
There follows a guest post by Dr. David Livermore, Professor of Medical Microbiology in the Norwich Medical School at UEA, who says that counting deaths from COVID-19 is tricky as it’s a pathogen that primarily endangers the already frail or at-risk.
Counting deaths is straightforward when a pathogen kills the healthy, as with ebola or plague. And it wasn’t hard to agree that HIV was the underlying killer to count even when AIDS patients succumbed to unusual fungi and cancers.
It’s not so easy when a pathogen primarily endangers the frail. Many antibiotic-resistant ‘superbugs’ are hard to treat and potentially lethal in a person with leukaemia, but harmless for the fit and healthy. What killed the patient, the leukaemia or the carbapenem-resistant Klebsiella? It’s hard to know, and easy to exaggerate, as when Jim O’Neill predicted 10 million deaths annually from resistant bacteria by 2050.
Similarly for Covid. Consider the unhappy realm of Scotland. As of March 17th, there were 11,075 deaths attributed to SARS-CoV-2, and 13,563 with the virus mentioned on their death certificate. Of these, 29% – around 3,600 – were in care homes. A separate report tells us another 1,986 (around 17%) “probably or certainly” resulted from hospital-acquired Covid, with three quarters of these folks aged over 75 years. So, almost half of all Scottish Covid deaths were ‘healthcare-associated’ (nosocomial) and – almost by definition – were folks with co-morbidities or vulnerabilities. On entering a U.K. care home in the pre-Covid era one had a median life expectancy of 462 days. For nosocomial Covid, mortality was 28.2%, or around 100-fold above the general Covid fatality rate, telling you a lot about the vulnerability of the Scots who succumbed.
This means that, when counting deaths among those infected by SARS-CoV-2 (or, similarly, antibiotic-resistant bacteria) it’s vital, though difficult, to distinguish ‘died with’ and ‘died from’. The death certificate has boxes for “Disease or condition directly leading to death” and “Other significant conditions contributing to death”, but how accurately these are completed is less than clear. A 2012 review by the ONS concluded that around 22% of death certificates were wrong, half of them in respect of the broad underlying cause of death.
Collateral Global’s latest report, by Tom Jefferson and team, explores this subject, reviewing responses from Government and NHS agencies to over 800 FOI requests asking how deaths were attributed in the case of Covid. Numerous inconsistencies emerge, even when the same agency was asked the same question by different enquirers, let alone when the same question was posed in different devolved administrations. Overall, 14 different ways of attributing the cause of death were found. Around 7.6% of care home deaths were attributed to Covid alone, which seems unlikely, given the frailty of the care home population. The authors also note “availability bias”, meaning a propensity to include information that is available – e.g. a Covid test result – whereas other contributory factors in a complex patient might pass unremarked or unsuspected. I’ll come back to that. Notably, few autopsies were done.
In Sweden, a review of 122 community deaths with COVID-19 recorded on their death certificate concluded that 70% had primarily died from other causes, with Covid as a contributory factor. I can’t find a similar review of the U.K., but ONS data suggest that death totals may not be very accurate.
