
Recently the Joint Committee on Vaccines and Immunisations (JCVI), the body responsible for recommending which vaccines are appropriate for which individuals in the U.K., decided that healthy individuals under the age of 50 should no longer be offered the Covid vaccines. This decision appears to have been made based on a multitude of factors, including the facts that the vast majority of the population have now had Covid (so no need to provide them with the immune stimulation given by the vaccines) and that Omicron variants of Covid appear to be rather less likely to result in hospitalisation, compared with prior variants.
This decision could well be considered as being long overdue – indeed, I consider it rather alarming that this seemingly evidence-based decision was made in early November, yet the JCVI only bothered getting around to telling the population about its deliberations nearly three months later. There will have been many thousands of individuals, many considerably younger than 50, who were persuaded to get their booster vaccination after early November when even the JCVI thought there was very little need for them to receive this medical product. I consider this apparent laziness in keeping the population informed to be rather dubious from a medical ethics point of view.
Furthermore, I note that even though the JCVI’s own deliberations have resulted in the conclusion that the Covid vaccines will offer the healthy young very little in the way of benefit, the report’s authors nevertheless insist on mentioning how awful it is that some in the population have not received their primary course of vaccination – an inoculation that still targets the original Wuhan strain which has effectively been extinct for over two years at this point. “Appropriate and adequate communication should be provided… to optimise update among those who are eligible but have yet to receive the offer of vaccination,” they write.
What’s worse, I’ve even seen information from the Health Minister (a qualified solicitor with a degree in history) informing people that the time available to get their shot is running out and that they need to hurry to get jabbed.
This isn’t a limited-time offer like the marketing from an online sofa warehouse; the JCVI now considers that the vaccines don’t offer benefit to the non-vulnerable. It is thus inappropriate to encourage people to hurry to get their jab as if it’s a matter of ‘when they’re gone they’re gone’.
What is particularly interesting about this latest JCVI announcement is that it has included in an appendix to the main document some data, provided by the UKHSA, to support its decision in the form of a calculation of the number of vaccinations that are required to prevent each hospitalisation. The numbers-needed-to-vaccinate per hospitalisation prevented given in the appendix appear not particularly to support the use of the vaccines; this point has been covered in an excellent series of tweets by Dr. Clare Craig.
What worries me more is the data upon which the calculations were made. These data appear at first glance to be plausible, but I have several specific concerns about their quality.
Firstly, the authors have not declared the population estimate which they’ve used to move from raw hospitalisation data to the per-million rates that they’ve included in their table.
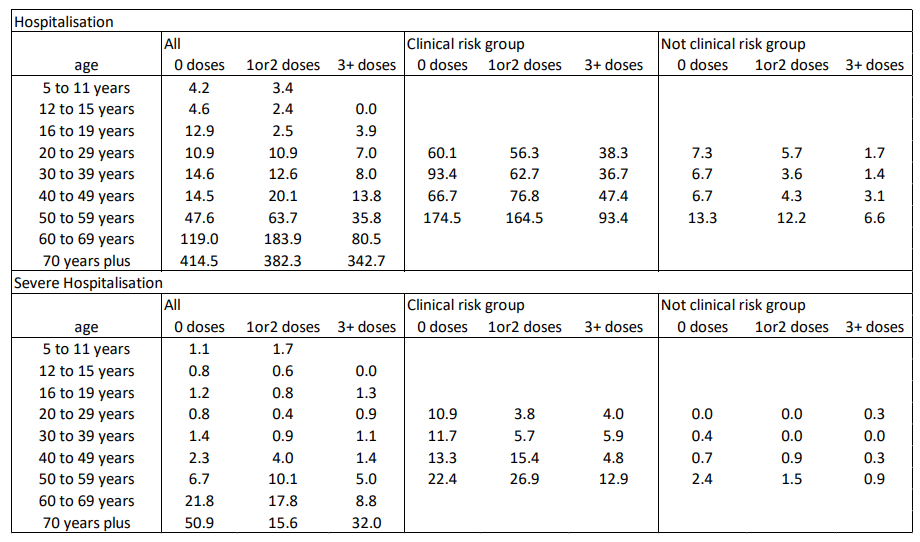
I’ve made this point numerous times previously, but in short there is no formal count of the number of unvaccinated individuals in the U.K. – this is calculated by subtracting the number of individuals that have received at least one dose of any Covid vaccine from the total number of individuals in the U.K. Unfortunately, the Government doesn’t have a good understanding of the actual numbers of people in the U.K. (which is astounding in itself), only various estimates of the population. The lowest population estimate is consistently that offered by the ONS. If they’re using the ONS population estimate – and the UKHSA does so like to use the ONS population estimate – then their calculations will suggest a higher hospitalisation rate in the unvaccinated compared with that reached using other population estimates. I estimate that a more realistic population estimate could easily remove any differences between unvaccinated and vaccinated in Table 1 or even result in the unvaccinated having lower admission rates. Note that they say they’re using NIMS as their data source, but that appears only to be used to identify the vaccination status of those in hospital – there still needs to be a population estimate to calculate the population rates and they do not state that they use the NIMS estimate for this purpose.
