
Now that the vaccinated are dying with Covid at a rate similar to the unvaccinated (probably because almost everyone has now been infected, so the vaccinated no longer gain much advantage from their vaccination) we can make an estimate as to how many lives the vaccines may have saved and so make a risk-benefit comparison with how many may have died from vaccine injury.
A recent study in the Lancet claimed that in the U.K. Covid vaccines saved between 395,000 and 1.1 million lives up to the end of 2021. But this estimate makes no sense. Up to the end of 2021 the official Covid death toll stood at 149,000, of which 74,000 occurred in 2020 before the vaccines were rolled out, and 127,000 occurred before March 2021, when few were fully vaccinated. Some might claim the winter 2020-21 wave would have been worse but for the vaccines, but in fact the U.K.’s winter wave was no better than in other countries where vaccination occurred later. It stretches credulity to breaking point to suppose that on top of the 22,000-75,000 Covid deaths post-vaccine rollout (depending when you start the clock) there were between 395,000 and 1.1 million deaths that were averted, particularly when in the prior 12 months without vaccines there were only between 74,000 and 127,000 Covid deaths.
Between the vaccine rollout and the end of 2021 there was one just main wave of Covid deaths: the Delta wave, during which around 22,000 U.K. Covid deaths were recorded. How many more would have died without the vaccines in this wave?
Using the deaths data from the UKHSA for September 2021 and the infection rate data from the ONS we can calculate an estimate of the infection fatality rate among the unvaccinated during the Delta wave. This gives: 0.1% for those in their 40s, 0.7% for those in their 50s, 1.3% for those in their 60s, 4.3% for those in their 70s and 11.1% for those over 80. This assumes that the ONS doesn’t overestimate infections (if it does, the IFR should be proportionally increased) and the UKHSA doesn’t overestimate deaths (if it does, the IFR should be proportionally decreased; note that during the Delta wave ONS figures showed deaths due to Covid were about 85% of those with Covid). It also assumes that the infection rate in the vaccinated and unvaccinated is about the same, which the UKHSA data from the time suggest was indeed the case (it was higher in the vaccinated later in the Delta wave but lower earlier on).
These estimates of the IFR for the unvaccinated during Delta are very close to those found in a study from December 2020, which for the original waves in Europe and the U.S. found an IFR of 0.4% for 55 year-olds, 1.4% for 65 year-olds, 4.6% for 75 year-olds and 15% for 85 year-olds. This suggests our estimates may be about right. (If they are right it also suggests Delta was not any more deadly than earlier variants, contrary to claims often made about it.)
What about the IFR for the vaccinated during the Delta wave? Using the same UKHSA and ONS data (and making the same assumptions), these are 0.02% for those in their 40s, 0.12% for those in their 50s, 0.34% for those in their 60s, 1.2% for those in their 70s and 3.9% for those over 80. This is using figures from September for all vaccinated with at least one dose.
By dividing the IFR in the vaccinated by the IFR in the unvaccinated we can get an estimate of real-world vaccine effectiveness against death during the Delta wave, which is 79% for those in their 40s, 83% for those in their 50s, 74% for those in their 60s, 72% for those in their 70s and 65% for those over 80. These figures are summarised in the table below.
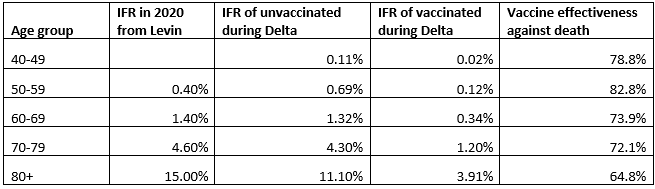
Since the majority of Covid deaths are in those over 80 and 98% are in those over 60, we will summarise these data as reducing deaths by about 67% in the vaccinated. In September 2021 around 8% of those over 60 were vaccinated and 92% were unvaccinated. From this we can calculate (22,000/[0.08+0.92*0.33]) that without vaccines there would have been around 57,000 Covid deaths during the Delta wave, meaning the vaccines saved around 35,000 lives during the Delta wave. So not 395,000-1.1 million, but 11-31 times less than that.