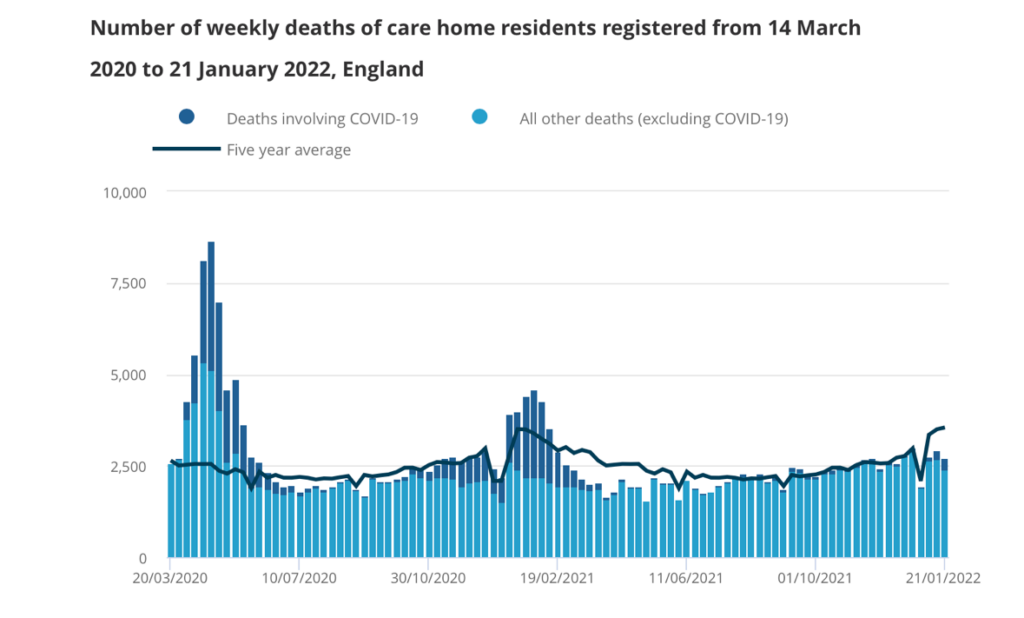
Figure 1, below, charts care home deaths in England from March 2020 to early this year. Note, first, the spike of light blue – supposedly non-Covid – beneath the dark blue Covid deaths in the first wave of March 2020. This light blue far overtops the five-year death average. Either Covid deaths were undercounted (likely) or something unknown was killing care home residents (unlikely).
Second, come to February 2021. Here, Covid is ‘involved’ in nearly half of all deaths, and ‘non-Covid’ deaths are far below the five-year average for pre-Covid years. This might be because numbers of residents were unusually few, but this seems unlikely, because non-Covid deaths had been near-normal in the preceding summer. The likely explanation is that Covid was being counted as ‘involved’ when the virus was inconsequential and the resident would have died anyway.
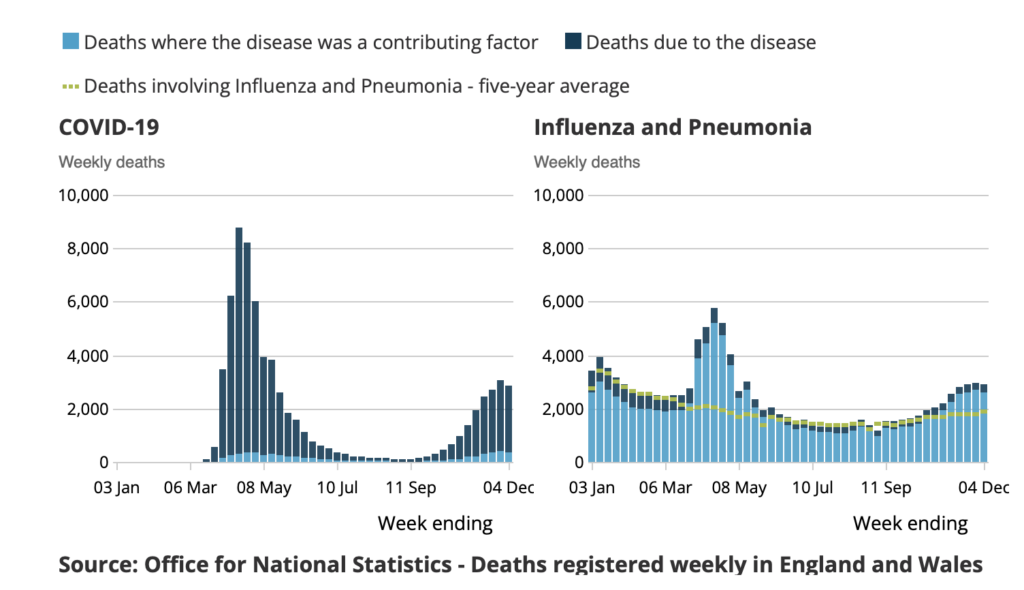
Next, consider Figure 2, a format that the ONS no longer publishes and upon which I have commented previously. The left-hand panel shows that, for patients dying with known Covid pneumonia in 2020, death was attributed as ‘due to’ the pneumonia in over 90% of cases (dark blue). By contrast – see the right-hand panel – few pneumonia patients without a Covid diagnosis had their deaths listed as ‘due to’ the pneumonia. Yet the May and December peaks on the pneumonia chart coincide with the Covid peaks and must substantially comprise patients with undiagnosed Covid. I believe that this illustrates Jefferson’s “availability bias”. When there was a virology result for a notorious pathogen, there was a much greater propensity to attribute its pneumonia as the cause of death.