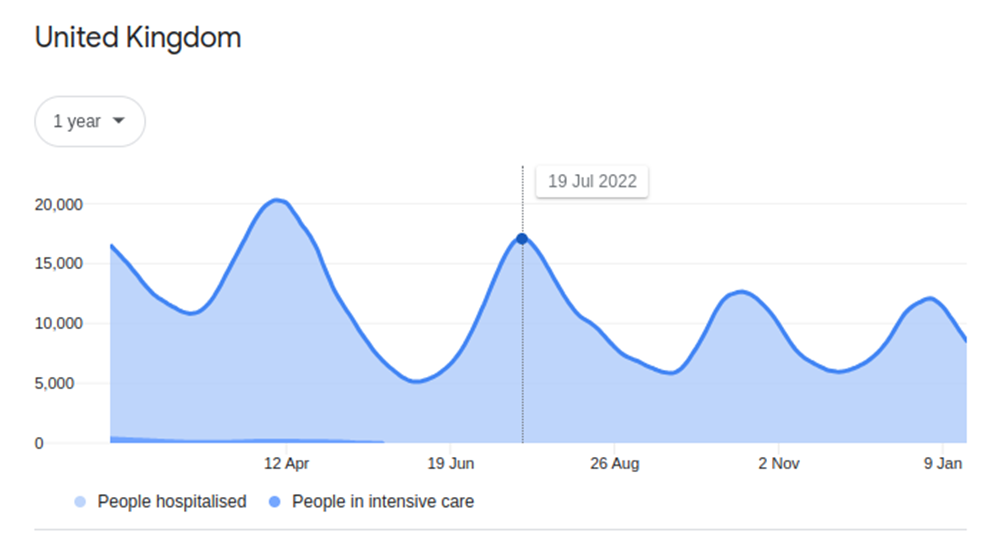
Secondly, they’re using July 2022 as their ‘example’ month, upon which their whole calculation of ‘numbers needed to vaccinate’ is based – this was a high month for hospitalisations in the U.K. and wasn’t representative of the average across the year. Their analysis appears to assume that the July hospitalisation rates were maintained across the year, thus using July’s hospitalisation numbers as their basis should result in a lower – or more favourable to the pro-vaccine position – estimate for numbers-needed-to-vaccinate to prevent each Covid hospitalisation.
Third, their ‘numbers needed to vaccinate’ table is based on vaccine effectiveness data from “other studies”. These appear to be mainly based on the Test-Negative Case-Control (TNCC) methodology – for the sake of the readers’ sanity I won’t delve into my criticisms of TNCC in this post, except to state that it can give misleading estimates of vaccine effectiveness if the vaccines also increase the risk of infection with other, similar, diseases (e.g., the ‘worst cold ever’).
Fourth, the JCVI release suggests that its vaccine effectiveness data were from when the Omicron variant was comprised of the BA.1 and BA.2 variants, which the bivalent booster doses supposedly targeted – thus it would be reasonable to imagine that the vaccines would have a worse performance against more recent variants, which have further escaped vaccine derived immunity.
