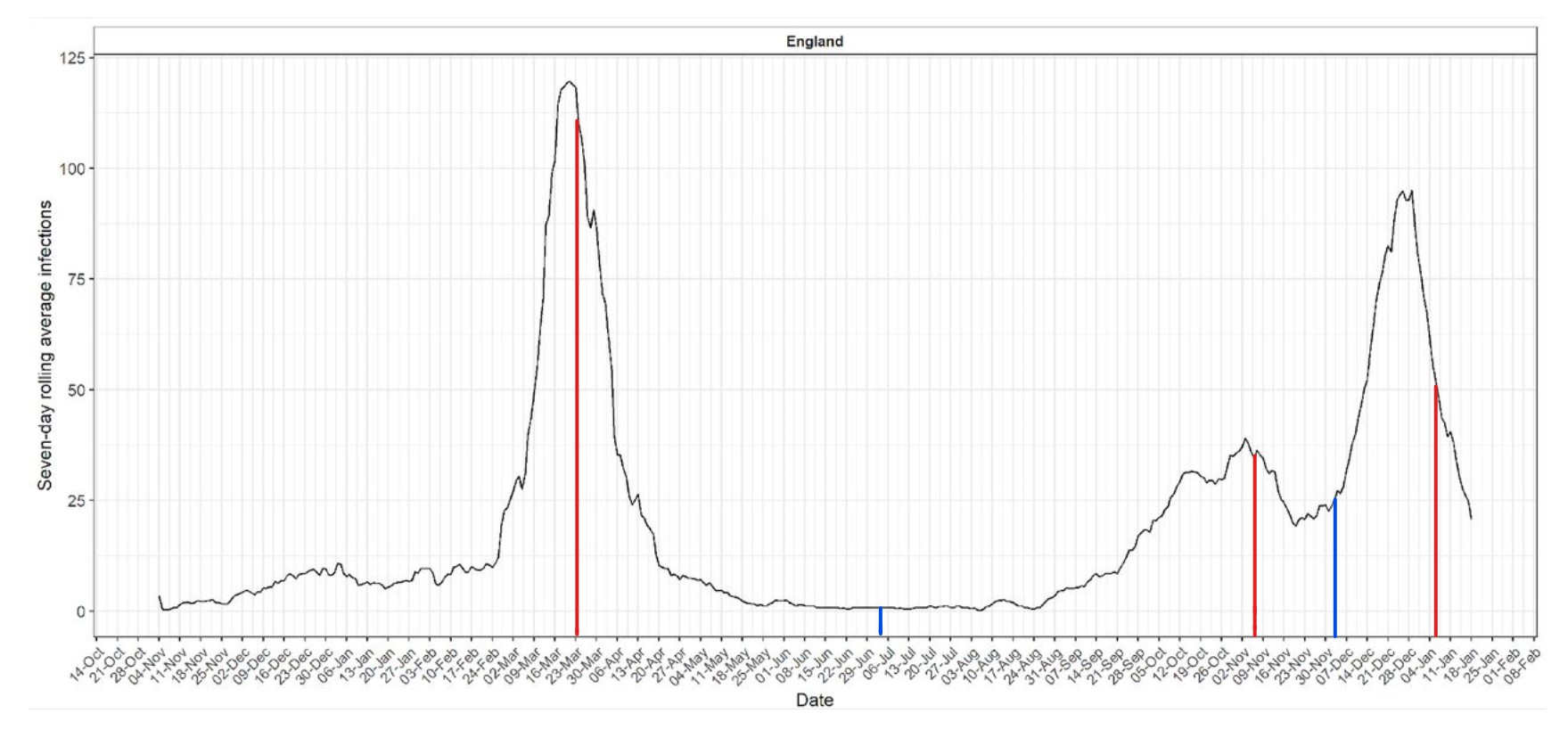
The above graph is the COVID-19 epidemic curve for England, reconstructed by Imperial College’s REACT antibody survey by asking those who tested positive in an antibody test when their symptoms began. I’ve added the start dates for lockdowns in red and the end dates in blue.
It’s a very useful graph because it does not involve any PCR tests at all, only lateral flow immunoassay tests, self-administered at home. This means it does not suffer from the problem of detecting non-infectious virus as it is not detecting virus at all but antibodies. (Its specificity is reported as 98.6%, giving it a 1.4% background false positive rate, which the researchers adjust for.) This means, for example, that the epidemic decline is much faster than in the familiar “case” curves, and the curves are more symmetrical.
What does it show? Here’s what I take from it. You might see more.
