Has COVID-19 caused excess deaths? This might seem an odd question, as most people do not doubt that the answer is yes. However, a growing number on the sceptical side of the aisle have been questioning this recently. This is not necessarily because they don’t believe in viruses – most of them do – but sometimes because they think there is nothing special about SARS-CoV-2 and invariably because they think interventions such as lockdowns, faulty treatment protocols and vaccines are responsible for any deaths out of the ordinary.
The first thing to be said in response to this is that there definitely is something special about SARS-CoV-2. Namely, that it is the only known SARS-like virus with a furin cleavage site – likely a feature it was given in a lab – which makes it unusually infectious. This essentially makes it like SARS-1 but far more transmissible.
A second thing to underline is that no one has yet shown any convincing relationship between policy interventions and deaths. Studies based on real-world data rather than modelling show that restrictions made little or no difference to outcomes. Here are five examples:
- “Full lockdowns and wide-spread COVID-19 testing were not associated with reductions in the number of critical cases or overall mortality.” “A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes” by Rabail Chaudhry, George Dranitsaris, Talha Mubashir, Justyna Bartoszko, Sheila Riazi. EClinicalMedicine (Lancet) 25 (2020) 100464, July 21st, 2020.
- “We find that shelter-in-place orders had no detectable health benefits, only modest effects on behaviour, and small but adverse effects on the economy.” “Evaluating the effects of shelter-in-place policies during the COVID-19 pandemic” by Christopher R. Berry, Anthony Fowler, Tamara Glazer, Samantha Handel-Meyer, and Alec MacMillen, Proceedings of the National Academy of Science of the USA, April 13th, 2021.
- “Stringency of the measures settled to fight pandemia, including lockdown, did not appear to be linked with death rate.” “Covid-19 Mortality: A Matter of Vulnerability Among Nations Facing Limited Margins of Adaptation” by Quentin De Larochelambert, Andy Marc, Juliana Antero, Eric Le Bourg, and Jean-François Toussaint. Frontiers in Public Health, November 19th, 2020.
- “Comparing weekly mortality in 24 European countries, the findings in this paper suggest that more severe lockdown policies have not been associated with lower mortality. In other words, the lockdowns have not worked as intended.” “Did Lockdown Work? An Economist’s Cross-Country Comparison” by Christian Bjørnskov. CESifo Economic Studies March 29th, 2021.
- “While small benefits cannot be excluded, we do not find significant benefits on case growth of more restrictive NPIs.” “Assessing Mandatory Stay‐at‐Home and Business Closure Effects on the Spread of COVID‐19” by Eran Bendavid, Christopher Oh, Jay Bhattacharya, John P.A. Ioannidis. European Journal of Clinical Investigation, January 5th, 2021.
This means of course that lockdowns failed utterly as disease control. But it also means that no relationship was observed with increased deaths either. It is not the case that the places which imposed the harshest restrictions had the most deaths, nor that the places which eschewed restrictions had fewer deaths.