Fifth, the JCVI states that the actual vaccine effectiveness data used in the calculation were from the UKHSA’s Vaccine Surveillance Report week 44 (November 4th 2021), but that VSR didn’t contain those figures – indeed, the Omicron variant hadn’t been identified at that point in 2021. Quite where the JCVI got the data to populate its table of vaccine effectiveness is unclear – I suspect that the vaccine effectiveness estimates were provided by the UKHSA, based on data contained in some of the references given in later Vaccine Surveillance Reports but not actually directly taken from these other sources. Whether its chosen vaccine effectiveness figures were corrupted by the UKHSA’s enthusiasm for the Covid vaccines remains open to question.
The situation outlined in the points above would have the effect of decreasing the numbers needed to be vaccinated to prevent each hospitalisation given in Table 3 and 4 of the JCVI appendix document.
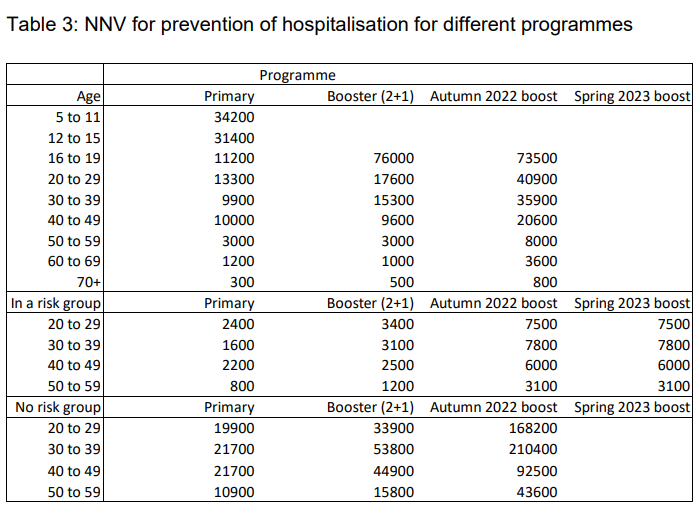
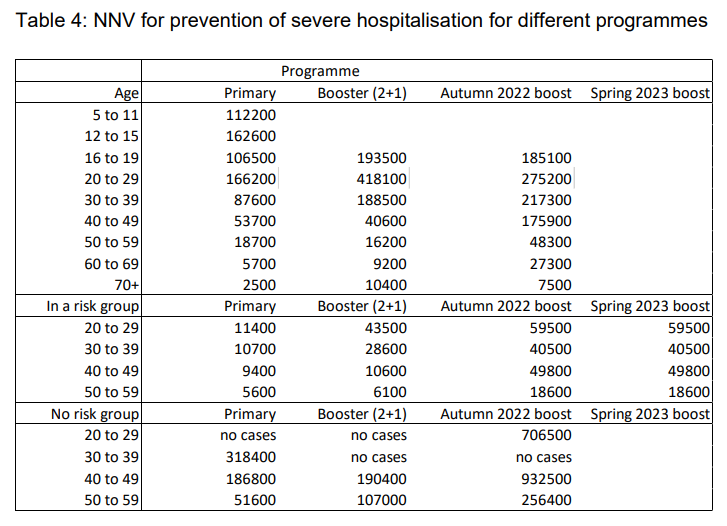
That is to say, if the JCVI used a more realistic population estimate, had based its calculation on an ‘average month’ for hospitalisations and had used more realistic estimates of vaccine effectiveness then its estimate of the numbers-needed-to-vaccinate would have been even less supportive of the vaccines than the marginal (at best) estimates that it has calculated.
There’s also no consideration at all of the mismatch between the estimates of vaccine effectiveness in Table 2 and the real-world data in the first table.