Last, there is the chaos of the real world in a crisis.
At the start of the pandemic, the Government established ‘PMART’ teams to visit homes and care homes where someone had died. These comprised a clinician, a police officer and a fire service driver, all uncomfortably trussed in PPE. The clinician could be a nurse, a medical student or some other health professional. Unless foul play was suspected they took the lead in attributing cause of death, with a certificate issued later after review by another medic, who didn’t actually see the deceased.
My friend, a coroner’s pathologist, tells me that the PMART teams preferred to be in and out of the deceased’s residence as swiftly as possible. As he puts it: “It was a perfect time to poison unwanted relatives, telling the clinician they’d been ‘coughing bad and struggling to breathe’.” And, whilst nobody is suggesting that the spring of 2020 was awash hidden murders, it’s hard to believe that the death certificates of the period are particularly precise.
Dr. David Livermore is Professor of Medical Microbiology in the Norwich Medical School at UEA.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Unfortunately the average life expectancy of an inner Glasgow resident is on a par with some sub Saharan Africans
Yes … not much sun/vitamin D in Glasgow either.
Despair plus vit.D deficiency = early death.
Death via starvation v death via battered mars bar.
Or was it the deep fat fried Mars Bars?……. we may never know
Or, as Dr Martin Kendrick holds, from the stress of a life that’s hopeless and without many oases of relief.
“Either Covid deaths were undercounted (likely) or something unknown was killing care home residents (unlikely).”
I think it’s spelled, Midazolam
You have to spell it out for these experts:
M I D A Z O L A M
When you say Midazolam, do you mean Matt Hancock? Asking for a friend.
In Hancock’s case it is Mad-as-a-lamb .. as in a Spring lamb.
or more likely in his case – a spring chicken
(Links precede quotations from the linked document.)
https://web.archive.org/web/20200909153336/https://www.uhb.nhs.uk/coronavirus-staff/clinical-info-pathways/clinical-info-pathways-downloads/End%20of%20Life%20Care%20for%20Patients%20with%20COVID-19.pdf
End of Life Care for Patients with COVID-19
…
The following advice relates to patients being managed OUTSIDE OF CRITICAL CARE [emphasis in original] and who are thought likely to die in the coming hours or days despite all previous or ongoing best efforts.
…
There are reports that some patients dying from COVID-19 suffer a significant degree of delirium or agitation which may be difficult to manage.
…
Patients, families and sometimes colleagues will need support and reassurance that the use of drugs for symptom control is to ensure comfort and NOT to speed up the process of dying.
…
Drugs for comforat [sic] at the end of life include the following: Benzodiazepines – Midazolam, lorazepam – [uses:] Fear, anxiety and agitation
…
Deliberately there are no maximum doses per 24 hours stated for the drugs below.
…
Benzodiazepines = FIRST LINE for anxiety, fear and agitation
Midazolam – suggest start with low doses for patients naïve to this drug but be prepared if response is poor or short lived and anxiety is severe to escalate dosing sharply.
Generally: Start with 2.5 mg SC or IV
If patient is particularly frail: use 1.25mg
If extremely distressed or show tolerance to this group of drugs: may require higher doses e.g. 5 -10 mg
…
For patients not responding to midazolam – this might be because doses have been too low or not frequent enough. Some patients might need much higher doses than normal.
https://www.bradfordhospitals.nhs.uk/wp-content/uploads/2020/02/1.1.1.4-Sedation-Policy.pdf
Policy on Sedation for Procedures in Adults
…
Medication guidelines for adult patients receiving procedural sedation.
