
There is now lots of evidence that the coronavirus had begun spreading undetected all over the world by autumn 2019 at the latest. This has led to a mystery as to why winter 2019-20 was relatively mild in terms of ‘flu’ deaths and why excess deaths only started appearing from January onwards, first in Wuhan, then Lombardy and Iran, then other places such as New York and London.
This has led some scientists to dismiss all evidence of early spread as false positives, and conversely some sceptics who accept early spread to argue that the excess deaths of the pandemic have all been caused by interventions, not by the virus.
For myself, I don’t see how interventions can explain all the excess deaths. If that were the case we should see a positive correlation between interventions and deaths, but we don’t. Rather, as we know, evidence-based studies show there to be little or no relationship between lockdown strictness and deaths, either positive or negative.
The reality is, there are a number of mysteries about the behaviour of the virus at different times and places, the lack of excess deaths prior to 2020 being just one. Consider: there was a relatively deadly outbreak in Wuhan in December 2019, but no deadly outbreak elsewhere in China or the rest of South East Asia. Then in February and March there was a more deadly outbreak in Lombardy, but not so much elsewhere in Italy, and in New York and the north east of the U.S. but not so much in the rest of the country. Western Europe had some hotspots in spring 2020 but central and Eastern Europe saw very little. Then some other places had a strong summer wave in 2020, but not so much India, which was only strongly affected by Delta in 2021. South East Asia, on the other hand, went largely unscathed until Omicron. These patterns have not yet been adequately explained, and nor have the reasons that each (pre-Omicron) Covid wave (like flu) typically only infected 5-15% of the population before dying away, irrespective of what measures were in place.
My current best hypothesis to explain the oddly variable behaviour of the virus is that it is to do with virus variants and human immune systems and some under-appreciated aspect of how they interact. Why more deadly variants started appearing from December 2019, however, I do not know. Nor am I sure why the first deadly outbreak was in the same place that the virus may have originally escaped from, in milder form, some months before.
What I have put together, though, is a graph of Covid deaths up to May 31st 2020 for each U.S. state, plotted against the state’s distance (in miles) from New York City. This provides a powerful illustration of how strong the relationship between proximity to New York and Covid deaths in that first wave was (note the logarithmic scale).
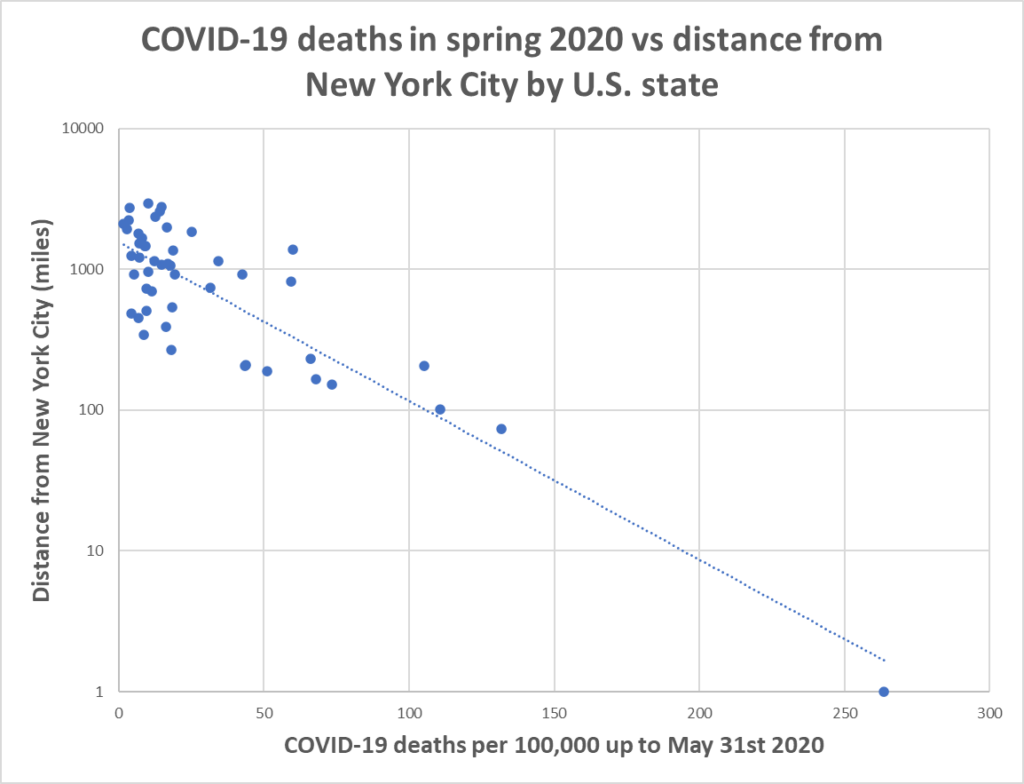
Looking at this, it’s little exaggeration to say that proximity to New York City was the key determinant in spring 2020 of a poor outcome, rather than anything else such as lockdown stringency or timing. This seems to me strong evidence that what was driving this pattern was the variant at large in New York, and how much of it was in your state.