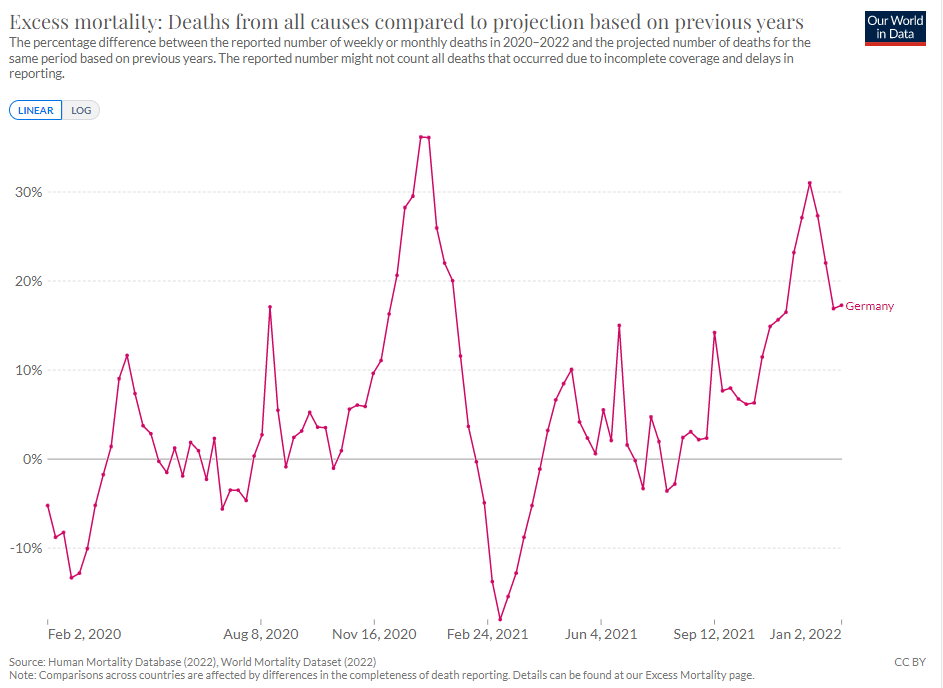
Consider Sweden: light restrictions in spring 2020, but a sizeable wave of excess deaths. And Germany: strict measures in spring 2020, but few excess deaths – though considerable excess in later waves. South Dakota imposed no restrictions in spring 2020 and had no excess deaths, yet then experienced a huge wave of mortality during the autumn (see below). Florida lifted all statewide restrictions in autumn 2020 and had a relatively mild winter, yet then saw a large wave of deaths the following summer. As per the above studies, nothing about these outcomes is explained by whether they did or did not have restrictions.
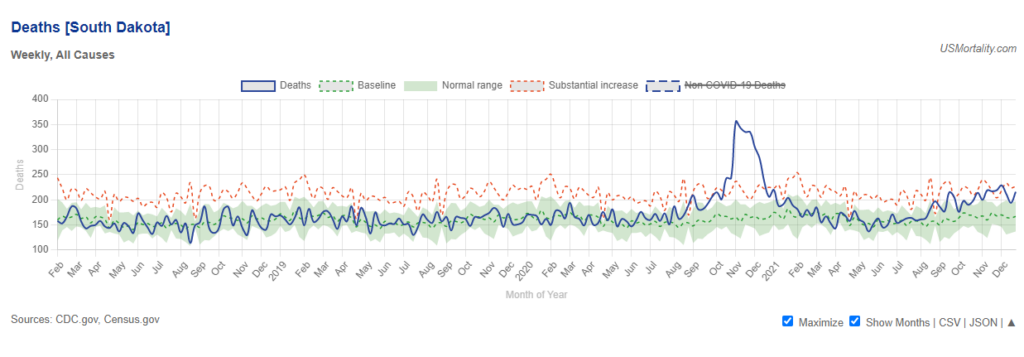
If all or most excess deaths during the pandemic were caused by interventions – and let’s bring treatment protocols into this as well now – then why did Germany and South Dakota have little or no excess deaths during spring 2020, but then considerable excess deaths later in the year? Why would interventions not kill in the spring but then do so in the autumn?
Some commentators blame overuse of ventilators for killing large numbers of people, and undoubtedly these killed some who would have survived otherwise. But the ventilator panic was entirely a first-wave phenomenon, spawned by ill-conceived treatment protocols out of China; it was over by June 2020. Germany had the same faulty Chinese treatment protocols as anywhere else, but it didn’t see a large spring wave like Lombardy, New York or London. But then later in the year, once people had stopped overusing ventilators, that’s when Germany and South Dakota saw their deaths. How can treatment protocols explain this any more than social interventions?