This guideline is not intended to be all-inclusive, but to serve as a guide. Please note that some patients may not tolerate even these recommended doses.
…
Midazolam – iv – Initially 2mg (elderly 0.5-1mg), Titrate 1mg every 2-5mins (elderly 0.5mg). Usual total dose 2.5-5mg (max 7.5mg); elderly max 4mg
https://bnf.nice.org.uk/drug/midazolam.htm
Side-effects
For all BENZODIAZEPINES
Common or very common
Alertness decreased; anxiety; ataxia (more common in elderly); confusion (more common in elderly); depression; dizziness; drowsiness; dysarthria; fatigue; headache; hypotension; mood altered; muscle weakness; nausea; respiratory depression (particularly with high dose and intravenous use—facilities for its treatment are essential); sleep disorders; tremor; vision disorders; withdrawal syndrome
https://dailyexpose.uk/2021/08/29/midazolam-was-used-to-prematurely-end-the-lives-of-thousands-who-you-were-told-had-died-of-covid-19/
Note: The Exposé referred to a Norfolk and Norwich University Hospital document that has now been expunged from the NHS web site. The Internet Archive has a catalogue page, for the document, but does not provide the document, itself: https://web.archive.org/web/20200119120615/https://www.nnuh.nhs.uk/publication/safe-use-of-intravenous-conscious-sedation-in-adult-patients-jcg0004-v3/
Ha – just commented about this on the previous article. The old chestnut regarding with or of covid. In March 2020 in discussion with a colleague we discussed how significant infection was in end of life care, leading to death. Be it bacterial or viral, it is in my experience very common. Infections that cause few issues to the healthy can be lethal to to the frail. Imagine what the picture would look like if all such infections were tracked like covid. I have sat with many people in their last moments, family and friends. Part of the cycle of life, but something oft forgotten. A destiny for many of us.
There has been a crackdown on the profanities, but why are the antifanities getting a free ride?
“Fanity of fanities, all is fanity.”
A buse is unacceptable but multiple buse appears to be ok
And a tack. Many tacks no problem.
Yes, and you wait for a buse for ages and then three come along at once.
Infanity, infanity , you’ve all got it, infanity. (After Kenneth Williams)
It’s quite put me off using my favourite Chaucer quotations on this website.
I’ve no idea how such a potty-mouth acquired such admiration.
No offence to the Good Doctor Livermore, but we’ve all been saying this since March 2020. I don’t even have a degree :/
Indeed. When you remove all the checks and balances, the data become meaningless. (But still useful if you aim to terrorise the populace.)
I think, like a few people posting to this website and clincians/scientists going on national TV, they feel less threatened by Big Tech and their colleagues by expressing their long-held but private scepticism / doubts over what has been going on and policy in general as regards the COVID response.
Whilst I can fully understand them being silent – as their careers and livelihoods may well have been on the line*, I suspect a good number have pretended to be on the authoritarian side – passively – by ‘liking’ the comments, tweets etc from Fauciists and doing the opposite for many of us who were arguing the opposite back in 2020.
* being a scientist or clinician isn’t the great eerience the media likes to portray – in my experience dealing with them as an engineer over the years on project work, they can be just as egocentric and nasty as entertainers and politicians, thus why some stay silent in order to not be ‘cancelled’.
Unfortunately that means MANY VERY BAD things often go unreported or what in reality is no where near a ‘consensus’ of opinion or actual fact is portrayed as such.
Note that as the debate (and as facts emerge) swings our way on COVID, some are already changing their tune to suit which way the winds are blowing, though some, it appears, are still attacking the sceptic side from a ‘middle ground’ position because they are as yet unsure whether our side will end up the winners.
I don’t even have a degree :/
Which, of course, does not stop you being both intelligent and well-informed….
A degree is essentially a social mark of acceptance. When societies are fair, truthful and accurate, this mark is worth something.
At the moment, holding a degree conveys negative esteem in my view – even degrees in topics which are dispassionately apolitical, such as Mathematics.
It was said very much tongue in cheek, but yes, I agree
While this article is interesting and informative, right from the title onwards, it does sound like a case for the defence.
