Steve Kirsch has analysed the data obtained from Barry Young, the New Zealand vaccine data whistleblower who was recently arrested under mass ‘breach of privacy’ legislation and faces up to seven years in jail.
Steve’s statistical analysis resulted in him claiming that one person per 1,000 doses of the administered vaccines in a standard population died prematurely as a result, with that result skewed heavily to the over-60s.
This is consistent with the trend that I have commented on already in June 2022.
Several other sceptical commentators have since weighed in with their own analyses and criticised the structure of the data and commented on whether or not it can be useful in any way. In particular I highlight those from Igor Chudov, William Briggs and Eugyppius.
Since these posts were published there have been some further responses, which more or less point to an acceptance of the fact that the data are far from perfect, lacking especially in perhaps the most important aspect of all, namely any control data on unvaccinated mortality.
Unfortunately at this time it is therefore still impossible to state categorically that it is the vaccines that are causative in the excess mortality being experienced in New Zealand or around the world since 2021. Other factors including longer-term effects from Covid infections and harms from the effects of the various NPI responses could for example be responsible in theory.
However, it is now generally accepted that the New Zealand data are very likely to be genuine, and the dataset’s haphazard structure is a reflection of the way such data are recorded in New Zealand rather than anything else. It is also a very large data leak, comprising mortality figures for about a third of all records on vaccines administered there during the last two and a half years or so.
This means that should a safety signal be found, it would represent far and away the biggest red flag to date. This should therefore become a huge pressure point to get the authorities to release a full dataset of all mortality since the vaccine rollout, which will be required to ascertain once and for all whether or not the vaccines can really be called ‘safe and effective’.
Consider therefore what we can see in this dataset, especially in relation to the analysis by William Briggs, who presents charts showing mortality spikes after each vaccination and compares these against the official timeline for Covid deaths in New Zealand. The Covid mortality spikes did not begin in any significant way until sometime in March 2022.
Briggs writes:
Since, officially anyway, there were almost no ascribed Covid deaths in 2021 in New Zealand, then the August peak in deaths for those who only had one or two shots could not be Covid and had to be something else
The same is true for the January 2022 peak, which had only a handful of official Covid deaths, but which saw a large number of people with three shots dying.
The lack of Covid deaths for the first two mortality spikes is strongly suggestive of a signal – since the first three vaccinations were all administered prior to any significant Covid deaths, Covid was not a factor in the ensuing abnormal mortality.
But just how abnormal was this mortality actually? Briggs tells us that just under 1% of the people who received jabs one and two died in the ensuing mortality spikes, which all occurred within a six-month period. That is roughly double the normal background mortality rate (for comparison the U.K. yearly rate is a fraction over 1%).
Almost 2% died with the third jab. Double as many again. And for the period after the fourth jab (which does include some Covid deaths) it was 2.8%. To me, this suggests a cumulative effect and that excess mortality is spread out for several months after each jab. Despite this, Briggs writes:
If shots were killing some people more or less right away, we’d expect a bump close to the shot day. But you’d also expect that if the shot was killing people, the ones most susceptible would die after the first, or maybe second, shot. People would not be as likely to die after three or more if they tolerated the first two, unless there was a cumulative effect. Which we could not reliably see in this short-time-period data.
In his commentary, Eugyppius suggested that the overall excess mortality could not account for Steve Kirsch’s guestimate of one excess death per 1,000 jabs, which should equate to 12,000 excess deaths based on the 12 million jabs administered there. But that argument depends very much on where the line is drawn regarding ‘baseline’ mortality.
Look for example at this recent article from Clare Craig, and also at this estimate of what is actually excess in New Zealand.
My take on the excess mortality uses a baseline of 33,366 for the average of mortality in 2018, 2019 and 2020 (figures taken from the Eugyppius article). Clare Craig tells us that from her analysis:
It would suggest there were bad years for mortality in 2017 and 2018, when there was indeed a high influenza mortality, but that in 2020-2021 the expected number of deaths occurred.