An extra piece of evidence, then, that the answer to some of the coronavirus mysteries lies in the virus’s changing genetic make-up.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Well ok, but if the variant spread out from New York then that would mean that travel restrictions would help slow the spread of the virus. But we know that such restrictions did nothing.
I have no idea how to explain what we are seeing here, or appear to be seeing here, except to suggest that the data is hopelessly incomplete and even misleading.
There’s far more to viral outbreak, spread and virulence than is dreamt of in your philosophy Horatio.
The problem with any analysis is it must rely on data produced by Governments or their agents which is wholly untrustworthy due to its deliberate corruption and manipulation and sheer incompetence.
There can be no meaningful analysis beyond we were deliberately misled and panicked by evil people for political, ideological and monetary motives.
I think that’s it. Gathering such data comprehensively, or at least sufficiently, to conduct useful analysis and draw useful conclusions would be extremely difficult with the best will in the world. But when governments, health agencies, and the like have deliberately corrupted and obfuscated the data then the task of analysis becomes almost hopeless.
My hunch is that Will is drawing ostensibly sensible conclusions from data which is probably hopeless, and hence not much relevance can be placed on those conclusions.
Happy to be shown to be wrong, but my feeling is that these conclusions can be regarded as only loose conjecture right now.
Australia and NZ had a more severe than normal winter (June to August) ‘flu season in 2019.
Was this not in fact Covid?
https://theconversation.com/its-a-bad-year-for-flu-but-its-too-early-to-call-it-the-worst-ever-5-charts-on-the-2019-season-so-far-120093
All-cause mortality, please! We need to stop referring to so-called ‘covid deaths’ as if there has been some definitive and reliable measure of this. And remember that some locations may test more than others.
Well sure. Given how the lurgy was “detected” with tests that amplified a genetic sequence far beyond what the inventor K Mullis intended (CTs of well above 30+, let alone its ability to differentiate live viral fragments from dead ones), how many afflicted were essentially at their end of life anyway (not including the Liverpool Care Pathway that was potentially used to accelerate those, and perhaps much younger others at that), the fact the average age-of-death due to the lurgy appears to be HIGHER than our average life-expectancy (something clearly doesn’t add up there if the lurgy increased our life-expectancy on the whole) and.. an mRNA “solution” that has arguably been the most dangerous intervention ever administered on the public (with no definitive evidence of its efficacy or safety other than the Yellow Card data which no one seems even the slightest bit concerned over, anecdotal hogwash of how awesome the potion is outside of the pharmaceutical’s own questionable declarations (PHE / HSA’s data clearly showed for months on end after its launch the recipients of the gene-therapy solution were testing positive up to three times as much as those ‘un-solutioned’, prolonging the pandemic by infecting others at a rate above R1).