To this total we should add those saved during the initial Omicron waves, before near-universal natural immunity rendered the vaccines largely obsolete. Around 17,000 died with Covid between January and March 2022, but with Omicron around 40% are deaths with-but-not-of Covid, so this figure should be more like 10,000. UKHSA data from the time indicated the vaccines started January about 80% effective against death but declined towards 50% as spring approached. If we assume that overall they reduced deaths in the vaccinated by around 70%, and with 95% now vaccinated, we can calculate (10,000/[0.05+0.95*0.3]) there would have been around 30,000 deaths without vaccines, meaning they saved around 20,000 during the early Omicron waves, giving a grand total of 55,000 lives saved.
What about the other side of ledger – how many were fatally injured by the vaccine programme? Dr. Theo Schetters in the Netherlands has estimated that the vaccine fatality rate may be around one in 800 in the over-60s, a figure that is similar to those obtained from analysis of the U.K. and Denmark. In the U.K. around 50 million doses have been delivered to over-60s, which gives around 62,500 deaths. This is slightly higher than the number estimated to have been saved.
Some of these estimates and assumptions may be a little off in either direction, so not too much weight should be put on the exact figures. The important point is that the number of lives estimated to be saved by the vaccines is around the same as the number estimated to be lost to them or slightly lower – a conclusion which is consistent with the findings of Professor Christine Stabell-Benn, who analysed the all-cause death data from the mRNA vaccine trials and found a similar number of deaths in the vaccine and control arms.
We should also note that the longer term impact of the vaccines is still unknown.
It is looking very much like the vaccine programme failed to save any lives overall and was a very costly mistake.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
What are the all-cause mortality rate statistics pre and post the covid “vaccine” rollout?
In the USA at least, significantly worse after the rollout compared with before.
I think in the UK too. It would be instructive to compare the rate of all-cause mortality between the vaxxed and the unvaxxed, though of course there might be selection factors that skew the results (e.g. maybe the unvaxxed are more likely to look after their health generally).
Why should the unvaccinated be more likely to look after their health? If those who were vaccinated were concerned that they might contract a serious illness then that appears to suggest that they are more likely to look after their health. In fact I would suggest that that is a red herring.
You cannot conclude that all-cause excess mortality is due to the vaccines. There is no breakdown of individual causes. Then the possible mechanism by which the vaccine could be the cause.
If you read what I wrote I said “maybe” – in my anecdotal experience and from reading the posts here and on other sceptic forums, a lot of sceptics are health conscious, try to eat well, not be stressed, get exercise. But it’s hard to know for sure and all I was doing was giving an example of things that might make the comparison less valid.
Nowhere did I say that all-cause excess mortality is due to the “vaccines”, but one way to see if it’s an avenue worth investigating is to look at all-cause mortality rates split by vaxx status, and see whether they diverge significantly and how they have changed since the vaxx rollout. It’s about looking for strong signals among all the noise so there are some likely avenues that can be looked into properly – but this will not happen because the interests at play in stopping this are huge and likely impossible to overcome.
But that is the problem, in some peoples minds the excess deaths are due to the vaccine, some may be, it would be difficult to show a causal link without a full forensic autopsy with a genetic analysis.
https://pubmed.ncbi.nlm.nih.gov/33896121/
https://www.frontiersin.org/articles/10.3389/fimmu.2021.641900/full
In asking if increases in Excess Deaths are linked to the vaccine rollout you might find the attached useful …
https://youtu.be/kFf5k2h-f_4
John, if there were a large spate of mysterious spontaneous fires in newly built houses and apartments that were killing hundreds of people but they didn’t know why. Then it was revealed that a brand new type of consumer unit was being used – let’s say made in China – that had managed to bypass British safety standards, been rushed to market and not undergone adequate safety tests, by any measure of sanity this would be the first place forensic fire officers, police and trading standards would look and this would absolutely be plastered wall to wall all over the papers.
In Covid jab terms, as it stands these fire officers and the media’s position is;
“We’re not going to investigate these consumer units because there’s no evidence that these consumer units caused these fires so we’re not going to investigate.”
The most bonkers and frightening circular argument in history and one that shows either catastrophic symptoms of mass formation psychosis or catastrophic symptoms of corruption and evil.
I’m not saying that there shouldn’t be an investigation, of course there should but it must be blinded in that there are no preconceptions. The first part would be to account where the discrepancies are. The second part would be stratify the data based on age, ethnicity, Co morbidities and geographical location.
Although the current dataset covers a decade, it wouldn’t be unreasonable to look at excess deaths in previous decades, such as the 1990’s and 2000’s.