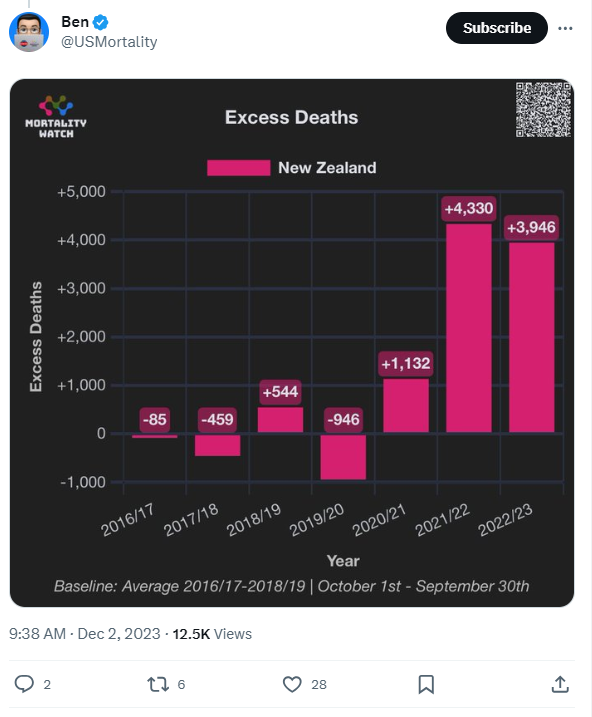
So as a baseline, the average of these three most recent years before Covid and vaccination began in New Zealand seems reasonable. Using this average there was an excess in 2021 of 1,566, in 2022 of 5,208 and perhaps 1,000 less than that in 2023. This adds up to nearly 11,000, and if most was a result of vaccination harms, then this would fit with Steve Kirsch’s estimate. So the question remains, how much did actual Covid deaths affect excess mortality?
Note that New Zealand only experienced significant Covid waves from Omicron and the strains that came after it, and these were not nearly so deadly as the earlier waves experienced in the U.K. and elsewhere. Added to that, New Zealand experienced the relative absence of influenza during the Covid years, as did many other countries including the U.K.
This suggests that respiratory deaths were trending low at the time, meaning overall deaths should have been below average and the fact they weren’t is itself a signal of something unusually harmful at work. In other words, the excess deaths may be partially hidden by the lack of the usual respiratory deaths. I am convinced that non-respiratory mortality (NRM), as I have written about in previous articles (most recently here), would account for most of the 11,000 excess deaths and would tie in with Steve’s hypothesis.
It is a pity we are still no further ahead despite the plucky individual who sent Steve the data. To echo the words of Guy Hatchard: “The message that most resonated with me during the interview was the heartfelt plea from the whistleblower for others to speak up.”
Finally, the latest developments in this saga are that Steve Kirsch had a discussion with William Briggs about his critique and Steve also held an X space to counter criticisms of his claims from Kim Dotcom and Dr. Shiva Ayyadurai.
Stop Press: Dr. Shiva Ayyadurai has been caught publishing dodgy analyses before so may not be the most reliable analyst. Back in November 2020, he was behind a notorious analysis of voting patterns in the U.S. Presidential election that claimed to provide robust statistical proof that the voting machines had been programmed with an algorithm that systematically switched thousands of votes to Biden from Trump in heavily Republican districts. In fact, Dr. Shiva’s analysis just described a natural pattern that occurs when voters are able to choose whether or not to split their votes between parties – as the Republican vote share in a district increases, the pool of those voters who choose to split their votes between parties becomes more negative towards the Republican Presidential candidate simply because a greater proportion of those wanting to split their vote are Republican supporters not wanting to vote for the Republican Presidential candidate. Despite this, Dr. Shiva’s claims were among those promoted by lawyer Sidney Powell, leading to her being disgraced (she recently pleaded guilty to crimes in relation to the claims).











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
There’s also an increase in alcohol consumption, that can raise the risks of gout.