Firstly, it provides further evidence that SARS-CoV-2 was circulating at low levels in England throughout December 2019 and to some degree also in November. This fits with widespread anecdotal evidence of people falling ill with Covid symptoms in December. It doesn’t fit with the original official timeline of an outbreak beginning in Wuhan in December.
Secondly, despite circulating widely during the winter of 2019-20, SARS-CoV-2 did not undergo fast spread in England until the end of February. Indeed, the winter of 2019-20 was the least deadly on record in terms of age-adjusted mortality, despite SARS-CoV-2 being around and infecting people.
Then, around February 25th 2020, it suddenly launches into a three-week long spike of extraordinary exponential growth. This abruptly comes to an end around March 17th, and after a short plateau till around March 21st it enters just as extreme a decline. This is all ahead of the first lockdown on March 23rd of course.
The mystery is: what happened on February 25th (or thereabouts – we don’t know whether Imperial’s assumptions about the incubation period are exactly right) to cause a virus that had been circulating for at least three months at a low level suddenly to go bang and spread like wildfire? It wasn’t panic – no one was panicking at the end of February. Mobility levels were still normal until around March 12th. There was nothing unusual about the weather. Suggestions on this welcome in the comments below.
The second mystery is what caused it to stop? Not lockdown, obviously – several days too late. Social distancing? It’s a possibility, given the timing. But notice that infections also go into decline around October 19th and November 3rd, neither of which is after a lockdown (the second lockdown began on November 5th). Also, the winter surge enters steep decline around December 29th, well before the third lockdown began on January 5th. In fact, the Christmas period when people were mixing with families and experts issued dire warnings of a Christmas surge is when the infections suddenly stopped growing and began to plunge.
In every case, then, infections plateau, peak and fall before lockdowns come in, and even during times of unusually intense household interaction.
Conversely, we can also see that infections suddenly stopped falling and began rising again around November 20th, nearly two weeks before the lockdown was lifted on December 2nd. So infections fell before the lockdowns and sometimes rose during them. What’s the point of lockdown again?
One last point: this time last year infections had dropped to zero and there was no summer ripple like we’re currently experiencing. Yet it was certainly seasonality and not lockdowns causing it as there was no surge in infections during the busy “Eat Out to Help Out” summer once reopening happened in July. Presumably the Delta variant is playing a part in this, though it’s safe to say it’s highly unlikely to be as bad as SAGE is predicting.
Perhaps you have some other observations. Feel free to leave them in the comments below.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
“The motivation for all this is the reduction, if not destruction, of man’s upward mobility — and climate is the tool. This must be stopped peacefully at the ballot box.”
All together now….
Our salvation will not arrive via the ballot box.
So true 👍
Only 15 comments under this article. ——The public deserve all that is coming their way for their apathy
It looks like solar farms are good news for parascenders
When I learned to fly a glider in the ATC, we were told about the ascending air generated by barn roofs, and experienced this as a big jolt as we flew into an upcurrent. This was in Norlfolk, so plenty of barns.
Reminds me of what I used to do in a private club, years ago! Tried soaring over an old coal fired station (Didcot A) for a similar reason – plenty of hard ground inc piles of coal to be heated by the sun then, so not a bad gamble.
The cooling towers provided a lot of lift as well.
Russian democracy v Western democracy. Compare and contrast.
Russian
democracy“Orthodoxy, Autocracy, and Nationality,” v Western democracy.Plenty of contrast there.
I jumped right in and took your comment literally. Your comparison works better but I’ll make a small adjustment to mine.
Russian
democracy“Orthodoxy, Autocracy, and Nationality,” v WesterndemocracyAutocracy.There are those who say “why don’t they build solar farms in the desert, that way the done damage farm land?”
The answer is because it’s to hot!
Solar panels lose efficiency at temperatures over 25°c ,they need light not heat so siting them in a desert would be uneconomical!
Correct. It’s almost 10 years since I had a set of solar PV panels on my house roof, and it’s long been evident that efficiency deteriorates as temperature rises. The manufacturer’s figures say that the power temp coefficient is -0.38%/ °C, and on a normal hot summer day they cannot generate their maximum output. The best environment is on various satellites, where it’s nice and cold!