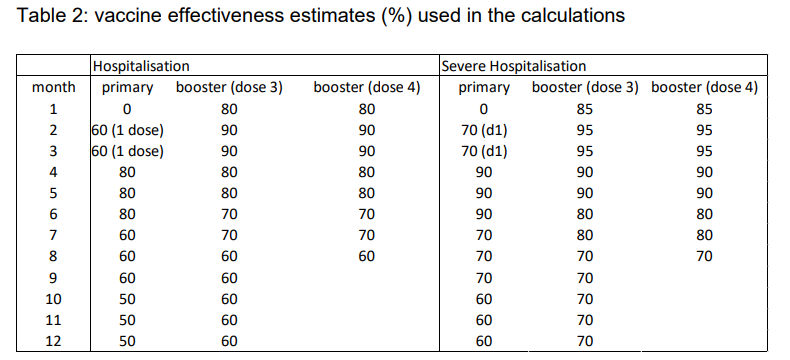
The assumed vaccine effectiveness suggests that the injections are preventing a fair proportion of hospitalisations, particularly in the first six months after vaccination (which would have been most of 2022 for older people given the enthusiasm for vaccinations last year). However, the real world data given in Table 1 suggest that the vaccines aren’t performing this well. A normal data scientist would ask questions here, but they merely state their usual “do not use these data to estimate vaccine effectiveness”. The report also states that the unvaccinated were probably doing surprisingly well because of prior infection; surely if this were the case then it would be a very important factor and shouldn’t be simply explained away. As it stands I’d suggest that nearly everyone in the U.K. gained ‘prior immunity’ in 2022, regardless of vaccination status, and so this wouldn’t have been an advantage unique to the unvaccinated.
Beyond the criticism above relating to the numerical data in the JCVI document, I believe that there are additional shortcomings. Firstly, there is no consideration of the impact of the vaccines on Covid-disease below the hospitalisation threshold. My fear is that the vaccinated are getting frequent reinfections with ‘nuisance symptoms’ but not ending up in hospital (merely feeling miserable for a week or perhaps longer).
Secondly, there’s no consideration at all of side-effects, which appear to be a non-trivial risk. The JCVI should have been undertaking risk-benefit analyses for the vaccines, but instead it has only considered the supposed benefits. Even when ignoring the risks, it has still decided that the vaccines don’t offer any substantive benefit to the healthy young. One can only guess at how negative its recommendations would have been if it had included risks in its analysis. But, of course, it appears that official bodies are not allowed to even mention the slightest possibility of there being any risks associated with the vaccines, and when pushed will only begrudgingly accept that there is a very very small risk of very very rare side effects (but only myocarditis and thrombosis, and anyway most people have a complete recovery armed only with a paracetamol and a day off work).
To summarise: the recent JCVI document appears to fall short of what is required of our medical regulators. Once again, one of our official medical agencies has had the opportunity to be timely, open and transparent in its deliberations, but has instead offered a delayed response full of ‘science words’ but which is desperately short on providing actual scientific evidence and logical argument to support its position.
Amanuensis is an ex-academic and senior Government scientist. He blogs at Bartram’s Folly – subscribe here.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Delicately put, I have rather stronger words for it.
Just what I thought 🙂
Amanuensis, ever the gentlemen. What a gentle way to say putting political expedience and pharma profits over public health.
The note about Barclay’s educational background made me think that he might be wheedling their way out of their difficulties. At least he’s not as bad of one of the previous “Health Ministers”.
Barclay has been an epic failure. The best that could be said of him is that he is about as much use as a chocolate teapot.
My view is that he is a second rate Jabbit. Guilty as sin and by omission as mired in the killings as the rest of them.
You’re right about that. What I thought was that, given his apparent training in legal work, and being educated re history, he might be working out defensive, legally acceptable methods of avoiding payment of damages etc. Not necessarily in the public interest. By comparison, one of the predecessors was an estate agent.
In Brazil there are 6 bills which will criminalise anyone who criticises the Stabs, or who spreads anti-stab ‘hate’. 2-8 years in prison.
I guess the terrifying Rona with its 0.3% death rate is still scything through Brasilia leaving trillions dead.
Why any country is still pursuing any of this bullshit, baffles anyone who walks upright and can think.
Didn’t Brazil have to sign contracts with Pfiser which required them to push the vaccines at all cost and offer land ang govt. buildings as collateral? These bills must be part of that.
‘when they’re gone they’re gone’
And good riddance! Hopefully, never to be seen or heard of again!🤞
” the Government doesn’t have a good understanding of the actual numbers of people in the U.K. (which is astounding in itself)”
Only astounding if you assume the Government is interested in governing effectively. Successive governments have allowed mass immigration to happen despite it probably being quite unpopular with a large section of the electorate. They’ve got every reason to simply play dumb over how many people live in the UK.
…They have absolutely no idea..at all…millions arrive and disappear into the ether….
I know I put this on some months ago, but part of the way they counted immigration was through the Department of Work and Pensions..they are now dropping this..presumably because, although they constantly tell us that immigrants are mainly coming to the UK to work, that isn’t born out in reality…..?
