
In the early summer of 2020, masks were introduced in the U.K. Thereafter, there was a mishmash of weird and wonderful measures that didn’t prevent further restrictive measures or lockdowns. According to Rishi Sunak’s statement to the Spectator, not even Cabinet Ministers were aware of the rationale for this merry-go-round.
As most of the important people making decisions, or at least communicating them, flip-flopped at approximately the same time on both sides of the Atlantic, were we treated to (or should we say, were we victims of) some clockwork change of course?
But why did this take place? Perhaps the question for Trust the Evidence is: on the basis of what new convincing evidence did the flip become a flop? We are unaware of any new high-quality evidence apart from the feardemic the flip-floppers induced.
Now that things have calmed down, we look closer at the efforts to retrofit the evidence to the policy decisions. Keith Duddlestone comments that some folks want to forgive, forget and move on. Some understandably want to do so, as they have suffered enough; others, though, are well aware that these measures will remain on the menu if we do not hold those responsible for their actions.
The reintroduction of masks will depend mainly on the politics of the day. More so the case in the U.S.: the CDC is back recommending face coverings in areas where hospitalisations are high, and some universities announced face coverings would be compulsory for staff and students on their campuses.
Because of the mismatch between policy and evidence, we promised to track the flip-floppers, escape artists, retrofitters and those who have just collected their honours and want to move on.
So, let’s start with the U.K. Health Security Agency (UKHSA). We have documented its dreadful reviews on masks that include the wrong type of evidence to answer the question, including just about anything its researchers could lay their hands on. The garbage in its reviews was presented in Parliament as evidence of effectiveness of mask use. It led us to question whether they had read some of the studies.
However, it now looks as if the UKHSA intends to update and enlarge its evidence dragnet. Now we are told:
There is a lack of strong evidence on the effectiveness of NPIs to reduce COVID-19 transmission, and for many NPIs, the scientific consensus shifted over the course of the pandemic.
Did you note the flip-flop? Consensus shifting, hey. Apparently, “there are specific limitations to the evidence-base for NPIs effectiveness”. Who’d have thought it?
The UKHSA has mapped available evidence by intervention and study design. The map is interesting. It is a cosmology of every non-pharmaceutical intervention (NPI) they can think of. The typology is unclear, but that is not the point. They called it an Evidence Gap Map.
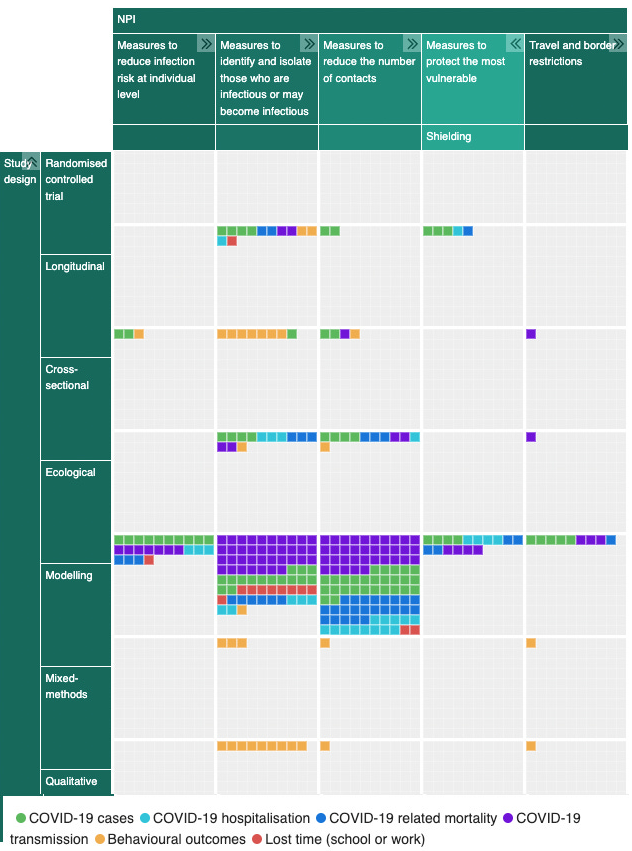
If you go to the page and click the arrows in the boxes at the top, you obtain a detailed list of interventions under each heading.
The map is part of a more detailed 91-page review of ‘What evidence exists of the effectiveness of the NPIs as implemented in the community in the U.K. to control the COVID-19 pandemic?’
The rationale for deconstructing the evidence solely to focus on the U.K. doesn’t make sense. There are certain situations where this might be appropriate. If the issue is genuinely setting specific, e.g. waiting list initiatives, or if the intervention is a U.K.-specific public health intervention alone. But masks are masks, and their deployment and effectiveness in developed countries should be the same as in the U.K.
The boxes in the map show the availability of evidence for each intervention and are almost all bare except for the model row. As no one seems to venture into conducting randomised controlled trials because of the politicisation of the whole issue, we wonder how the UKHSA plans to fill the boxes. With more models? With observational studies or ‘systematic reviews’ carried out by friendly and trustworthy academics carefully directed by the agency?
Or is UKHSA just playing draughts using a chequerboard of its own design? Whatever, it must get a move on, as more people are asking questions and getting fobbed off, like Philip Davies MP.
The UKHSA concludes the evidence was “primarily based on modelling studies (100 out of 151 studies) and there was a lack of experimental studies (two out of 151 studies)”.
It goes on to report that:
Whilst this body of evidence overall provides weak evidence in terms of study design (study designs at the lower end of the hierarchy of evidence such as cross-sectional studies are at higher risk of bias than studies at the higher end of the hierarchy of evidence such as RCT) and potentially in terms of study quality (although critical appraisal was not performed), the wider challenges of the pandemic should be acknowledged, including the limited resources that were available.
