
A recent study of deaths in U.S. students appears to show a declining rate of sudden cardiac deaths. The study included students who were registered with the National Collegiate Athletic Association, which organises intercollegiate athletics. Figure 1 shows the main findings. However, there are a number of points about this paper which raise doubts about the findings.
The authors had access to data from the following databases:
- NCAA resolutions list
- Parent Heart Watch database
- Prospective media report searches
- NCAA insurance claims
- National Centre for Catastrophic Sports Injury Research database
In the five years from 2004-2008 there were 55 deaths and nine cardiac deaths per year.
Over the 10 years from 2003/4 to 2011/12 there were on average 53 student deaths per year. The NCAA has a database of deaths but the only years publicly available are 2016, 2022 and 2023, which show the following:
- 2016: 71 students and 191 staff deaths
- 2022: 70 students and 231 staff deaths
- 2023: 68+ students and 285+ staff deaths
An honest scientist with access to these data would surely want to investigate the 50% rise in mortality between 2016 and 2023 among staff, but this was ignored. In fact, anyone wanting to understand the impact of Covid vaccines on sudden cardiac deaths would need a much bigger dataset. Epidemiologist Tracy Beth Høeg points out that, assuming vaccine uptake of 85%, this study was examining only 255,000 males, which is far too small to see an increase in mortality of between one in a million and one in 333,000, meaning we would expect zero to one deaths in a study this size.
It is odd that 2016 is the only historical year still available. Was it an outlier? Where are the other years?
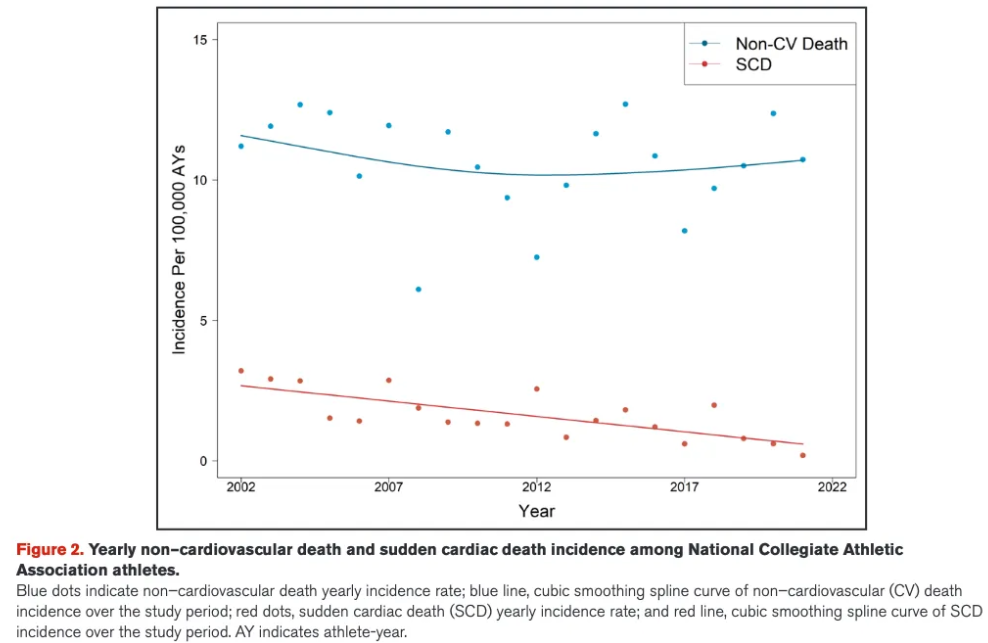
As to 2022 and 2023, why were student deaths so much higher than in the preceding years – around 70 compared to a historical average of 53? Have they just got better at recording the deaths? Were there more students registered? The authors are not clear on how many students were enrolled in each year and their characteristics. This is crucial as including more females and more athletes in low risk sports will skew the data. The overall trend downwards (see chart above) seemed to be to do with increasing numbers of females and low-risk sports being included as the rates for male basketball players remained high throughout the period.
Of the cardiac deaths, there were eight due to myocarditis over the whole period with only one post 2020. What is not clear is whether an athlete who received a diagnosis of myocarditis and had to end his or her athletic career as a result would still have been included in the NCAA database if he or she later died.
Tracy Beth Høeg also points out that the small rise in non-cardiac deaths among these athletes was not even commented on by the authors.
While it is encouraging that there was not a loud signal of harm among these U.S. athletes, the small dataset used means it cannot be used to dismiss concerns based on numerous much larger datasets.
Conflicts of Interest?
Virtually no scientific studies are completed these days that do not in some way link directly or indirectly to pharmaceutical funding. I was interested therefore to see this stated boldly on the final page of the paper: “Sources of Funding: None.”