An immigrant count was always very feasible via DWP and still could be.
Once immigrants have been granted some sort of Leave to Remain they can apply for a National Insurance (NI)number. Once they have an NI they can apply for jobs. In reality only the single people apply for work because benefits are not great. However, those couples with children, well it’s like Christmas every day. Benefits including free housing and finance (cash benefits) equivalent to PAYE wages of £25 – 30 k are routine. Plus of course free NHS, dental care, prescriptions, eye care…there’s no end to the taxpayers largesse.
I would suggest counting every NI issued to immigrants and then doubling the number to account for the illegals and that would be a ball park figure.
If the ‘vaccines’ were safe and effective why withdraw for any age group? If there was no risk from the ‘effective’ ‘vaccine’, but a risk, even a small risk, from the virus, why not continue to recommend everyone has them. The move is a tacit admission of a safety problem.
They could be withdrawn on the basis of value for money. However, I think there is very defintely a safety problem, which might not be a problem for some.
Nethen – define value for money.
To a WEFfer seeing off a pensioner at the cost of one more injection as opposed to say ten more years of pension payments would be value for money.
Absolutely. Around March 2021 the AZ blood clot issue was in the news, so NL, which had purchased a fair amount of AZ, pulled it for people under 60. This promptly led to no one wanting it, as they assumed like you, that if there was a safety problem, then it must apply to everyone. I assume that’s why NL did not ban murderna for people under 30, contrary to the Scandinavian countries, Germany and France – they knew too many people would become more and more “anit-vaxx”.
In July 2022 the current Health Minister (an actual doctor, which makes it all the worse) sent a letter to parliament saying he was recommending an autumn booster for people over 50 (or 60, can’t remember exactly). He stated that people under that age had little benefit from the vaxx and to vaxx people without good cause would have legal implications. Fast forward to end August 2022, he sent another letter to parliament, saying everyone over 12 was to be offered the autumn vaxx, again admitting that there was no personal benefit for most, but it might temporarily help slow infection – almost verbatim how it was worded. Nothing about costs of offering drugs to millions of people that didn’t need it, nothing about the legal liability he had previously referred to. There has been a series of extraordinarily lame ads to get the shot going since September, clearly aimed at people over 50 – I can only assume they opened the vaxx up to everyone over 12 because otherwise those over 50 would have refused. As it turns out, most people under 60 have refused 🙂
Surely this is all about using up stocks of V before the expiry date?
….not only spinning the data, but keeping up with the farce….
I can only think that in the face of massive resistance against the boosters they’ve decided to give a ‘sop’ to the masses….I think it’s meant to hoodwink people into thinking there has been a change of tack…there hasn’t..they are as fraudulent as ever…
The whole document is inconsistent…and really doesn’t change anything very much…
Firstly, what exactly constitutes a ‘clinical risk group’? As they suggest that anyone in this group get all the jabs and boosters? This includes, people over 60 and pregnant women….? It also includes children….?
They still suggest persons aged 12 to 49 years who are household contacts of people with immunosuppression get the jag…
They still suggest persons aged 16 to 49 years who are carers, get the jag…
What studies are they basing this on exactly? I would like an FOI to find out?
So are they still manufacturing the primary, long-obsolete doses of clot shots? Or have they just got a load of near to expire stock they need rid of? Same for the boosters. I’m not keeping track of what letters we’re up to now of which ‘scariant’ is meant to be dominating the world but I’m pretty confident the current boosters are not relevant for this ever-mutating alphabet ‘virus’. We’re at a 10 on the ‘Desperation Scale’ now aren’t we? Bloody farcical! Pff…
…yes…..I’ve not thought about it much but.what did happen to the ‘scary, much more transmissible…hide under the bed’ …..Kraken??
It was swallowed by a Leviathan.
Due to constant overexertion, it shrunk to the size of still violently thrashing goldfish which is kept in a fishbowl at the reception of the UKHSA building.
The point of the covax jabs is to stop other people from being afraid of you having a cold. That’s an important public health benefit!
I’m rather looking forward to Dr John Campbell’s podcast on this.
His masterful “take out” of Pfizer’s protestations of innocence after Dr Walker’s revelations was the funniest thing I’ve seen since Delboy fell sideways after the bar had been lifted.