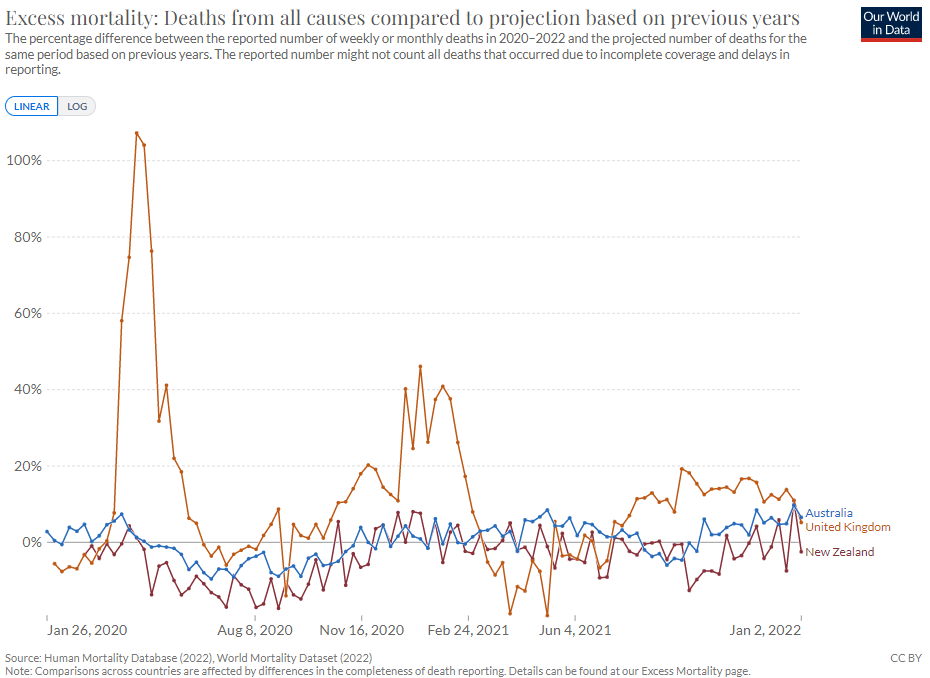
Other counterexamples include Australia and New Zealand, which imposed long and extreme restrictions and had the same faulty treatment protocols as anywhere else, but saw no spike in excess deaths in 2020 and 2021.
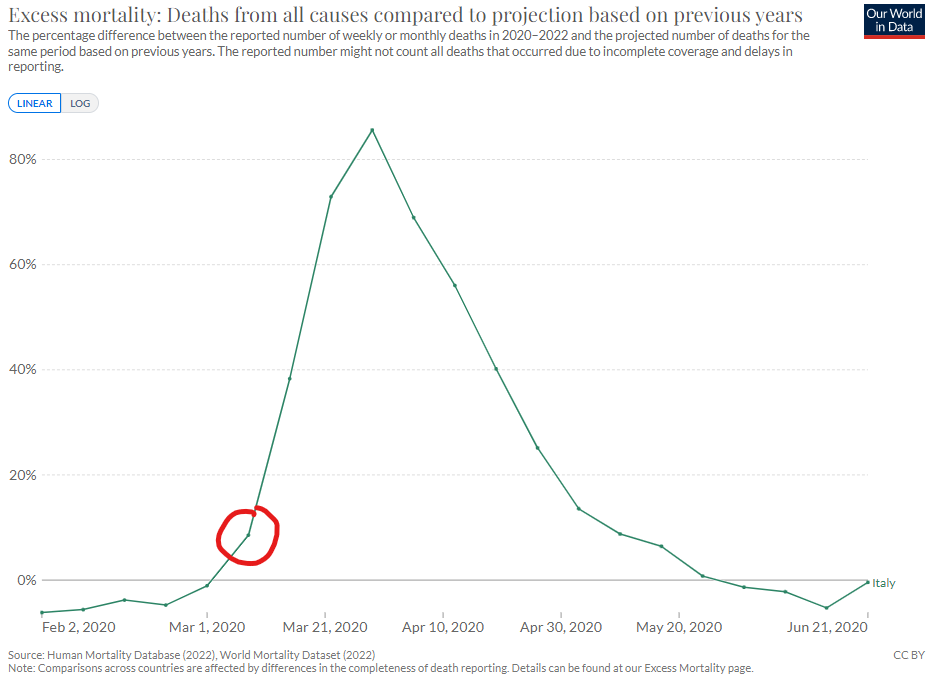
Dr. Jonathan Engler has stated that there is “no excess death observable until the emergency is declared” and he and others take this as further evidence that it is the emergency response that caused the excess deaths. But as a point of fact it is untrue that there is “no excess death observable until the emergency is declared”. Italy’s lockdowns started on March 8th but there were already excess deaths in the week prior to that (see below) and the ICUs were already full. It was the high number of deaths and hospitalised patients that prompted the Government to impose the lockdown.