All combined shows “the data” is useless – more than useless since it’s guided policies that themselves have caused untold disaster (some still to be realised in many years to come). Leaving us with only one metric that could be beneficial as you point out – all-cause mortality to give us an indication of how a complete and utter shitshow this really was / is.
Interesting that the data source used by Will shows the NY curve completely out of synchronisation with the five other locations depicted, which appeared to progress in lock step. And this graph also emphasises how different were NY’s results.
Of course, one reason for New York to be so different from the rest of the country is that the NY authorities simply made up the results, but surely nobody would do that, would they?
Could there have been a second leak in Wuhan, of a different variant?
Maybe the 1st release wasn’t doing the job, maybe the 2nd release was accompanied with a dodgy PCR test knocked up in a couple of weeks to big up the numbers. Maybe Omicron was released to cover up the shoddy vax and to show how effective they are at preventing death.
Remdesivir, Midazolam ventilators all helped with the numbers and the authorities deliberately muddying the statistics. Who actually knows?
In the UK we saw only saw deaths start to spike in the ‘care’ homes once they shut down the hospitals and started giving out Midazolam. That would be my investigative starting point.
There’s no mystery. It simply wasn’t killing enough people for anyone to notice.
Nor producing symptoms not shared by umpteen disease causing respiratory viruses that are routine part of life.
Another outstanding effort by Will Jones, for which many thanks.
Of course the main thing that New York, Wuhan and Lombardy all have in common is very poor air quality.
The other thing in common everywhere is very poor data regarding cause of death and covid/influenza diagnosis, distinction.
Nevertheless:
‘….the present study demonstrates that higher rates of spread of COVID-19 in Metropolitan Lima (Peru) are associated with previous long-term PM2.5 exposure. Men and older people were at higher risk of death due to COVID-19. Reduction in air pollution from a long-term perspective and social distancing are needed to prevent the spread of virus outbreaks.’
‘Association between air pollution in Lima and the high incidence of COVID-19: findings from a post hoc analysis’ 16 June 21 BMC Public Health
The key appears to be previous long term exposure to pollution with, no doubt, consequent previous respiratory infections.
The obvious solution would seem to be bicycles but these seem to engender frequent psychotic episodes in their users.
Since March 2020 I’ve suspected that air quality plays a major role in covid mortality. Back then I use to joke that it wouldn’t bother us down here in Devon and Cornwall, as the virus didn’t like the sea air. Except that I wasn’t really joking.
Completely agree. The reason that so many of us on here have been so incandescent for so long is that all of this is so obvious.
Up north, it hasn’t bothered us much either, except in the cities!
This is not complicated, has been going on since the ‘smogs’ in major cities in this country.
The common cold, coronavirus or other, is a major killer of the elderly and infirm, even more so than influenza, well documented.
Only the World Health Organisation and its acolytes, for reasons doubtless not unconnected with venality, could have instrumented this monstrous debacle.
Just as we can no longer be beholden to the global energy market, we must sever all links with this plethora of undemocratic supranational entities, WHO, OECD, ECHR, World Bank etc. who very much do not have our best interests (but their own) at heart.
My first thought after reading this was: orchestrated biological attack.
It is becoming pretty clear that Covid 19 started Oct 2019 or earlier but the panic only started when it reached high density centres of population with poor air quality, populations, many of whom had already had or still had respiratory infections which made them particularly susceptible to a novel common cold coronavirus, Covid 19.
The situation was further confused by simultaneous outbreaks of influenza and covid 19
‘The spread of COVID-19 in Wuhan and Seattle was far more extensive than initially reported. The virus likely spread for months in Wuhan before the lockdown.’
Using the COVID-19 to influenza ratio to estimate early pandemic spread in Wuhan, China and Seattle, US. The Lancet, 12 Aug 20
‘So the 20,000 cases in China is probably only the severe cases; the folks that actually went to the hospital and got tested. The Chinese healthcare system is very overwhelmed with all the tests going through. So my thinking is this is actually not as severe a disease as is being suggested.’ ‘There’s a vast underreporting of cases in China.’