Methinks that’s rather a case of coincidence of consumption of alcoholic drinks and lots of junk food.
High wine consumption is linked with gout – it’s generally believed that high alcohol consumption leads to over-production of uric acid, which causes gout. Some say red wine in particular, and although my father-in-law is only a sample size of one, he has gout and no one else I know drinks more red wine…
High wine consumption is linked with gout – it’s generally believed that high alcohol consumption leads to over-production of uric acid, which causes gout.
The teetotallers will link everything to alcohol, be it dying of thirst, because of their a priori convicton that everything bad which happens to humans must be caused by it. In reality, nobody really knows what causes gout and nobody’s much interested in knowing, either. It’s a fairly harmless albeit painful disease whose symptoms can be handled with the the usual suspects medication.
What is “junk food”?
Food which should be thrown away before eating due to its atrocious quality. This applies to most of everything which can be bought in all of these street food outlets.
“The number of cases has risen by 20% in three years, with 234,000 patients admitted to hospital with gout in 2021/22, NHS Digital statistics show.”
That’s 234,000 candidates for bogus covid-19 diagnosis, then.
Might not be worth reading in full, but I like the image of the character under the headline! Reminds me of the occasion in early 2020 when he was allegedly admitted to hospital in London (St. Thomas?) with C-19. There was a report from that place as to what his weight was; not nice (the value quoted, not the publication of it!). Apart from what the Mail says, I think it is likely that being overweight can screw up one’s immune system in general. In particular, at least one of our important vitamins (D) tends to be fat prevalent.
In simple terms, being obese tends to make one more vulnerable to a range of different infections, such as the, err, common one under consideration.
I am shocked that people diagnosed with gout are hospitalised.
Agreed.
Gout is predominantly a genetic disorder caused by overproduction or reduced excretion of uric acid.
Inflammatory episodes my be triggered by alcohol, certain dietary factors, dehydration (possible with a heat wave and/or water shortage) or trauma.
In my experience outpatient diagnosis is frequently incorrect as a correct diagnosis relies on aspiration of joint fluid and the finding or monosodium urate crystals in the fluid.
Even that can sometimes give an incorrect diagnosis.
Since Covid “vaccines” have become prevalent I have seen a huge increase in presentations with acute joint swelling.
Some of these have been labelled as gout by ED staff.
I have performed multiple joint aspirations on these patients as well as other investigations, and found very few to be caused by gout.
My conclusion is that Covid “vaccines” cause inflammatory joint swelling in a proportion of patients.
I have seen no increase in gout presentations.
It is very rare for a patient to be admitted to hospital for gout.
Many thanks for this in-depth explanation.
Very interesting. A friend gets gout and he doesn’t drink alcohol but has to put up with all the comments that go with being diagnosed.
My first post so be gentle with me.
My first cynical thought was that, as gout is a consequence of excess purine intake (port and red wine, but also red meat and, curiously, fructose – https://pubmed.ncbi.nlm.nih.gov/16234313/) this story would be yet another flag-waver for the insect diet. I was gratified to find this – as yet uncensored – little gem which notes the high levels of purine in several edible insect species. https://www.wageningenacademic.com/doi/abs/10.3920/JIFF2018.0023
While still playing into the pockets of Big Pharma ref drug based treatment options, the best, cheapest and most effective solution is the phrase ‘oi lard*rse, stop stuffing your face with cr*p and get some exercise’.
Excellent first post so please keep them coming.
Pleased to welcome you aboard.
Thanks!
Seconded!
Gout may be caused by excess histamine consumption and/or production. Foods high in histamine include prawns, seafood, oily fish eg salmon, cured meats, aged cheeses, avocado, pickles, wine, sherry and port, and foods which trigger histamine production include egg whites eg in meringues and macaroons, chocolate, citrus fruits, horseradish, shellfish, strawberries, and some nuts …. basically my favourite foods ( when not eating gluten, at which times my favourite food is pizza! ), and traditionally central to the diet of the rich.
), and traditionally central to the diet of the rich.