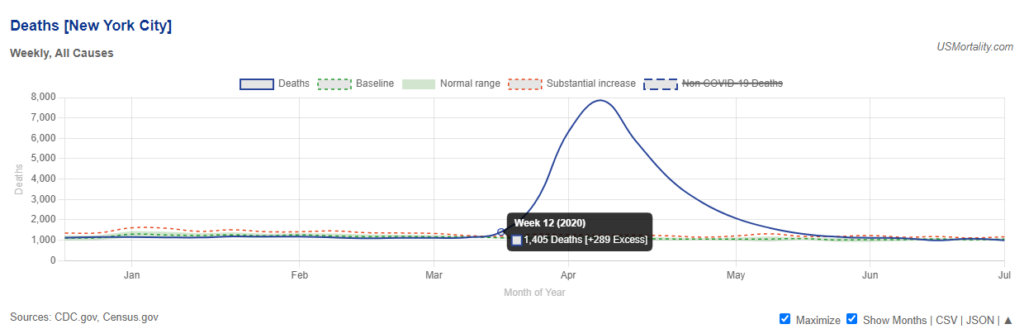
Likewise, in New York City there were excess deaths in the week ending March 22nd (and again, ICUs were full), but the city didn’t lock down until the end of that week. The restrictions in these places were imposed in response to the rise in deaths and hospitalisations.
Dr. Engler asks why there was a lack of excess deaths before March 2020 when the virus had been circulating for months. The short answer is that this is likely a result of the virus mutating and not having yet reached the most transmissible, immune-evasive form in each context. Spread before February 2020 was at a low level and there were no explosive outbreaks.
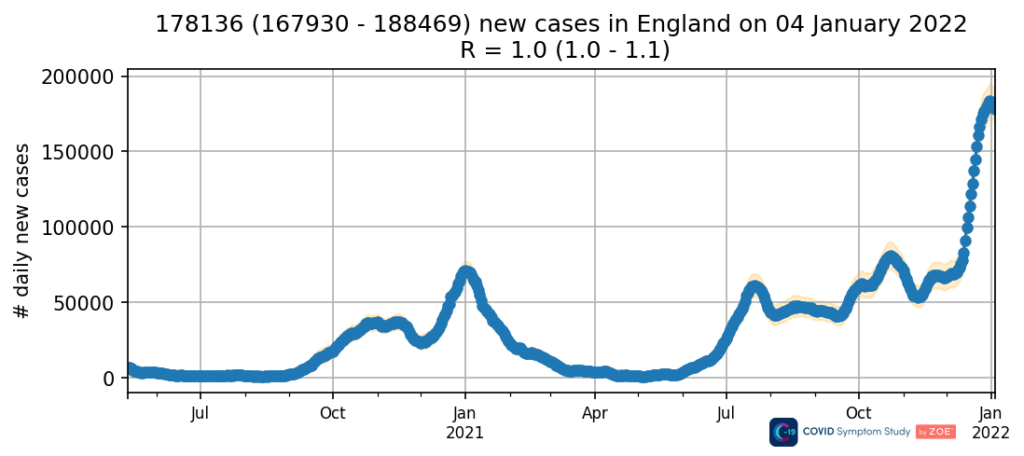
Taking a step back, we need to recognise why it is so widely believed that a virus is responsible for most of the excess deaths. It’s not based on any single, fallible measure such as PCR testing, but on a host of factors that together build a clear picture. These factors are symptoms, PCR test positivity, LFT positivity, sequencing of viral genomes, hospitalisations, ICU admissions, Covid deaths, excess deaths and antibodies, which all rise and fall together during a Covid wave. This happens in each wave and in every country and region of the world, and the pattern always repeats. There is no other explanation for why this would happen. Let me illustrate with England, but the same could be shown for any country or region.
Here are data on Covid-like symptoms from the ZOE app.