Prof John Nichols Univ. of Hong Kong 06 Feb 20
Lima, also Iquitos, Peru are other examples of how poor air quality, a cause of respiratory infections for some years, created a population of the elderly and infirm particularly susceptible to Covid 19.
Interestingly I had to retire to my bed for several days in November 2019 with the then classic symptoms of Covid-19, especially the protracted dry cough. I was completely washed out. It could of course have been flu (though I had been jabbed a couple of months earlier) but it was unlike any previous bout of flu I can remember. I didn’t trouble my GP and fully recovered after a couple of weeks
I have come across a few other people with the same story…. curious.
It’s no mystery. Why did it spread undetected? Because nobody was looking. Had we not been told there was a ‘novel’ virus causing what we normally call Cold or ‘Flu, with all the unnecessary ensuing panic, we still wouldn’t know about CoVid 19.
How much do we currently know about the spread of rhinovirus and adenovirus? There is no daily escalating count of positive PCR tests for these, but they surely are spreading as they have been doing for some time.
Completely agree and these can, of course, be every bit as lethal amongst the elderly and infirm as the novel common cold coronavirus, covid 19, as this paper, well before Covid, explained:
‘Unexpectedly Higher Morbidity and Mortality of Hospitalized Elderly Patients Associated with Rhinovirus Compared with Influenza Virus Respiratory Tract Infection’ Apr 2017
The Prime Minister and Health Secretary both deserved to lose their jobs many times over for multiple grave derelictions of duty. Beyond time for the Gumby Brothers Whitty and Vallance to lose theirs.
Beyond time for the Gumby Brothers Whitty and Vallance TO FACE CRIMINAL INVESTIGATION.
It might be critical to look at treatment of Covid patients in hospitals and care homes, including use of sedatives and ventilators, if only to rule this out as a factor explaining the Spring 2020 surge in excess deaths.
Though the ONS buried historical mortality statistics in a dusty corner of their website (instead only ever choosing to publicly present five years’ of data), they were obtained via FOI, and are still available.
They show that absolute mortality in 2020 was no higher than ~2003. Age adjusted, the date moves forward several years. What made 2020 seem so unusual was that all cause mortality had decreased substantially from the early 2000’s onwards.
You can speculate as to why. Most likely a generation moving into old age who were more switched on to their health – reduction in smoking; better diets; better healthcare; better diagnosis with the aid of smarter technology, particularly of cancer and heart problems.
Health isn’t binary between good and bad though – there’s a continuum, and it’s likely these improvements left a large number of people who would have died of other causes in previous times, more vulnerable to death from viral infection.
It would have also left a section of the population less likely to survive aggressive and inappropriate medical intervention. The damage caused by this intervention could be hidden during an outbreak of a fairly nasty flu-like respiratory illness. Some have suggested governments used the pandemic to implement mass state-mandated euthanasia. This is a shame as it poisons the well, making it easy to dismiss legitimate worries surrounding this as conspiracy theorising. There’s no way such a programme could remain hidden.
There is however the possibility – and one that the healthcare sector might be understandably reluctant to acknowledge – that the surge of excess deaths was caused (or exacerbated) by a combination of panic and institutional errors resulting from the sort of groupthink that thrives in a crisis. That in a healthcare system riven with fear of being overwhelmed, of infection of its staff, and of fear of catastrophe enhanced by government and media hype, many already vulnerable Covid patients with pneumonia were pushed over the edge by interventions rather than the virus itself. That without these interventions, the excess death figures might resemble those of a flu outbreak. There’s also the possibility that this skewing of the data makes it harder to determine the true cause of later excess mortality.