There must be accountability here. From a propagandised headline of 156,924 deaths with a positive covid test to 18,939 deaths of covid without a pre-existing condition to 6,183 deaths with only covid on the death certificate, we have a 25x multiplier. (ONS data up to 31 December 2021).
This is unacceptable and not due to ‘being difficult to count’.
I agree , dancing on a pin head. The State killed old people in April 2020. Mainly through imbecilic diktats brainlessly followed by ‘health and care’ workers.
‘Hancock the Terminator’… coming soon to a cinema near you.
If you believe such a thing as Covid 19 even existed.. this FOI request is a long way from 130/50,000
ENGLAND WALES (alleged) COVID DEATHS
COVID-19 deaths and autopsies Feb 2020 to Dec 2021
Release date:17 January 2022
TOTAL : 6182
https://www.ons.gov.uk/aboutus/transparencyandgovernance/freedomofinformationfoi/covid19deathsandautopsiesfeb2020todec2021
Seeing as on average 1,400/500 die every day in the UK, around 500,000 a year.. 6,182 over 22 months is totally insignificant. And yet our personal freedoms and economy have been nigh on destroyed for this supposed killer disease..!!!!
Which is why the Government and their scientific advisors will fight tooth and nail to avoid the truth coming out.
On top of this, the WHO is still operating in maximally hysteric mode: Infections are rising again! The worst is yet to come!!, something they’ve bee continuously claiming since 2020 and need to keep claiming because – minus the policy response to COVID – nothing particularly bad has happened because of it so far.
The one policy decision of Donald Trump I completely agree with was to stop sending money to this gremium of experts in freaking out because of everyday occurrences and then, throwing the baby away as precautionary measure while keeping the bathwater.
Yes, this is the figure that I refer to, together with the 18,939 without pre-existing conditions here. They really benefit from a closer look from different angles. The numbers are mind boggling!
Quite. Succinctly put too, I hasten to add.
Somebody the other day was banging on about Covid killing 6 million people over the past 2 years, didn’t say of or with but 6 million dead. However, to put some perspective on the situation 9 million a year starve to death, so 18 million over the past 2 years.
Given the results of the Covid measures, now followed by the food, energy and other problems, the abandonment or delay of curative or preventative treatments against “normal” diseases in many countries, etc., and let alone any consequences of the Covid “vaccines”, I think the casualty lists will be enormous. I see nothing that will make them go down, only a multitude that will make them increase.
Hancock, Whitty, Vallance, I look forward to the day you are made to explain, under oath, the reasons for your actions and advice.
They just need to say, to keep people SAFE, and everyone melts.
Yes, for the greater good, obviously…
I think your only hope of ‘justice’ is via a strong belief in karma. Life will sort them out. I’ve got more chance of becoming Pope than you have of seeing them brought to book, unfortunately.
For that we would need an independent judicial system and independent judiciary.
Do you see that at all?
Not really and not as thing stand. But circumstances can change and it does happen when the time is right… We are approaching that point.
https://ourdecisiontoo.com/Issue/there-s-nothing-left-to-do-but-go-our-separate-ways/320/
Spoil sport. I was hoping to see them on the rack.
‘And it wasn’t hard to agree that HIV was the underlying killer to count even when AIDS patients succumbed to unusual fungi and cancers.’
Sorry, what now? That is quite the pivot there, from ebola. Not hard to agree? Why, because your entire professional reputation depended on going along with it? Or because there was clear scientific peer-reviewed evidence that patients who succumbed to unusual fungi and cancers did so because their killer was HIV? If it’s the latter, as I assume from the sound of spluttering I’m hearing, then it shouldn’t be hard, as you put it, to point to the paper which established that fact. Can we have the citation please? Errr no, we can’t, because no such paper exists.
I think it’s time for Daily Sceptic to change its masthead. Clearly it is no longer tenable to proclaim that this is a site that encourages the reader to ‘Question everything’. It should now have an asterix after the ‘everything’, then down the bottom, in tiny letters, ‘except the viral theory of disease, including the notion that HIV is the cause of AIDS’. Sure, question everything else, but don’t be questioning these sacred cows. That would be beyond the pale.