It may be worth looking at excess deaths in 1976 and 2003.
https://pubmed.ncbi.nlm.nih.gov/15804164/ suggests that the number of excess deaths in 2003 was 2091 (17%), other sources suggest 16%.
According to Wikipedia the excess death rate in 1976 was 20%.
The winter of 2017-18 had 50,000 excess deaths the highest since the winter of 1975-76.
Brilliant analogy
It’s not a question of how many lives the “vaccine” did end, the important question is how many lives the vaccine is GOING to end, and also how many life changing auto immune diseases they have caused and will continue to cause.
The gene therapies – for that is what they truly are – can only work by dysregulating the immune system. The consequences cannot be benign.
Basically, genetic engineers know the square root of F*** all about the effects of their products on the immune system but have been encouraged to carry on regardless..
It is beyond all parameters of incompetence and evil.
Indeed
Long term safety trials are not yet completed, but have been irrevocably compromised as there is no longer a control group
Indeed, if you got jabbed, you ARE the long term safety trials.
Oh well. Those who got jabbed made their choice, did their risk – benefit analysis. They’ll find out soon enough how it’s turned out.
Personally I’m feeling quite happy with my decision not be jabbed, in spite of the limitations it imposes on me and the small indignities I’ve had to endure.
Those who got jabbed didn’t do a proper risk-benefit analysis because they were constantly bombarded with propaganda telling them the vaccines were safe, it was their duty to society to have the jab, they faced an exagerated risk from covid etc. Therefore if they suffer injury/death from the vaccines they don’t just have themselves to blame, everyone from the government, MSM, celebrities etc. who nudged them to take the vaccine are responsible for any harm the vaccinated come to.
Their problem, not mine. I wasn’t nudged.
And many of the jabbed were nudgers themselves.
I agree in that adults should be treated as adults and stand or fall by their own decisions, but I don’t think taxpayers money should be spent on advertising, especially not on advertising products where the profits don’t go back to the taxpayer.
Encouragingly many people we know who did get a couple of Covid jabs are now regretting it and will not have another.
They are not gene therapy as they do not alter anyones DNA, not even the AstraZeneca version despite it needing the nucleus to start the replication process by creating mRNA.
All replication takes place away from the nucleus in organelles such as the rough endoplasmic reticulum, the Golgi apparatus and ribosomes in the cytoplasm.
Being genetically engineered does not equate to being genetically altering.
SARS-CoV-2 itself dysregulates the immune system as do a lot of pathogens, there are viruses that mimic certain proteins that are recognised as “self” and thus escape the immune system.
See https://www.ijbs.com/v17p1547.pdf
https://repository.um.edu.mo/bitstream/10692/102855/1/SARS-CoV-2%20%26%20the%20Nucleus.pdf
Sorry I call BS. We already have evidence of these MRNA injections reverse transcriptasing on Liver cells. Bid only knows what they will do to human gametes as we do know the LNPs have an awful tendency to go to ovaries, lymph nodes snd bone marrow.
The cell line used in that experiment were eternal cancer cells, whose DNA was abnormal and there was a transcriptase that is not found in healthy cells. Watch https://www.youtube.com/watch?v=bsF82gg9vMs
and this https://www.youtube.com/watch?v=UAibZnGbxRQ&t=33s
Please provide a reference or two regarding the LNPs
You can start with this https://expose-news.com/2022/04/29/pfizer-study-mrna-vaccines-suspended/
I’ll check your vids tomorrow.
https://dan-peer.tau.ac.il/wp-content/uploads/2021/04/Manu_Small_2021.pdf
https://dan-peer.tau.ac.il/wp-content/uploads/2021/01/ranit-kedmi-biomaterials-2010.pdf
https://physicsworld.com/a/positive-or-negative-nanoparticle-surface-charge-affects-cell-membrane-interactions/
https://www.sciencedirect.com/science/article/pii/S027869152200206X#!
We’ve been down this road before, and yes one of the authors most definitely knows a thing or two about genetic engineering.
“Codon optimisation results in G-rich mRNA that has unpredictable consequences”.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4412290/pdf/ppat.1004562.pdf
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5909458/pdf/gky187.pdf
We can go on like this all day.
https://osf.io/bcsa6/
Except G quadriplexes are found in the human genome. https://www.pnas.org/doi/10.1073/pnas.2203760119
“How Many Lives Did the Vaccines Save and How Many Did They End?”
Maybe the Times muppets will get Oliver Wright to do an article on it?
