I continue to suffer from the worst cough I’ve had in recent memory, but in the spirit of keeping the plague chronicle at least limping along until my health returns (I hope by the weekend), I draw your attention to an analysis of tweets discussing the risk of Mpox among children and young people in school by Benjamin Knudsen, Tracy Beth Høeg and Vinay Prasad.
The authors looked at Twitter accounts bearing medical or public health credentials tweeting about the (basically non-existent) risk that Monkeypox posed to children between May and October 2022. Their search criteria yielded a corpus of 262 tweets from 188 different credentialed accounts, 215 or 82% of which “overstated or exaggerated the risk of [Monkey]pox to children or young people in the school setting”. A mere 47 or 18%, meanwhile, managed to provide accurate information.
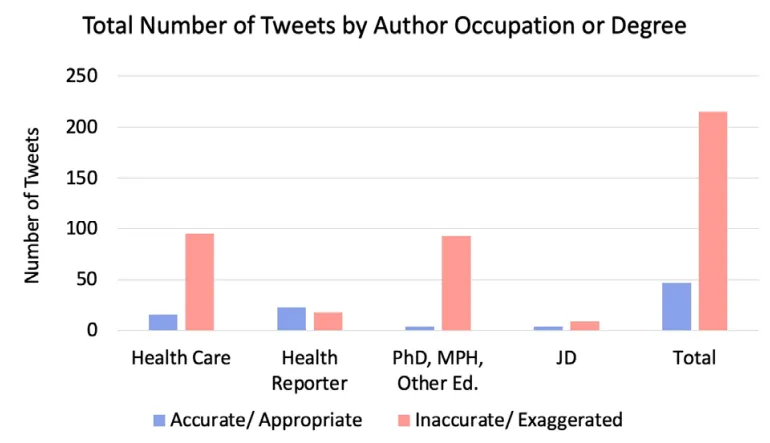
Healthcare professionals and academics – precisely those people held to represent ‘The Science’ – had the least accurate assessments; journalists, simply by managing to be merely hit-or-miss, achieved far higher reliability.
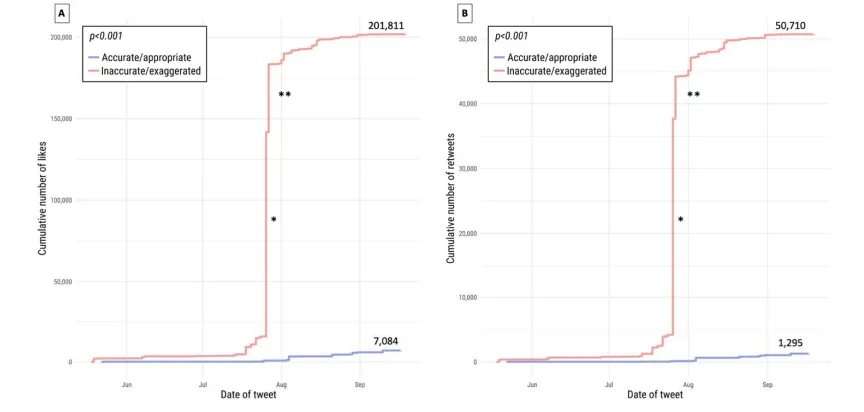
What is more, tweets categorised as “inaccurate” or “exaggerated” accumulated vastly more likes, as hysterical twitterers with medical credentials have vastly more followers.
Experts, far from being impartial oracles, are in fact self-interested careerists, and we all live in the world that Eric Feigl-Ding has made. Public health gurus and social media virus understanders only have relevance when people are panicking, and exaggerating the risks that viruses pose to children is one of the simplest ways to get people to panic. It’s also, unfortunately, one of the most harmful and destructive messaging strategies anybody could imagine.
This article originally appeared on Eugyppius’s Substack newsletter. You can subscribe here.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
In other news:
The C1984 was a Scam.
Yawn.
Meanwhile…CDC warns of another outbreak of Monkeybollox, also letting slip how crappy those smallpox vaccines were. In other words; Pride is coming up and should carry a health warning for an uptick of an STD which is of no concern to those of us who don’t partake of ‘butthole surfing’.
https://rumble.com/v2oenka-cdc-warns-of-new-mpox-cluster-w-most-cases-in-the-fully-vaccinated.html
I think I’ve even encountered someone with moneypox when it made headlines last year. At least, one of the They can pry my mask from my cold, dead face! M&S counter ladies had some very ugly looking lesion on her hands. Not willing to trust in her mask protecting me from that, I actually used the hand sanitizer station on exit on this occasion.
The thing that gets me with this particular STD though is, and surely this is stating the bleeding obvious, why not just wear a condom?
“Hmm, a double dose of a proven ineffective vaccine which is all risk and no benefit or…stick on a ‘Johnny’.. This is a real tough one, I’m gonna have to sleep on it.”
This is a real tough one, I’m gonna have to sleep on it.” 


It’s not really a STD. Transmission can happen when people come into physcial contact with open lesions on the extremities of other people. The chances for this to happen during everyday interactions is slim. But a lot of people having anonymous group sex in a darkened room is obviously a different story.
It may not be an STD in the classic sense, but do a basic search and you will find that by far and away the mode of transmission is via sex and the population affected are gay men. Now, obviously one should avoid having close physical contact with anyone who has lesions but surely a common sense precaution which would mitigate your chance of getting infected would be to wear a condom.
”We report 528 infections diagnosed between April 27 and June 24, 2022, at 43 sites in 16 countries. Overall, 98% of the persons with infection were gay or bisexual men, 75% were White, and 41% had human immunodeficiency virus infection; the median age was 38 years. Transmission was suspected to have occurred through sexual activity in 95% of the persons with infection. In this case series, 95% of the persons presented with a rash (with 64% having ≤10 lesions), 73% had anogenital lesions, and 41% had mucosal lesions (with 54 having a single genital lesion).”
https://www.nejm.org/doi/full/10.1056/NEJMoa2207323
Transmission of monkeypox virus occurs through large respiratory droplets, close or direct contact with skin lesions
[…]
Skin lesions were noted in 95% of the persons. The most common anatomical sites were the anogenital area (73%); the trunk, arms, or legs (55%); the face (25%); and the palms and soles (10%).
This adds up to 163% which means most of the 73% also had lesions elsewhere. In particular, 90% of the members of the observed group had lesions on trunk, arms, legs, face, palm or soles which means these are actually more common than anogential lesions. That this mostly affected gay men is due to a particular hobby that’s common among them (reportedly), namely, partaking in sex orgies with strangers[*]. Moneypox would equally well spread in other prolonged close-contact activities of naked people.
This is an observational study of 528 people located all around the globe (from 16 countries on five continents) and the only real conclusion which can be drawn from such a sample is that human <-> human transmission of moneypox is exceedingly rare. Which suggests that neither droplet nor fomite transmission (mentioned as possibility) contribute significantly to it, IOW, that both are likely Must happen! conjectures inserted to justify masking, distancing and sanitizing, just as with COVID.
[*] Why that’s supposed to be called love is an interesting question.
Stop putting your willy into another man’s bum. There you go, no more apespot.