Just one small addendum to the article (and fast becoming my own personal bugbear): unvaccinated under 50s will no longer be able to get the primary course (lol) without first consulting a medical professional.
I am astounded this is not being more widely referred to. A vaccine that was so vital billions were spent on its rollout and a campaign of mass manipulation and coercion to get people to take it; a vaccine that was considered so safe and effective care workers were mandated to get it and genuine consideration was given to vaccine passports, is longer available without going to your GP to ask for it?!
wtf?
Re: “A vaccine that was so vital billions were spent on its rollout and a campaign of mass manipulation and coercion to get people to take it…”
Re the campaign of manipulation and coercion, see Angus Dalgleish’s aggressive promotion of the Covid jabs for young people, in the Daily Mail in July 2021: What every young person who fears the jab MUST be told: Vaccine expert ANGUS DALGLEISH dismantles beliefs that have seen rates stall among the 18-30s.
The Covid jabs are unnecessary medical interventions for young people…and many others…
See my email to Angus Dalgleish: Re: Health practitioners, Covid jabs and ‘valid informed consent’ – a medical ethics disaster. Response to Gus Dalgleish, 13 January 2023.
In computer science, there’s something called the law of diminuishing returns: This is supposed to apply to attempts to tweak code in order to make it run faster. It’s always possible to tweak it some more to make it run yet faster but after all the low-hanging fruit was picked, these tweaks need ever more work put into them and their effective benefit keeps getting smaller.
The same presumably applies to the covax campaign: The cost of increasing covax uptake yet more became higher than the profit which could be made by doing so. It was safe and effective and absolutely vital while large segments of the population were still unvaccinated and thus, large vaccintation yields could be expected from aggressively campaigning for it.
Seems quite a thorough and damaging assessment to me. Nice piece of work. All our institutions are broken so what next ?
(1) ‘The authors have not declared the population estimate.’
(2) ‘Quite where the JCVI got the data to populate its table of vaccine effectiveness is unclear.’
Presumably this information could be obtained through a freedom of information request.
(reposting this from a few days ago as relevant)
I was looking at the latest UKHSA vaccine surveillance report week 2
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1132668/Vaccine-surveillance-report-week-2-2023.pdf
On page 50 is a breakdown of hospitalisations by vaccination status. I thought I would add in on the right a column of percentage unvaccinated (see attached). I don’t have the unvaxed under 40 figure to do a comparison in that age group as UKHSA data only covers over 5s.
As you can see the percentage of ‘covid-19’ hospitalisations that are unvaccinated is almost identical to the percentage of that age group who are unvaccinated in every age group.
So for example 3.5% of the ‘covid’ hospitalisations in the over 75s are unvaccinated and 3.6% of the over 75s are unvaccinated according to the UKHSA’s own data. The 3.5% goes up to 3.7% if you exclude the unlinked but it’s still essentially the same as the unvaxed proportion.
So even in relation to the thing that the experimental vaccinations are supposed to protect against, hospitalisation from ‘covid’, there is no benefit at all with experimental vaccination. Of course experimental vaccination comes with all the significant harms.
Of course this isn’t mentioned in the UKHSA report at all. They simply claim ‘vaccination is highly protective against hospitalisation as VE studies show’
Can anyone confirm my figures are correct?
Why was there ever a ‘vaccine solution’ to Covid-19, given it was known from the beginning it wasn’t a serious threat to most people?
The Oxford-AstraZeneca vaccine was off and running in January 2020, apparently being the longed for ‘Disease X’ to justify a vaccine…but how was this vaccine response justified?
What was happening in January 2020 that justified this response?
Andrew Pollard, who subsequently became the Chief Investigator of the Oxford-AstraZeneca vaccine trials, was in a French taxi, The BMJ reports, on his way to present his group’s research on typhoid, sharing the ride with John Edmunds of the UK Scientific Advisory Group for Emergencies, and they discussed a new virus emerging in China.
But why? Why ‘straight away’ did Andrew Pollard think “we needed a vaccine”? Pollard was also the Chair of the UK Joint Committee on Vaccination and Immunisation – the conflicts of interest of this role for a person initiating a commercial vaccine trial must be questioned.