Sorry to Labour the point, but if a Times editor wants to dismiss us as “anti-vaxxers”, I will call them out for not covering this issue properly.
Oh, and well done to Mark Steyn (whose honorary knighthood will surely be on its way sometime soon…) for continuing to call out Twitbook for the pain they have been causing to ” covid ‘vaccine’ ” victims like Vikki Spit.
“It is looking very much like the vaccine programme failed to save any lives overall and was a very costly mistake.”
Soon to be reported on the “impartial” BBC…
(Mark Steyn interview here)
‘We just get abuse… I think the mainstream media is a large part of why that happens’ | Vikki Spit – YouTube
The reason people give abuse is because they are morons. The BBC might egg them on, but the fundamental cause is their toxic combination of stupidity and malice.
We all know that the gunk has at best done sweet FA and God knows what at worst. But as long as our institutions and media are funded by drug pushing philanthropists they will keep on publishing junk science and made up stats to keep the flocks attention. As I mentioned earlier the jabs are not doing the amount of notable damage, so the government are able to hide the harms. Along with not being classed as vaccinated until 2 weeks post jab, where we suspect alot of the “unvaccinated” deaths occured either from covid because of a buggered up immune response or from the jab which gave people covid like symptoms. The whole thing has been twisted beyond comprehension and if asked to explain I wouldn’t know where to begin.
“We should also note that the longer term impact of the vaccines is still unknown.
It is looking very much like the vaccine programme failed to save any lives overall and was a very costly mistake.”
This is how one begins to get red pilled. Will has come a long way.
The next question is: “why would Pharma and Govhealth and MSM all lie to us when many of those within these groups knew these were not going to prevent nor mitigate this virus that was not a pandemic level virus in the first place?
When I was a young’un at school I remember a teacher who said, one must always know the details, the facts, the “what,” “when,” “where,” “who” and “how.” But ultimately the hardest question to answer was always and forever the “why.”
So why Will Jones, why did this happen? Why is it still happening? Why are our children going to be injected or already have been?
WHY?
Ask a bookmaker. Maybe there’s a lot of Short-Term trading in the pharma business?
Side effects of smallpox and influenza vaccines
https://journals.plos.org/plosone/article/file?id=10.1371/journal.pone.0118283&type=printable
https://jamanetwork.com/journals/jama/articlepdf/201968/joc50154.pdf
Of course the vaccinated are at as great a risk as the unvaccinated simply because the vaccines were based on an early strain of the virus. There has been substantial changes to the spike protein, which is the main antigen for the antibodies to prevent entry into cells. This means that there are no antibodies or the correct memory cells around to block the virus from infecting, therefore the vaccinated will have symptoms, showing that their innate immune system is working. If the infection is too much for the innate system then the adaptive system is triggered, taking 7-14 days to become effective. The half life of the relevant B cells and antibodies is about 23 days, if there’s no infection or continuing infection then antibodies will diminish in number, with B cells becoming memory cells by the addition of triglycerides to the cell membrane.
Our immune system depends on the creation of B cells that can attach to specific antigens. Each B cell (and T cell) has a unique receptor that attaches to one pathogen and one pathogen only, with each B cell being different covering all of the antigens. Each and everyone of us has a B cell that can bind to SARS-CoV-2 or Ebola or any pathogen you can name. B cells are produced in the bone marrow, where they create their receptor by literally chopping up their DNA and recombining it. These B cells are then tested against “self” cells and if they react they are destroyed. Only B cells that don’t bind to self are released into the blood stream.
Might be worth trying to explain that the T cells are the useful longer term memory mechanism that we have. They are stored away well after antibodies are chucked out, are they not? Whilst I hesitate from advertising a certain institution, this might be vaguely interesting: https://www.imperial.ac.uk/news/201833/cell-immunity-what-does-help-protect/
Thats right, we have both memory T cells and memory B cells. They are basically ordinary cells that are somehow protected by triglycerides. It is interesting to note that one of the markers for concerns about ischaemic heart disease risk are raised triglyceride levels, if a person has a lot of memory B and T cells then could this account for raised triglyceride levels?
And here in the USA, there actually were more excess deaths *after* the novel experimental gene therapies misnamed “vaccines” were launched than before. If that’s success, I’d really hate to see what failure looks like!
What is the difference in death rates of those who got three or more doses compared to those who stopped at two? I would hazard a guess that the former is either worse or no better than the latter, at least in the long run.