Anyway, more of these great experts coming out now with brainy explanations of how to close the stable gate, with the horses long gone, galloped over the horizon. I guess it’s safe to be brave now. The cancel culture caravan has moved on to slamming anyone not collecting money for Ukraine or changing their social media profile to the blue and yellow..
It should now have an asterix after the ‘everything’, then down the bottom, in tiny letters, ‘except the viral theory of disease, including the notion that HIV is the cause of AIDS’.
It might be interesting to consider all the theories which are nowadays unable to be questioned because to do so would result in professional suicide.
Gravity*, Evolution, Climate Change, Smoking as a cause of Cancer, the Linear no-threshold model of radiation damage…
*the commonly accepted model of Gravity HAS, in fact, been shown to be wrong, but it has been used so often to smear free thinkers that it we allow double-think between technical and lay persons.
Well in order to question, you have to have something to question. By publishing such articles it gives us an opportunity to question and comment, which you have.
The modus operandi of the MSM and Social Media Thugs is to publish only approved articles.
Do you want DS to be like that, so we live in our self-constructed echo chamber?
Switched on to BBC, by mistake, still pumping out the message that ICU are full of unvaccinated. Do not believe that, still doing the Nudge Units job when they admitted deliberately terrifying people, disgraceful.
Ditto, all MSM, IE:ITV,C4,SKY ETC.
ALL BLEEDIN LIARS!!!
Right from the start it would have been possible to split covid deaths (and hospitalisations) into three groups:
The other thing they could have done is had the attending medic estimate the deceased ‘quality adjusted life years lost’ — this would have indicated the seriousness of the covid pandemic to society.
They did neither of these things, resulting in two enormous problems:
Differential diagnosis by clinical history, symptoms, test for antibodies if a particular pathogen is suspected.
But The Science™️ replaced long established medical good practice in the pursuit of political objectives.
The other way of looking at this death issue is to stop and consider, when all this lockdown madness ended and things opened up again, everybody seemed to still be here! the same people at the swimming pool, in the pub and turning up at village hall events. I find it hard to find anybody who is no longer around, anecdotal I know but if this had been the black death we would have noticed swathes of our friends and acquaintances having disappeared. The fact that we are having to do in depth studies on deaths to try and get some figures indicates to me that overall this has not been a major death event. Indeed looking at ONS total registered death figures apart from a few months in 2020/21 there has been nothing untoward about deaths.
The major issue with deaths is with increased deaths in the under 60s and possible vaccine links
The Covidaholics always seem to know someone who knows someone who is related to… (almost ad infinitum) who might just have died from something attributable to a seasonal pathogen. They use that tactic whenever they feel an attack of logic and rational behaviour approaching.
Hold Them Accountable.
https://holdthemaccountable.world/
This is worth a look.
Dr Cowan discussing a peer reviewed study published in the Lancet where they acknowledge that the PCR tests used for sars-cov-2 were not actually testing for a any new virus but were in reality testing for known human proteins.
The whole thing has been a massive scam from start to finish.
From 32:50
Scientific Trickery?! Evidence For Pathogenic Sars-CoV-2 Virus Almost Totally Lacking?https://odysee.com/@TimTruth:b/Virology-on-Trial-part-7:1
AFAIK most PCR tests screen for ORF1ab, N gene, S gene, RdRp gene or E genes. And these are not novel or exclusive to Sars-Cov-2?
E genes are supposedly not specific to SARS-COv-2.
N genes were pointed out as unreliable in Christian Drostens original application for the Covid test protocol in Eurosurveillance.
RdRp genes are apparently insensitive and dimerize to other molecules.
Bullshit baffles brains, as the medical ‘opressors’ in this situation know all too well as they ‘weaponise their privilege’ (h/t millennials). Unfortunately most of us are left lacking in this particular regard, however it always amused me that in the West the Gold Standard test results for this dreadfully dangerous pathogen were not provided to patients? No information is provided, no Ct, no test kit, reagents or primers, no genes. You simply must take a test for the deadly deadly oh so deadly mystery lurgy, but you’ll only get a smiley face or a sad face in reply. Its all very technical you see.