Also see: Developers of Oxford-AstraZeneca Vaccine Tied to UK Eugenics Movement, Unlimited Hangout, 26 December 2020.
So why was a ‘vaccine solution’ initiated against Covid-19, given it wasn’t a serious threat to most people?
Why were healthy people 18-55 years old included in the Oxford-AstraZeneca vaccine trials?
Why were children included in these trials?
I contacted the chair of the ethics committee responsible for assessing and approving vaccine trials on this matter, the Berkshire Research Ethics Committee, see this email thread: HRA response to FOI 2021/FOI/062.
My request was refused “in part, under FOIA exemption section 43 – trade secrets & prejudice to commercial interests.”
I raised this matter with Andrew Pollard, Chief Investigator of the Oxford-AstraZeneca Covid-19 vaccine trials, and also Chair of the UK Joint Committee on Vaccination and Immunisation, see: Who initiated the plan to vaccinate the entire global population against SARS- CoV-2? 30 June 2021.
As I said in my email to Andrew Pollard:
Yes indeed, this was seriously unethical, and now billions of people around the world have been injected with worse than useless Covid-19 jabs, thanks to the UK taking the lead in getting the Covid-19 jab response off the ground, and being the first to insert needles in December 2020.
Countless people have been subjected to mandated Covid-19 jabs...mandated medical interventions. It’s diabolical. Voluntary informed consent has been trashed, certainly in Australia, where Covid jab mandates have been widespread.
Bill Gates was the leader of the ‘race for a coronavirus vaccine’.
Speak critically of Bill Gates in 2020/2021 and eyes would roll…
But yes indeed, Bill Gates was the kingpin leading the coronavirus response.
See his GatesNotes article, published on 30 April 2020: What you need to know about the COVID-19 vaccine which led in with the statement:
Yes, a software billionaire was leading the coronavirus vaccine response, he’d been leading international vaccination policy for over 20 years – e.g. via influence at the WHO, Gavi, CEPI…
The Bill & Melinda Gates Foundation was also a funder of the Oxford-AstraZeneca vaccine trials, along with CEPI and others.
Brilliant posts, thanks.
“Yes, a software billionaire was leading the coronavirus vaccine response”
I’m reminded of a post on Twitter by the incomparable Ian Brown, nutjob conspiracy theorist, covid sceptic, anti-vaxxer. Someone replied to one of his tweets along the lines of “why should we listen to a musician on the subject of covid vaccines”. His answer was to wonder why we were listening to what he memorably termed a “computer salesman”.
Thanks very much Elizabeth. An absolutely staggering article from Unltd Hangout.
The JCVI should Withdraw all jabs immediately
First Friday Freedom Drinks For all freedom lovers everywhere to meet.
Friday 3rd February 7pm
The Foundry Bell
London Rd,
Wokingham RG40 1RD
Directions from M4 – A329(M) – A329
Directions from M3 – A322 – A329
***
Stand in the Park Make friends & keep sane
Sundays 10.30am to 11.30am
Elms Field
near Everyman Cinema & play area
Wokingham RG40 2FE
Given that Steve Barclay is pushing “vaccines” in a manner akin to a supermarket BOGOF deal I have to conclude this chap is compromised and with some hefty skeletons in his loft.
I hear the feet of rats scurrying across the deck…way past time…after devastating damage has been done to the world – medically, politically, economically and socially.
It’s Time for the Scientific Community to Admit We Were Wrong About COVID and It Cost Lives Written by a medical student and researcher, and published in the mainstream media.
The mainstream media is coming to save us…but there will be many who won’t forget how the mainstream/corporate and taxpayer-funded media, such as the BBC and ABC in Australia, lied to and betrayed the people.
Lies, damned lies and statistics. Who could have believed that critical information could have been so massively distorted to keep the official narrative alive?
I am about to write to the MHRA. They are simply not doing their job.
Is the reason for this simply related to the origin of their funding?
Here in Scotland, the updated Covid-19 guidance for care homes etc continues to promote the jabs as necessary, safe and effective for all staff, including pregnant and breastfeeding women. Unbelievably they’re still claiming they’re important in reducing infection and even to some degree transmission! The importance of vaccination as the main factor in managing the virus is threaded throughout the whole document and makes for depressing reading.