
Throughout the pandemic, commentators have relied on ‘COVID-19 deaths per million people’ as a measure of the disease’s lethality. While this is not unreasonable for making comparisons within Europe, it is less justifiable for other parts of the world, where there has been substantial underreporting of COVID-19 deaths.
A better measure to use is excess mortality, i.e., the number of deaths in excess of what you’d expect based on previous years. This measure does not vary with factors like testing infrastructure or the criteria for assigning cause of death. (Though the best measure is age-adjusted excess mortality.)
In an unpublished study, the researchers Ariel Karlinsky and Dmitry Kobak have compiled all the available data on excess mortality. Their database – which they’ve termed the ‘World Mortality Dataset’ – allows us to make more meaningful comparisons across countries.
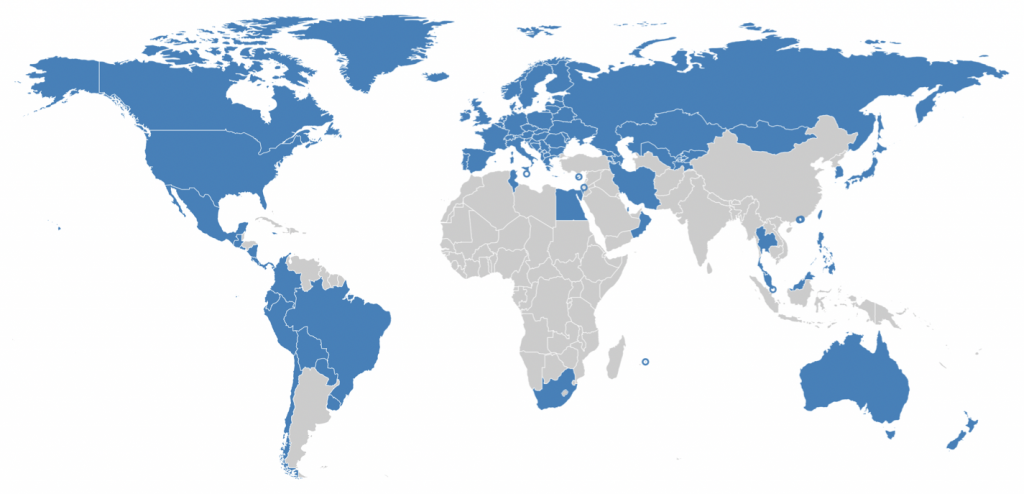
Unfortunately, data are not yet available for most of the countries in Sub-Saharan Africa, Asia and the Middle East. However, the database does encompass Europe, much of Central Asia and the Americas, and parts of East Asia. Countries with available data are shown in blue in the map below:
Note that Karlinsky and Kobak did not take the usual approach of using the average of the last five years as the baseline. Rather, they took the superior approach of using a linear trend over the last five years. If deaths have been increasing year-on-year, their approach will yield a higher baseline, compared to using the five-year average. (See here for a visual explanation.)
The authors’ results are shown in the chart below. Note that red shading corresponds to excess mortality in 2020; purple shading corresponds to excess mortality in 2021; and the % value in the lower right-hand corner of each plot is the percentage excess mortality.

There are some clear patterns in the results. Countries in Latin America have by far the highest levels of excess mortality. Six of the top seven are in Latin America; and the fifth – San Marino – is a very small country, so it’s high level of excess morality may be partly due to chance.
Central Asian countries and South Africa have the next highest levels of excess mortality. (The authors subtracted deaths in the recent war between Azerbaijan and Armenia from those two countries’ figures.)
European countries, Middle Eastern countries and the United States have the next highest levels. Finally, geographically peripheral countries and East Asian countries have the lowest levels – close to zero in most cases. Germany has somewhat lower excess mortality than you’d expect, given its size and connectedness.
Two Latin American countries – Paraguay and Uruguay – appear among those that have zero excess mortality. However, the data for these two countries stops before the beginning of 2021, when both experienced a rise in COVID-19 deaths (a dramatic rise in the case of Uruguay). It’s therefore likely they would be somewhat closer to the top if the latest data were available.
Particularly notable is that every country in East and South East Asia has zero excess mortality. (Though bear in mind that several haven’t yet reported data for 2021.) All the others with zero excess mortality are either islands (e.g., Jamaica, Mauritius) or otherwise geographically peripheral (e.g., Norway, Finland).
To what extent has policy shaped these clear regional disparities? With the exception of border controls in geographically peripheral countries, it’s difficult to see how it could have been a major contributor. Indeed, there is substantial overlap between the strictness of lockdown measures in different regions of the world.
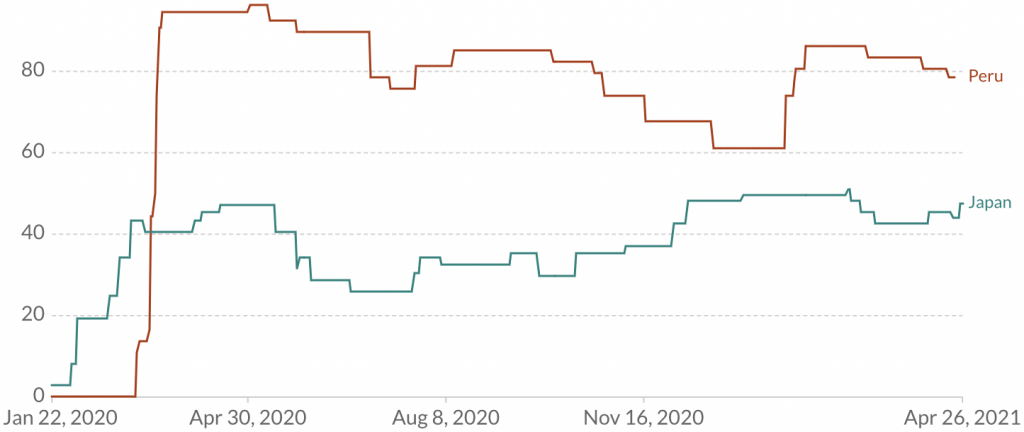
As I’ve noted before, Japan saw a minor epidemic last winter, but it retreated without any real lockdown measures being imposed. On the other hand, Peru went into lockdown on March 16th, but has seen the highest level of excess morality in the world. In fact, Japan has consistently had a low score on the Blavatnik School’s Stringency Index, whereas Peru has consistently had a high score, as shown in the chart below:
Overall, there is strong regional clustering of excess mortality: the level is high in Latin America, moderate in Europe, and low in East Asia. Unsurprisingly, it is also low in island nations like Jamaica and Mauritius, which leveraged their geographic isolation to prevent the virus getting a foothold.
This pattern of results suggests that geography is more important than policy (i.e., lockdowns) in explaining variation in COVID-19’s lethality across countries. Which exact geographic factors are involved is not yet clear, though the level of prior immunity is one obvious candidate.










To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.