So we don’t actually know the granny-count?
From January through to end of March 2020 and then the rest of the past wretched two years, did anyone other than me note the astonishing absence of terminally sick people all around them – family, friends, neighbours, work colleagues – struck down by this ‘dangerous, serious, deadly, fast-spreading, killer’ virus – no cries in the street, ‘Bring out your grannies’, no convoys of hearses carrying away the dead to the plague pits?
The thing that truly has shocked me – I do mean shock – is just how many stupid people there are in the populations of our ‘advanced’ Countries. And even now the same fools are going ga-ga over Ukraine determined to do themselves more economic self-harm, because,,, reasons.
I thought the strangle hold of the MSM over the minds of the population was failing due to the rise of alt media, turns out the vast majority still believe what the BBC (transgender) man tells them.
“cries in the street, ‘Bring out your grannies’”
Some days you could hardly get out the front door for the bodies piled several feet high.
Having recently nursed MOH through serious illness caused by covid, I doubt that most care home residents would or could have received the same and necessary level of care. The homes simply wouldn’t have had sufficient numbers of staff.
Having said that, my elderly mother, who has Alzheimer’s, tested positive for covid back in January 2020. She was a little unwell, and lethargic for a few days. That was all. She recovered ok.
MOH, 20 years younger, was seriously ill and admitted to hospital for a week. I also had covid and recovered after a week(ish).
it’s a highly variable virus.
Are you certain it was Covid, and not, for instance, flu or RSV (which has almost identical symptoms)?
The miscounting is clear, with only heinous intention.
You don’t need to add narrative-friendly nods to ensure publication anymore Professor, like suggesting Coivd-19 care home deaths have been underreported. Unless you’re angling for a role at The Economist’s bad-faith extrapolation unit.
Anyone who has completed a death certificate in the elderly is aware that ultimate ‘ Cause of death ‘ is impossible to know. The large numbers of recorded deaths in the 70+ with no comorbidies is a myth. Most medical records and prescriptions in this group are vast. The question we must ask is why the misinformation? I venture that if you put Covid19 on the certificate you were never challenged and if the patient had a positive PCR you had the proof. Why risk putting a more complex explanation? Virtually no PMs in this period!
According to the ONS: “COVID-19 deaths are those deaths registered in England and Wales in the stated week where COVID-19 was mentioned on the death certificate. A doctor can certify the involvement of COVID-19 based on symptoms and clinical findings – a positive test result is not required.” Just one person’s opinion – no specific test is required to prove it at all.
Dr. John Ioannidis declared the infection fatality rate right at the beginning of the scamdemic. Nothing has changed. Perhaps with early treatment with repurposed drugs we now know work, those numbers will be reduced. What exactly are we waiting for?
If it’s THAT difficult – then why not look at the number of burials/cremations nation-wide in 2020/21 and compare that figure with the average from the past five years? Then assume if there’s an increase it was due to SARS of some kind.
Is it possible that part at least of the reason for less infection in the unvaccinated is that they have already had undiagnosed Covid in a mild form which ha given them greater natural immunity than that given by the vaccine? Is it time for goverments to admit that the vaccine doesn’t work long enough to be worth the cost and stop paying billions to the Pharma companies. Is there a way of transferring natural immunity between people? Would that be better than the vaccines?
“In the UK, 458 000 people live in care home settings in which 103 000 deaths occurred in England and Wales in 2012 (20.7% of all deaths), half of such deaths being from dementia. Care homes may be categorised into residential care homes that provide personal care only and nursing homes that provide personal and nursing care. They are increasingly recognised as important providers of palliative care for older people, potentially offering a homelike environment, continuity of care, and relationship-centred care until death. ” From an article in The British Journal of General Practice, September 1st, 2014 entitled “Living in uncertain times: trajectories to death in residential care homes.”
No Vit D or C, no Ivermectin – just Midazolam and dehydration.