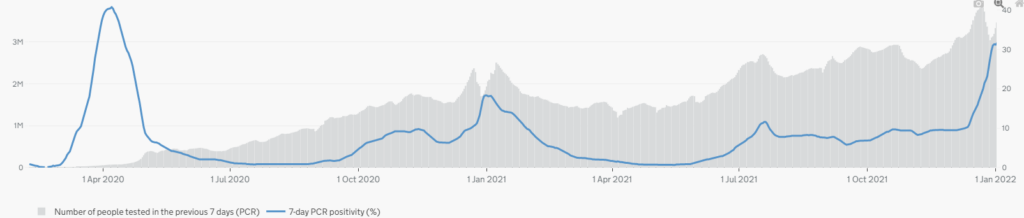
Here is PCR positivity (percentage of PCR tests that are positive).
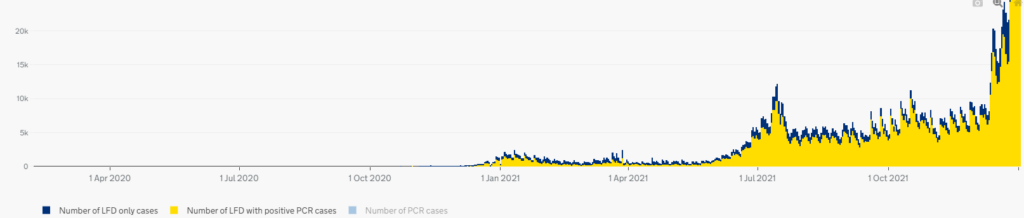
Here is the number of positive Lateral Flow Tests (LFTs), which were introduced towards the end of 2020.
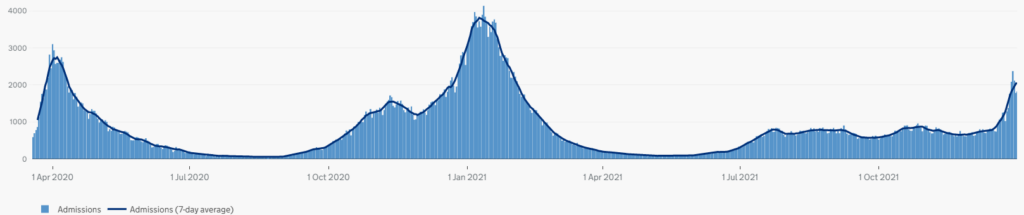
Here are hospitalisations.
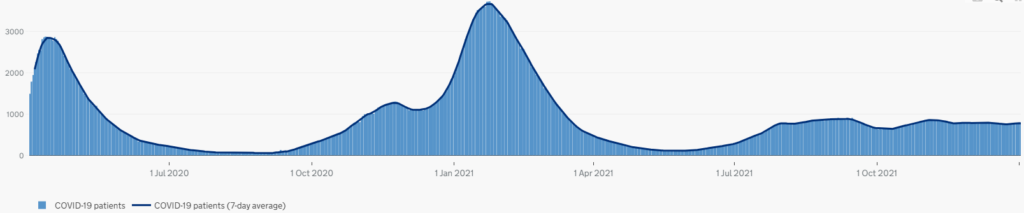
Patients in mechanical ventilation ICU beds.
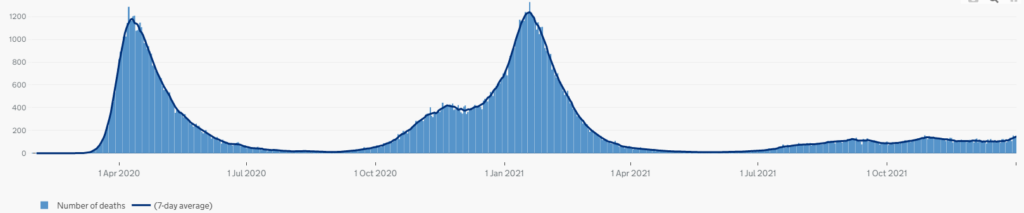
Covid deaths (where Covid is mentioned on the death certificate as a cause of death).
Excess mortality.
