
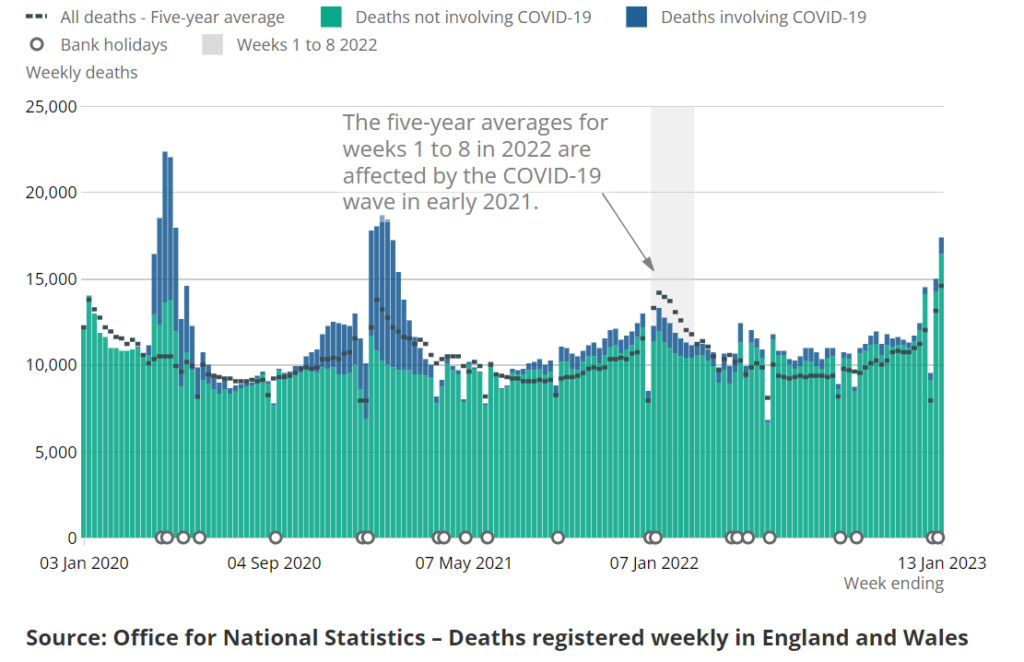
Deaths continue to run at extraordinary levels in England and Wales. In the week ending January 13th 2023 there were 17,381 deaths, which is 2,837 or 19.5% above the five-year average. This is despite the five-year average having risen due to the early 2021 Covid wave. Compared to the pre-pandemic five-year average of 13,822 it is 3,559 or 25.7% above average.
There were 922 deaths with Covid registered on the death certificate, of which 654 were registered as due to Covid as underlying cause. This leaves 2,183 excess deaths from a different underlying cause. Since the wave of excess non-Covid deaths began in April the total now stands at 34,691.
I have previously noted how waves of excess non-Covid deaths appear to correlate with the Covid booster campaigns in spring and autumn, as seen in the chart below, which shows deaths by date of occurrence in England and Wales.
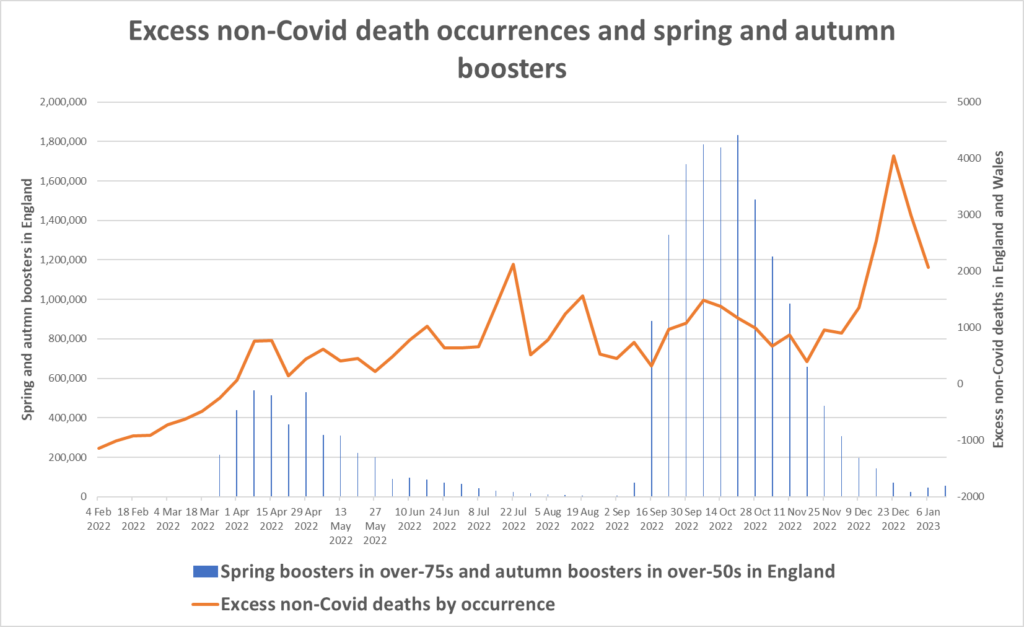
It’s clear, however, that these correlations with booster rollouts are far from determinative of the overall shape of the curve. In particular, deaths remained high during the summer and have spiked over the winter, despite few boosters being delivered in those periods.