We did not perform a critical appraisal. Why? Because we didn’t have the resources. This is an astounding statement; it means the UKHSA doesn’t know how to do a critical appraisal.
Furthermore, it states:
It is also worth noting that the traditional evidence hierarchies and corresponding ‘low level of evidence’ and ‘low or very low certainty’ of the GRADE framework were developed to inform clinical practice where RCTs are feasible, and linear causal pathways are more often the norm.
For this reason, the ROBINs I tool was developed to assess the risk of bias in non-randomised studies of interventions. It’s only been available since 2016 and is the preferred method for Cochrane reviews.
UKHSA says the “next steps are to critically appraise and synthesise the evidence identified on the effectiveness of individual NPIs implemented in community settings to reduce the transmission of COVID-19 in the U.K.”
Despite a lack of resources at Trust the Evidence, we think we can do the job of critical appraisal for them as we’ve done in the past.
The UK Health Security Agency Review – our Trust the Evidence Critical Appraisal
- U.K. Government Evidence for Mask Mandates – an introduction
- Mystery studies
- Studies with non-representative populations
- Studies with obscure methods
- Studies with no blinding and no protocol
- Office for National Statistics – Part 1
- Office for National Statistics – Part 2
- Studies which shouldn’t have been in the UKHSA review
Dr. Carl Heneghan is the Oxford Professor of Evidence Based Medicine and Dr. Tom Jefferson is an epidemiologist based in Rome who works with Professor Heneghan on the Cochrane Collaboration. This article was first published on their Substack, Trust The Evidence, which you can subscribe to here.
Stop Press: The BBC reports this morning that face coverings are now needed in clinical areas of three hospitals in Leicester: Leicester Royal Infirmary, the Leicester General and Glenfield Hospital.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
They’ll simply decide that they weren’t done properly and needed to be longer, harder and more restricitive
Although possible they have absolutely no evidence that that would work either. They already know, if it makes an iota of difference, that lockdowns are ruinous to society. The longer the lockdown, the more ruinous. Whatever ‘they’ find and ‘they’ decide, I ain’t doing it, no matter the consequences. And I think I speak for many.
Amen
So typical of them
I don’t care whether lockdowns and masks “work” or not. I’m not doing them for the flu/a bad cold. Normal life is much more important.
Amen. I second that. The motion carries.
I do wonder if these quangos would be missed at all if they were obliterated (yes, I mean that literally) because they appear able to do nothing other than contribute to government’s effluent overspill.
I’ve noticed a marked increase in public mask wearing hereabouts in the last couple of weeks, regardless of actual evidence or politicised ‘consensus’ change. For some, the mindf*ck damage is in too deep. Sad.
I observed this very morning a lady in her car driving along with a mask on, her husband (presumably..) sat in the passenger seat with face uncovered. Could be an interesting conversation over breakfast..
Indeed. I keep seeing couples in the supermarket where one is bemaskec and the other not. I wonder whether they cohabit and did they travel to the shop in separate vehicles
I’ve not noticed where I live, but in 2020/21 there were quite a lot of people not wearing masks and I never suffered verbal abuse for not wearing a mask and wasn’t aware of anyone else being subjected to this. Apart from constantly voting SNP it seems like Scots have a certain amount of common sense.
They should have read the bsi-guide-for-personal-safety-equipment-0520 v1.4 June 2020. Remember that in the UK, most of the junk sold to the public were NOT classified as “masks” – indeed, they would have tiny labels that say no (if you had a magnifying glass to hand), so as to avoid being done under trading standards. In the BSI guide they were classed as “face covering” and it said that: “The manufacturer/seller must not call it PPE or a medical device nor make any claim that the product will provide protection to any specific individual ”, and “General product safety regulations (product must be safe i.e. non- toxic, non-choking etc) ”. In short, they were of no physical value at all.
I’ve still got a copy of that one. And I never bought any of them.
So, ‘surgical masks’ were they?
🙂
It comes to something when NHS hospitals have face nappy mandates for more of the year than when they have not enforced this violation of human rights. But facts don’t matter in Clown World, seemingly. Anyone here in Leicester? Stay healthy and stay out of hospital. You also have the bonus of not being ‘Matt Midazolam’d’
”People in some parts of Leicester’s hospitals will be required to wear face masks again after a rise in coronavirus cases among patients.
Face coverings are now needed in clinical areas of the Leicester Royal Infirmary, the Leicester General and Glenfield Hospital, senior medics said.
University Hospitals of Leicester NHS Trust (UHL) insisted the number of infections were “low”.
However, it said the step would protect, patients, staff and visitors.
UHL’s chief nurse Julie Hogg said: “We are constantly monitoring Covid-19 levels in our hospitals, and as a result we are reintroducing mask wearing in clinical areas.
“The number of patients testing positive for Covid remains low but has increased, and we are determined to ensure the safety of patients, colleagues and visitors to the hospital.
“Mask wearing is not mandatory in non-clinical spaces, such as offices, lifts, restaurants and corridors, but we will keep the situation under review.”
https://www.bbc.co.uk/news/uk-england-leicestershire-66988015.amp
The UHL Chief Nurse obviously knows the square roor of sweet FA about aerosol viral transmission. How the hell has she risen to this position of authority?!
I live in the Leicester area. I wonder what will happen if I need to go to hospital and refuse to wear their stupid muzzle. Will I be denied access? Denied treatment? What a world.
Yet more reason to look elsewhere for treatment and to take care of ourselves as a matter of urgency. How can these people be trusted with needles and scalpels if they think wearing a cloth over one’s mush will safeguard anyone.
The Conspiracy against “We, The People” was NOT a Theory. Shame on those who remained silent in 2020/2021. ALL Th evidence was already there.