Doctors, nurses and paramedics were inculcated with the idea that Covid infection in the vulnerable was a downhill path to a painful and protracted death; that due to irreparable damage to lung tissue, there was little chance of recovery beyond use of ventilators, failing which powerful sedatives should be used to ease anxiety and discomfort prior to death. It’s established that invasive ventilation causes lung damage. Ventilator associated pneumonia was also later shown to be higher in Covid patients than in non-Covid patients. Its also established that sedatives like Midazolam and Morphine cause respiratory suppression and distress, which for an elderly patient with pneumonia is likely fatal. These factors would have fed into the Covid mortality data, circularly heightening the perceived mortality risk of the virus and further justifying use of these interventions.
Regarding sedatives, it’s also known that the previously banned Liverpool Care Pathway was resurrected at this time. The Covid ‘end of life’ guidelines published by Public Health Scotland and the Birmingham NHS trust (which I found after a couple of minutes googling) recommend administering sedatives in Covid patients to ease anxiety and distress, in doses that according to CDC guidelines for their use act as anaesthetic, and in elderly people would often lead to death. Moreover with no clinical basis required for their administration in settings like nursing homes or adequate monitoring that the guidelines insist upon.
It’s not hard to see how such a policy could be disastrous. While a compassionate medic might understandably want to ease the suffering of a patient near death, and even hasten their passing, how, in the absence of clinical evidence, could they know that death is inevitable? Especially when the effects of the drugs they’re administering are indistinguishable from acute respiratory distress syndrome? Anxiety is a subjective measure – any Covid patient admitted to hospital was likely to be in a state of extreme anxiety and have breathing difficulty from at least mild pneumonia.
There’s a possibility that medical interventions might have acted at least as a multiplier for patients with Covid symptoms in excess death data, which could help explain the unusual bumps and age discrepancies. This needs serious investigation, but I’m not holding my breath..
The ‘surge’ in mortality spring 2020 was a simple product of hospital clearances.
The Amnesty International report “As If Expendable’ gives chapter and verse.
The rest of the year, age adjusted, was pretty much plumb normal and not much out of the ordinary since then.
This view chimes with what I’ve said. As far as I know, the NHS end of life guidelines would have applied to treatment in care homes as well as hospitals. In the former there would have been even less (if any) examination of clinical evidence justifying administration of sedatives and less medical expertise. Proper analysis of their administration in these settings would help clear it up, but the whole thing seems to have been swept under the rug.
Insightful post, methinks.
Government-reported COVID death numbers are completely useless as there’s no single definition of COVID death and the usual definitions are only insofar related to COVID as they’re based on a positive PCR test result some time before death.
Worth recapitulating here: According to lots of anecdotical evidence, the so-called Spanish flu was the most horrible killer disease since the black death. The German official history of WWI by the Reichsarchiv (Der Weltkrieg von 1914-1918) mentions hundredthousands of sick German soldiers (all malnourished and living in poor and very cramped accomodations, out of somewhat less than 5.5 million soldiers in the German field army) who will typically again be fit for service after 4 – 5 days and will have completely recovered within a few weeks. Which means this horrible pandemic was pretty much not more than a severe outburst of pandemic hysteria in the USA.
Even the most ardent COVID zealots freely admit that COVID is much less deadly than the Spanish flu. Considering the information from the source mentioned above, this means that COVID was, relative to a non-event, an even ‘noner’ event. Someone should really classify the WHO and everything associated with it as instrument of senseless mass devastation rivalling to the most deadly weapons invented by mankind so far.
I expect this has already been cited, but aren’t the axis labels reversed on the chart?
That’s what I thought?
A Chinese scientist charged with investigating the outbreak defected to the US and went on GB News where she claimed the release of the virus was deliberate. If that was the case, it might have been released in several locations before it took hold, possibly with different variants, while also escaping from the Wuhan lab. Omicron’s mysterious appearance in South Africa is a good example. And no, I’m not being a conspiracy theorist: just speculating. As for me, I had it at Christmas 2019 and was wiped out for weeks by it. Very unpleasant. It was all over my home town.
“Consider: there was a relatively deadly outbreak in Wuhan in December 2019”
Was there? I don’t believe a single word of it.
Are your axes mislabelled?