The Health Advisory and Recovery Team (HART) has noted this week that high-level mortality data like these do not contain an “obvious smoking gun” pointing to vaccines causing high numbers of deaths specifically during the vaccination campaigns. Rather, the excess deaths are broadly spread throughout the year. The appearance is of something generally raising the likelihood of death, or equivalently, reducing life expectancy. (This doesn’t appear to be due to an ageing population; see here for a discussion on this point.)
The lack of correlation with vaccination programmes has led some to question the role that vaccines are playing in driving the excess deaths and advance arguments in support of other possible explanations, such as Long Covid, the NHS crisis and the legacy of lockdown including missed treatment. While some of these other contributors may be valid, it would be wrong to rule out a role for the vaccines simply on the basis of a lack of correlation with vaccination campaigns. This is because the mechanisms by which a vaccine may injure a person are not fully understood, and those for which understanding is more developed, such as auto-immune reactions due to the persistence of spike protein in the blood and organs, give plenty of scope for a delayed effect. In particular, we should note that many of the excess deaths are related to the heart and circulatory system, and the vaccines are known to increase the risk of such deaths.
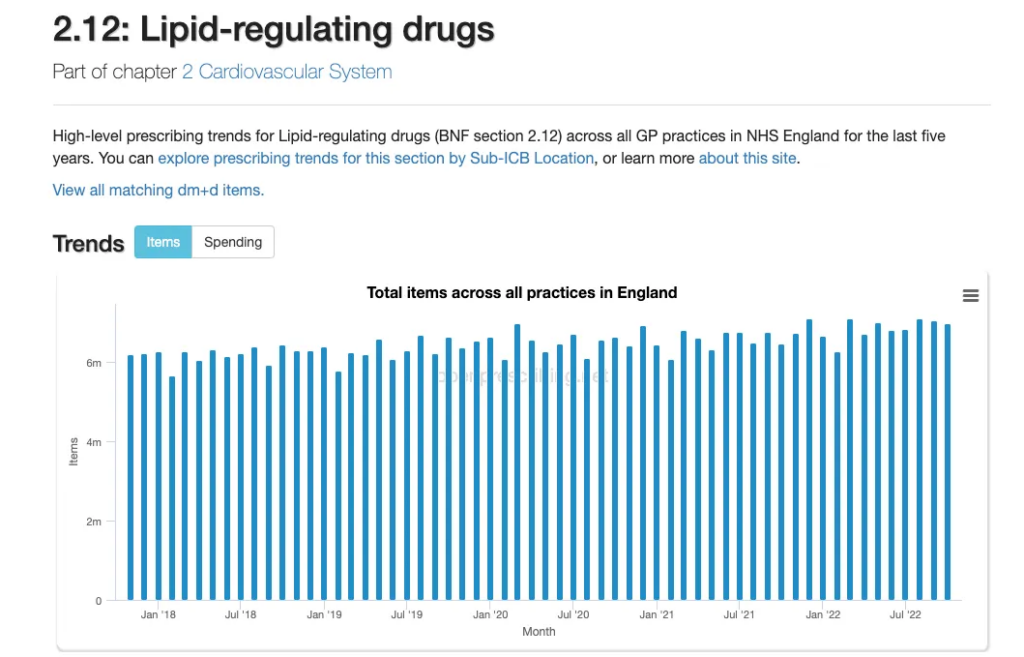
Chief Medical Officer Chris Whitty has recently claimed that 5,170 deaths in men aged 50-64 could have been helped by heart medications that were missed during the pandemic. Health Secretary Steve Barclay agreed, saying that “we know from the data that there are more 50 to 64-year-olds with cardiovascular issues” – a state of affairs he blamed on “the result of delays in that age group seeing a GP because of the pandemic and in some cases, not getting statins for hypertension in time”. The British Heart Foundation published research earlier this month which made similar claims.