I did think that the swollen and tingling toes said to be part of covid symptoms at one point might be something else.
A very powerful instant anti-histamine is vitamin C, which is a relief! ( I had an attack recently, with the odd nausea it can cause too, after eating a bit more sashimi, seafood, and avocado than I’m used to, and drinking plum wine and sherry with them )
Lemons are very useful as they are usually much richer in vitamin C than in their histamine triggers. And high-strength soluble vitamin C tablets will also usually work to relieve symptoms.
Some people are more sensitive to/prone to histamine “storms” than others.
Histamine is essentially an inflammatory reaction, and can be exacerbated by stress …
Sunshine , and Vitamin D, on the other hand help to down-regulate the immune system’s tendency to inflammation … A lot of people may have lost out on their usual doses of Vitamin D over the last 2 years. ( Rich people used to avoid the sun because white skin was prized as sign that didn’t have to work ( outside )).
Interestingly, ( to me anyway ), in the context of covid, “long covid”, and the changes in behaviour and diet that lockdowns caused, ( less time outdoors and different foods eaten because at home ), excess of histamine consumption and/or production can cause not only the swollen, red, sore fingers and toes and stiff aching joints which may be diagnosed as gout, but also the following:
), in the context of covid, “long covid”, and the changes in behaviour and diet that lockdowns caused, ( less time outdoors and different foods eaten because at home ), excess of histamine consumption and/or production can cause not only the swollen, red, sore fingers and toes and stiff aching joints which may be diagnosed as gout, but also the following:
Chronic inflammation
Tingling/numbness in hands and feet
Difficulty regulating body temperature and an increased tendency to sweating
Hives, rashes, itchy skin, flushing
( Quite frightening ) racing heart/heart palpitations
Low blood pressure
Difficulty/obstructed breathing, sinus issues, bronchitis
Post-nasal drip, persistent throat clearing, weepy eyes
Digestive disturbances/distress
Headaches, dizziness
Anxiety/feelings of dread
Insomnia
Chronic fatigue
Thyroid disruption and all that can lead to; energy and mood disorders among other things
Histamine has a systemic effect on the body. And lockdowns may have had a significant effect on people’s levels of histamine by keeping them indoors, ( out of the sun, with no holidays to top up, with resulting loss of vitamin D which would normally keep inflammation in check ), and by perhaps encouraging increased consumption of the higher-histamine foods which are usually the most expensive or only present in small quantities in restaurant dishes but somewhat cheaper/more affordable when bought in supermarkets.
With adequate exposure to ultra violet B from the Sun being our source of power to create our own vitamin D. Otherwise, we need supplement it via our diet. Not going out enough can therefore be contradictory to good health. Worth noting that other animals that spend time outside, such as grazing the fields, do the same thing – even through their fur, which UV B penetrates.
Did Saint Boris and his merry men expect a nation in perfect health, after he literally criminalised exercise? The consequences of the hallowed lockdowns are coming in thick and fast, just as we said they would.
As for gout: Hyancinth Bucket (lockdown snitch personified) once said “gout comes from an excess of good living”, when she made Richard pretend he had gout, instead of a mere fungus infection.
“Over-Eating and Lack of Exercise During Lockdown Has Triggered Huge Increase…” in illnesses, both physical and mental across much of the UK population.
It is important that the correct perspective is taken when the health of the community at large is under discussion.
Once you accept that many other health issues could be substituted for ‘gout’ it is nigh on impossible to refute the conclusion that all of this is intentional.
Stating the obvious but the government (and opposition) are clueless (or ambivalent) about health issues. Do they even have a policy on orthomolecular (nutritional) medicine? Of course they won’t, it’s not profitable enough to them.
But they probably have shares in the elastane/spandex/Lycra ® industry?
Reminds me of The Fast Show and ‘Does my bum look big in this?’
So nobody thought that sitting around, doing nothing but bingeing on delivered food, whilst boozing to excess would have a negative impact on their health? Truly, common sense is not very common.