Wow. A completely unbiased piece of scientific research! Amazing!
Or maybe not.
When one takes more than a cursory glance, the ‘Acknowledgements’ and ‘Disclosures’ sections directly above and below the ‘Funding’ section tell a slightly different story (emphasis added).
Disclosures
Dr. Ackerman is a consultant for Abbott, Boston Scientific, Bristol Myers Squibb, Daiichi Sankyo, Invitae, Medtronic, Tenaya Therapeutics, Thryv Therapeutics, and UpToDate. Dr. Ackerman and Mayo Clinic are involved in an equity/royalty relationship with AliveCor, Anumana, ARMGO Pharma, and Pfizer. None of these entities was involved in this study.
Dr. Baggish has received funding from the National Institute of Health/National Heart, Lung, and Blood Institute, the National Football Players Association, the American Heart Association, and the American Medical Society for Sports Medicine to study cardiovascular outcomes among elite athletes and receives compensation for his role as team cardiologist from the U.S. Olympic Committee/U.S. Olympic Training Centres, U.S. Soccer, and U.S. Rowing.
Dr. Drezner has received funding from the American Medical Society for Sports Medicine, the American Heart Association, and the National Centre for Catastrophic Sports Injury Research.
Dr. Harmon has received funding from the American Medical Society for Sports Medicine, Football Research, Inc, the Pac-12, and the American Heart Association.
Dr. Kucera is supported by funds from the National Centre for Catastrophic Sports Injury Research.
Acknowledgments
This research is supported, in part, by the National Centre for Catastrophic Sports Injury Research at the University of North Carolina at Chapel Hill. National Center for Catastrophic Sports Injury Research is supported by the National Collegiate Athletic Association, the National Federation of State High School Associations, the American Football Coaches Association, the National Athletic Trainers’ Association, the National Operating Committee on Standards for Athletic Equipment, and the American Medical Society for Sports Medicine. Conclusions drawn from or recommendations based on the data provided by the National Centre for Catastrophic Sports Injury Research are those of the authors and do not necessarily represent the official views of the National Centre for Catastrophic Sports Injury Research or any of the supporters. The authors thank the Parent Heart Watch and National Collegiate Athletic Association for data collection and Kyle Conley for work on this study.
By way of translation, ‘supported’ here means ‘receives money from’. Which essentially means ‘is funded by’. This is a deeply dishonest trick to give the illusion that the paper suffers no conflict of interest bias. We would pretend to be shocked, but as we know by now, this is de rigueur for The Science™. What is also well-known is that if Ackerman, Drezner & co. don’t find exactly what their ‘supporters’ want them to find, that ‘support’ may find itself evaporating overnight. Careers don’t tend to get a mega-boost from crossing Big Pharma.
The ‘Acknowledgements’ section is particularly compelling reading. If you were an institution involved in the mandating of these jabs as a condition of entry or continuing membership, you might be a tiny bit motivated to find ‘scientific’ evidence to prove that this vaccine mandate had not caused harm, particularly if, as is hypothesised, the harm was in some cases a fatal heart attack in a formerly young, super-fit individual. Nothing here is new, nothing here is surprising. But it continues to be our duty at HART to point out the dishonesty that is being promulgated as ‘science’ to try and prop up the increasingly fantastical idea that these injections were safe and effective.
Dr. Clare Craig is a diagnostic pathologist and Co-Chair of the HART group, which first published this article. She is the author of Expired – Covid the untold story.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
This whole system relies on two evils – plausible deniability and the facelessness of the corporate Wendigo. They will often say that no financial interest has leaned on them to go a certain way but their very existence is predicated on keeping schtum about most things and of course this is internalised by everyone within that organisation. Most journalists will say that no one tells them what to say but as Chomsky pointed out, they wouldn’t have high-paying journalistic positions if they didn’t accept the fundamentals implictly.
Look at the COVID on the spiritual level. I know you have an understanding of what it really means. I would say just remind everyone to stand still and contemplate because this really is the time for it. It is more than just the cliche of a crossroads. It is a fundamental parting of the ways which has long been predicted by indigenous soceties (the Australians predicted a run on toilet paper which would mark the beginning of the end of the era). The time that we are going into will be in many ways the time of the unthinking but imagine if the thinking found each other because of that time. That is where your heart should be. We can all so easily fall into despair but we shouldn’t despair all that is asked is that we affirm our radiance. In the future we will care about each others lives because we will have a greater understanding. We were all beguiled by the shadows on the wall when we look back at how we perceived the world. Given a hundred years of a scientifically-crafted Anglo-American propaganda model. it is a wonder that we have any dissent left at all.