However, such claims were dismissed by Dr. Carl Heneghan, Professor of Evidence-based Medicine at Oxford University, and his colleague Dr. Tom Jefferson, who wrote that the extra cardiovascular disease deaths cannot be accounted for by a fall in drug treatment or drop in risk monitoring, “given the lack of evidence of an effect”. In making this assessment they relied in part on a major recent study reviewing the trial data on statins and concluding that the benefits of statins were minimal and most of the trial participants who took statins derived no clinical benefit. Dr. Heneghan and Dr. Jefferson also noted that the claimed reduction in prescriptions appears to be illusory, with rises and falls well within normal levels.
Unlike allegedly missed prescriptions, the NHS crisis is more plausibly contributing to excess deaths, as people experience severe delays getting urgent medical attention. However, the crisis can hardly explain sustained levels of deaths throughout the year or generally increased demand for health services. Something must be making people sicker in the first place.
As I have noted previously, the main alternative explanation is the after-effects of the virus, also known as Long Covid. Interestingly, the British Heart Foundation dismisses this as a factor, laying the blame entirely on access to healthcare – though is there an agenda here of calling for more resources for the sector? But a number of others see the virus as a much bigger factor than the vaccines in driving additional heart deaths.
One problem for the vaccine-deaths hypothesis, they note, is the lack of excess working-age deaths in a number of highly vaccinated countries. Ron Unz has recently written an article drawing attention to this point, observing that while working-age mortality has been very high in the United States and U.K., some other countries, including highly vaccinated ones, have been exempt from this trend.
To develop his argument, Unz draws on analysis which shows that a very strong predictor of working-age mortality in 2022 is mortality in 2020, as illustrated in the charts below.
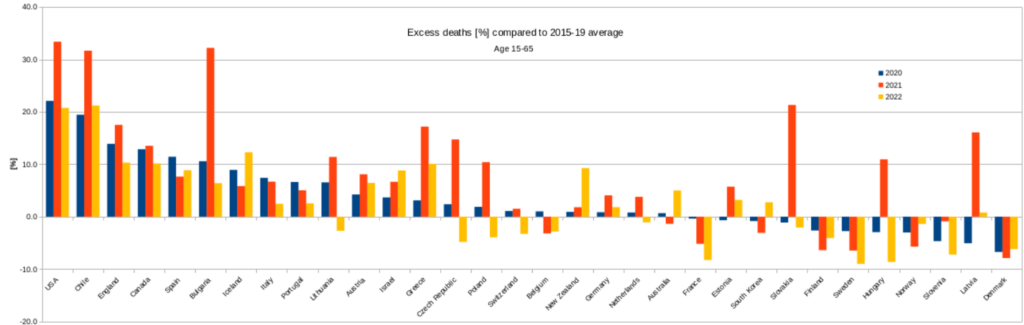
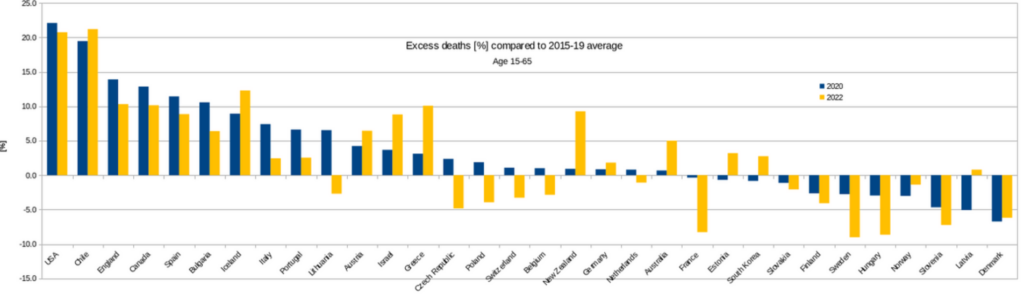
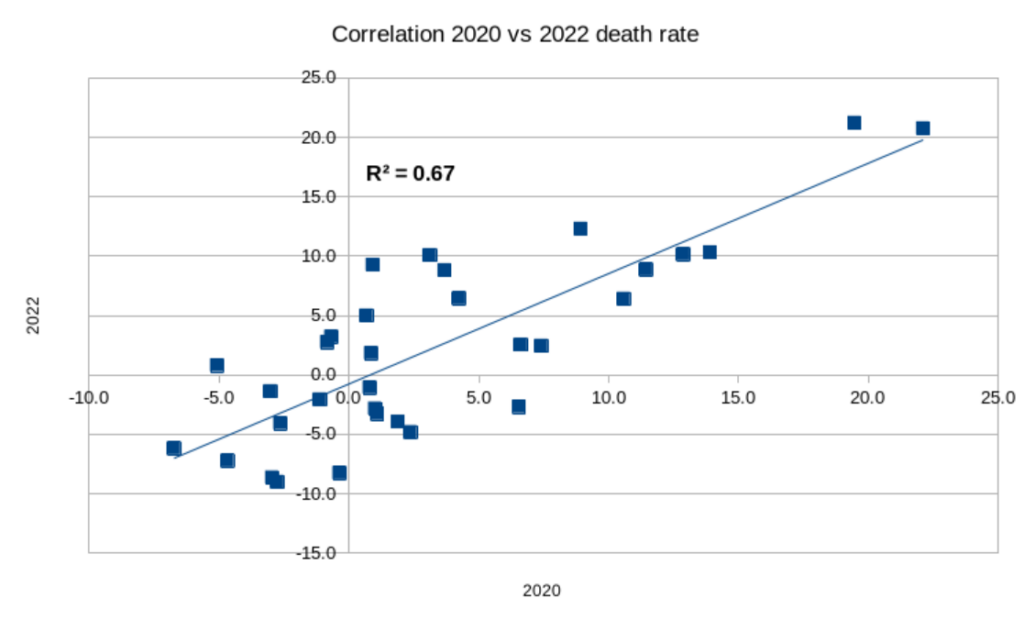
From this Unz concludes that: “The level of 2022 deaths was largely determined by the same factors, probably the interaction of Covid infections with local health characteristics, such as obesity levels and the strength of the public health system rather than having been influenced by the vaxxing.”