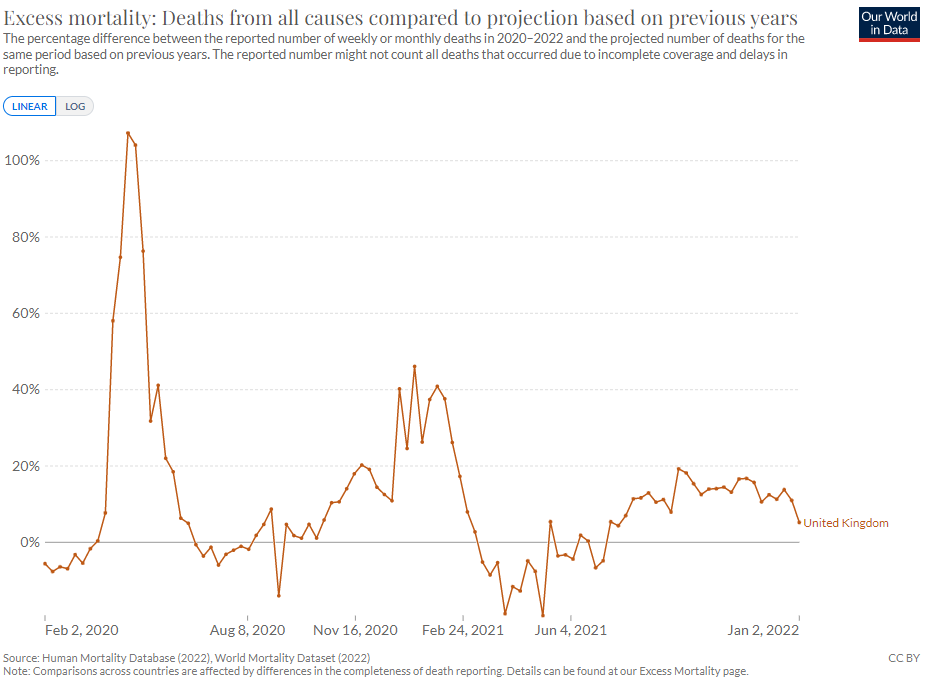
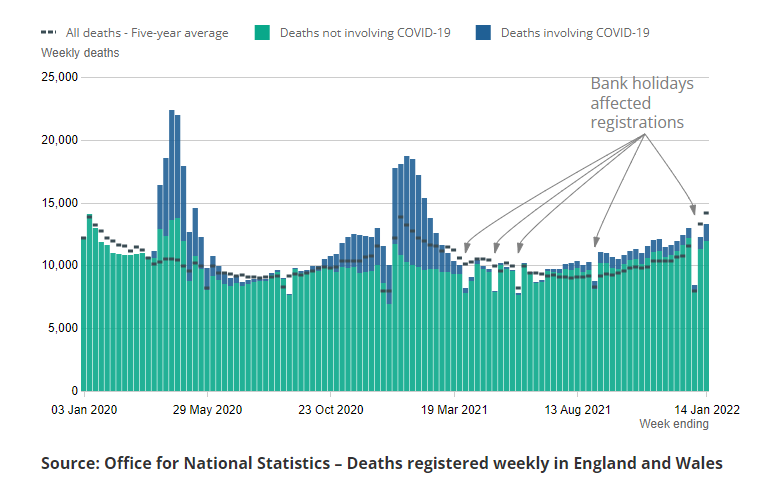
Note that the sharper peak in excess deaths in the first wave compared to the second is mainly a result of the baseline in winter being higher, as shown below.
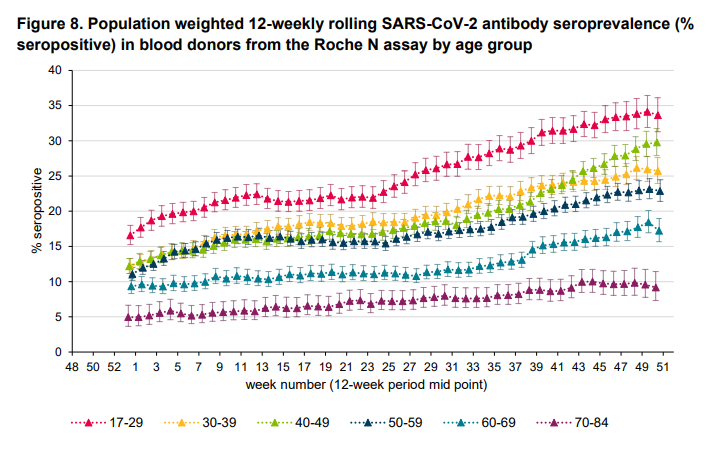
Here are antibodies (for 2021).