Shame of the medical quislings who connived with the Covid State
https://www.conservativewoman.co.uk/shame-of-the-medical-quislings-who-connived-with-the-covid-state/
Paul Collits
Yellow Boards By The Road BUILD BACK FREEDOM …
Friday 12th August 12pm to 1pm
Yellow Boards
B3408 London Road,
Junction Russell Chase & John Nike Way Binfield
Bracknell RG42 6AE
Stand in the Park Sundays 10.30am to 11.30am – make friends & keep sane
Wokingham
Howard Palmer Gardens Sturges Rd RG40 2HD
Bracknell
South Hill Park, Rear Lawn, RG12 7PA
Telegram http://t.me/astandintheparkbracknell
How could the experimental biologicals save any lives? They are ineffective and unsafe. Period. They should have never been used. Early treatments were available, still are available. Sadly they were ignored, suppressed, banned. A disgrace and just shows how truly backwards the world is.
I think that part of the rationale for allowing Emergency Use was based on the absence of alternatives, which was a good reason to suppress them, otherwise Emergency Use would be invalid.
Steve Kirsch’s suggestion
What it may have demonstrated is that a short-cut route to product development is a bad idea. The “drug trade” has grabbed the opportunity from certain politicians, but who knows what the long term effect on it all will be? Not just this product, but others that would be affected by their loss of reputation.
I agree with Matt Dalby’s comment earlier on, but I sympathise with those who were caught in the spell dished out by the campaign – including a retired ex-GP that I used to use.
Back in March 21, I declined the offer, and am content that it was a wise choice, although I was 50/50 at the time. Pretty unlikely to change my mind, given he emerging evidence.
Back in Spring of 2021 our Gov. finally suspended AZ jibby jabs for the under 50s due to clear evidence that it was more likely to kill you of a blood clot than save your life from wu flu – the blood clots that they’d spent months denying didn’t exist. How anyone could have trusted them after this I have no idea. It was in the mainstream news, amongst the propaganda but it was there.
I really object to this phrase “saving lives”. Sorry but old people need something to die of and if it’s not covvie then it’s likely something similar or worse. Delaying this for a few months or years is not a life “saved”.
Do we stop treating heart attacks or stroke because the person is above a certain age but are otherwise healthy? Should I stop injecting myself with insulin when I reach 75, 80 or some other arbitrary number?
Are you advocating for a Logan’s Run scenario?
It’s about proportionality and return on money spent. Saving lives at all costs is impractical and immoral. Healthcare resources are not infinite and since time immemorial they have been rationed.
Down votes for linking to published papers, seriously?
Here are some more for discussion.
https://www.thelancet.com/pdfs/journals/lanepe/PIIS2666-7762(21)00259-3.pdf
https://academic.oup.com/jpubhealth/advance-article/doi/10.1093/pubmed/fdab327/6356442
https://www.researchgate.net/profile/Samuel-Ghasi/publication/362062716_THE_PSYCHOSOCIAL_FACTORS_OF_COVID-19_VACCINE_EFFICACY/links/62d46ab4fd347a451bc5df79/THE-PSYCHOSOCIAL-FACTORS-OF-COVID-19-VACCINE-EFFICACY.pdf
SARS-CoV-2 variants have an increased resistance to interferons
https://www.pnas.org/doi/10.1073/pnas.2203760119
My impression of vaccination in general and these jabs in particular, is that, in line with the old adage that “there’s no such thing as a free lunch”, any kind of sliver bullet remedy will always be accompanied by an equal and opposite reaction as well as its intended effect.
There is no such thing as a medication that does nothing but good.
While the short-term adverse side-effects are of course important to analyse, the long term consequences are in fact much more important because the numbers affected by long term effects will of course be higher than those affected by short term effects because there is more time for those to happen. (You could even take into account the genetically inherited effects on future generations!)
Long term effects will also happen for a longer duration, or even permanently, than short-term adverse reactions. It could be, for instance that our biochemistry is permanently altered, and once the effectiveness against Covid has diminished to nothing, this effect would be purely negative.
All just speculation of course, but to use the data on short-term effects for cost-benefit analysis is to see just the tip of the iceberg.
Which is why it’s quite handy for the Satanists that the control group in the long term safety trials was given the “vaccine” so now they can blame long term effects on anything they feel like – Long Covid, Global Warming etc.