Environmentalism at one time was about a genuine concern for the planet. Overfishing, whaling, oil spills, smoke from coal fires and industry, the destruction of wildlife habitats eg concern for the Orang Utan due to Palm Oil production, etc etc etc. Then in 1999 something happened to change all of that. I remember working in Germany and I was supposed to be going off to Berlin in the next week, but then all of a sudden ……..down came the Berlin Wall. Communism suffered a massive defeat. People rejoiced that they no longer had to jump over this wall, in one direction only ofcourse. From Tyranny to freedom, from impoverishment to prosperity and from socialism to capitalism. No one ever jumped across in the other direction (unless they were a lunatic or related to Jeremy Corbyn) ——–Oh dear what were the communists to do now? What they did was find another vehicle for their communism and that was “The Environment”. ——-So what we have now is the hijacking of the environment for political purposes. 7 years previous to the wall coming down we had the Earth Summit United Nations Conference where population reduction and lowering of living standards were advocated to “save the environment”. Some years later we had this chilling statement from Maurice Strong who had played a big role in setting up the UN IPCC in 1998 when he said. “Isn’t it the only hope for the planet that the Industrial civilisations collapse? Isn’t it our responsibility to bring that about? ——–So here we had the birth of modern environmentalism which was no longer about the environment. It was about control of the world’s wealth and resources, and that eventually led to current climate policies like Net Zero. ———Problem—Reaction—-Solution. The solution always involves one thing. Massive government control over every aspect of our lives —–Communism.
Quite...
”The emerging ‘environmentalization’ of our civilization and the need for vigorous action in the interest of the entire global community will inevitably have multiple political consequences. Perhaps the most important of them will be a gradual change in the status of the United Nations. Inevitably, it must assume some aspects of a world government.”
Mikhail Gorbachev
“The concept of national sovereignty has been immutable, indeed a sacred principle of international relations. It is a principle which will yield only slowly and reluctantly to the new imperatives of global environmental cooperation.”
UN’s Commission on Global Governance
“I envisage the principles of the Earth Charter to be a new form of the ten commandments. They lay the foundation for a sustainable global earth community.”
Mikhail Gorbachev
“Nature is my god. To me, nature is sacred; trees are my temples and forests are my cathedrals”
Mikhail Gorbachev
“A reasonable estimate for an industrialized world society at the present North American material standard of living would be 1 billion. At the more frugal European standard of living, 2 to 3 billion would be possible”
UN Commission on Global Biodiversity
“Now it is the least developed world who are not responsible for this climate change phenomenon that bore the brunt of climate change consequences so it is morally and politically correct that the developed world who made this climate change be responsible by providing financial support and technological support to these people.”
Ban Ki-Moon UN Secretary General
“A deal must include an equitable global governance structure. All countries must have a voice in how resources are deployed and managed.”
Ban Ki-Moon UN Secretary General
“For the first time, humanity is instituting a genuine instrument [Kyoto Protocol] of global governance,’…”By acting together, by building this unprecedented instrument, the first component of an authentic global governance, we are working for dialogue and peace.” Jacques Chirac
“Overconsumption and overpopulation underlie every environmental problem we face today.”
Jacques Cousteau
“In order to stabilize world population, we must eliminate 350,000 per day”
Jacques Cousteau
No wonder this scam is being imposed on us when all I have is 16 thumbs up and all you have is 1 thumbs up for your fantastic comment. ———-The public deserve all the impoverishment coming their way for their apathy. If they think things are bad now just wait until Net Zero really gets going and starts to drag their living standards right downhill.
Why is Obama dropping in on Sunak? Obama is no longer in politics, officially, Sunak was not in office when Obama was President so why is he here and what is he doing? Giving Sunak his orders?
How is it that Canada, France, Ireland and Germany are introducing the most extreme
tyrannical lockstep shut down of free speech, is Pfizer and Big Phama paying these Government leaders?
How again in Lockstep is Euthanasia being pushed in these countries and ours?
plus of course America
What is going on? Do they think we don’t notice or is it the reality that the world Government a fusion between Governments, the WEF and corporations such as Big Pharma, BigTech and Blackstone just couldn’t give a damn because they now control everytthing.
Is Obama the puppeteer steering Biden?
I think/hope WEF, Big Pharma, BigTech and Blackstone, are only successful in the west.
For the first time I heard an advocate for the Net Zero lunacy, in addition to claiming the climate change justification, add a comment that switching to so-called renewable electricity generation would mean we wouldn’t have to rely on despotic regimes (he mentioned Putin) for energy.
It reminded me of an article I read in the DT shortly after 9/11 ….. which said the USA would have to wean itself off middle eastern oil ….. and presumably that meant so would the UK, the rest of the 5 Eyes and NATO.
One of the reasons for the lunacy is certainly a wish to stop funding despotic regimes by buying their oil and gas.