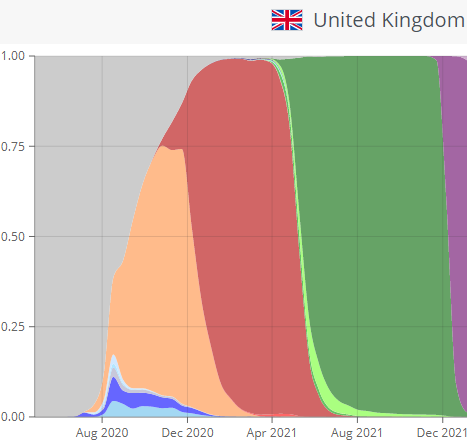
Here are the data from sequencing of viral genomes, with variants corresponding to each wave.
The close correspondence between these graphs is I’m sure obvious to anyone. The significance of that correspondence is that these are all showing different aspects of the same phenomenon, namely a viral outbreak that is causing a closely correlated rise in symptoms, PCR positives, LFT positives, variant genome detection, hospitalisations, ICU admissions, antibodies and deaths. No other cause for this multifactorial phenomenon is plausible. Thus we must conclude that excess deaths during the pandemic are to a large extent explained by the effects of the virus that is causing all these things. Some excess deaths will no doubt be due to interventions and faulty treatment protocols, and the impact of these should be investigated. But most will be due to the virus.
We must, of course, as sceptical inquirers, follow the evidence where it leads and challenge received wisdom. Nonetheless, I have been watching the recent rise of the Covid-doesn’t-cause-excess-deaths theory among sceptics with a growing sense of alarm. The views can be extreme. For instance, Denis Rancourt, whose analysis is often cited in defence of the view, states:
We conclude that a pandemic did not occur. We infer that persistent chronic psychological stress induced by the long-lasting Government-imposed societal and economic transformations during the Covid-era converted the existing societal (poverty), public-health (obesity) and hot-climate risk factors into deadly agents, largely acting together, with devastating population-level consequences against large pools of vulnerable and disadvantaged residents of the USA, far above pre-existing pre-Covid-era mortality in those pools.
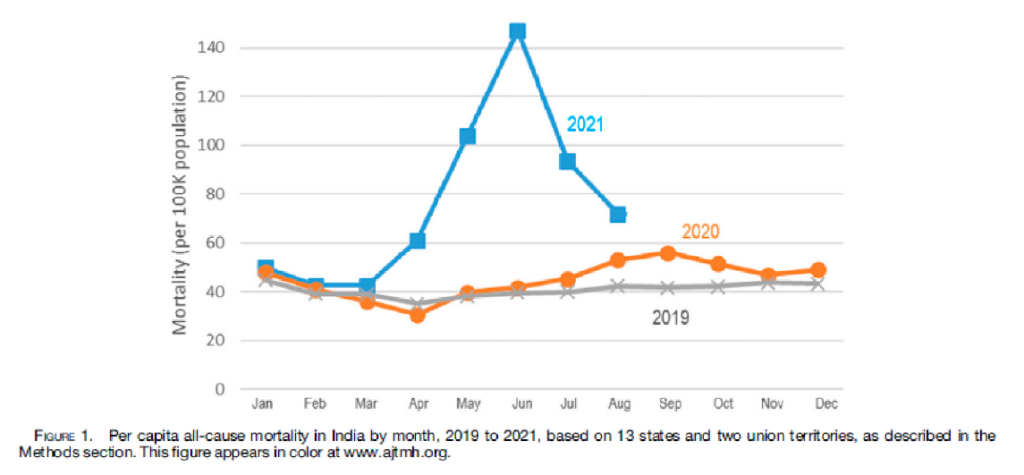
In more recent articles, Dr. Rancourt has begun arguing that all excess deaths since 2021 are caused by the vaccines. For instance, Dr. Rancourt claims that all the excess deaths in India’s large Delta wave were due to the vaccines, giving a vaccine fatality rate of 1%. But in fact the correlation between vaccine doses and excess deaths in 2021 in India is very weak, and the graphs in his own report make this plain.
Here are excess deaths in India:
And here are vaccine doses.
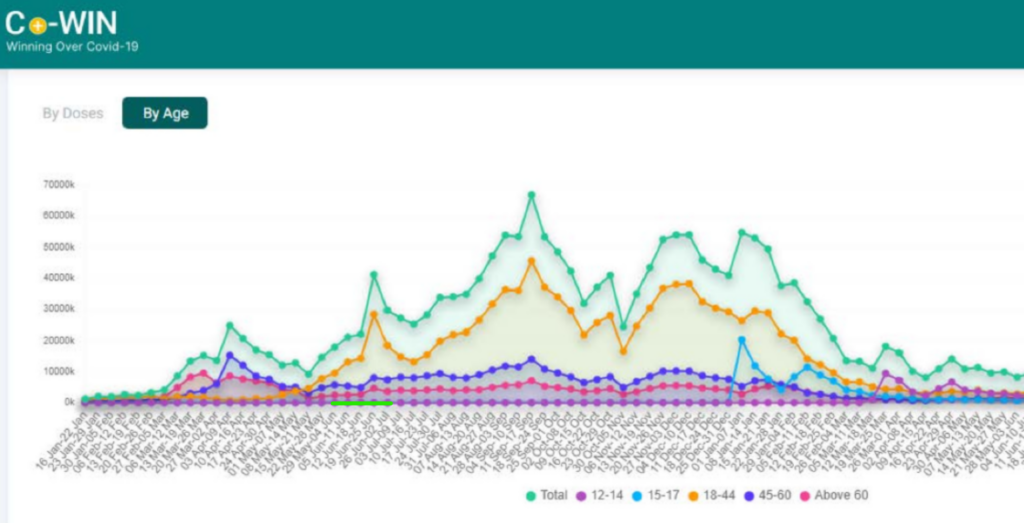
Note the peak month for deaths is June, which is a month of little note for vaccines (see green horizontal line). There is no obvious relationship here at all, and certainly no warrant for supposing all the Delta wave deaths were vaccine deaths. While we know from other data the Covid vaccines are injuring and killing people, this is not something that can be easily seen in correlations with excess deaths.
Dr. Engler has argued that “it was the manner in which healthcare was delivered which was relevant to the death rate, not the spread of a virus” and his analysis has been picked up by others. Dr. Jessica Rose has stated that “what has taken place over the past few years is government-assisted termination of our elderly using such tools as the injections themselves, lethal cocktails of respiration depressing drugs upon declaration of ‘Covid positive status’, improper do not resuscitate (DNR) declarations and use and neglect (starvation and dehydration)”. It’s unclear how much of the excess deaths these analysts regard the non-viral causes to be responsible for, though the way they write seems to suggest much or all of it.
I agree that we need to look into the extent to which interventions may have made things worse. But it’s essential, for our own credibility and fidelity to the evidence, that we keep this in perspective. The main thing driving excess deaths over the last three years (well, 2020 and 2021 at any rate, 2022 is less clear) is the new SARS-like virus that was made highly infectious in a lab somewhere. It’s important to acknowledge this because the evidence for it – symptoms, test positivity (of two types), genomic analysis, hospitalisations, ICU admissions, deaths and antibodies – is so clear that denying it is a fast-track way to becoming instantly discredited in the eyes of anyone outside the small bubble of sceptics who have spent too long staring at graphs and playing with spreadsheets. If we want to be taken seriously in our reasoned, evidence-based opposition to lockdowns, masks, experimental vaccines and so on, then we don’t need to go making it easy for our enemies to smear and cancel us because we’ve started arguing that the waves of deaths that invariably accompany waves of infections are not in large part caused by a virus.
Update: This article has been corrected. An earlier version incorrectly implied that SARS-1 did not spread via aerosols.













To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.