This correlation is a very helpful observation, but it actually has the opposite meaning to that which Unz takes from it. Far from suggesting the vaccines are not playing a role, it is consistent with the vaccines playing a significant part. This is because the elevated deaths in 2020 were caused largely by COVID-19 (as well as lockdown measures). But during 2021 and in 2022, Covid was no longer driving excess deaths. Whether this was due to protection from the vaccines, the growth of natural immunity or the arrival of the milder Omicron variants is not material here. What matters is that excess deaths shifted from being primarily respiratory related, driven by COVID-19, to being cardiovascular related, driven by an unknown cause.
What is now driving these excess deaths, which, as Unz notes, appear to be occurring among the same risk groups as were at risk of serious COVID-19? Unz proposes it is still Covid, and that despite the reduction in the severity of the disease, it is the virus behind the scenes driving the extra cardiovascular deaths.
This is a false dichotomy, however. An argument for the virus being involved in non-Covid cardiovascular deaths is also an argument for the vaccines potentially being involved as well. This is because one of the main contentions supporting the vaccines being involved is that the mRNA and spike protein travel to various organs, especially the heart, and persist there for weeks and months, causing injury and triggering auto-immune attacks – a mechanism supported by a number of autopsy studies. This is a very similar mechanism to how the virus may contribute to problems with the heart and other organs. Indeed, it is likely that both are contributing to the effect, reinforcing each other in various ways. Another possibility is that the immune tolerance induced by repeated vaccinations is contributing to the persistence of the spike protein in the body. Either way, it means that the underlying risk factors for Covid death will often be the same for vaccine death, and the correspondence between mortality in 2020 and 2022 would therefore be expected.
The question is whether the virus or vaccines are playing the bigger, more fundamental role in driving excess heart deaths.
One reason for thinking that the vaccines may be playing a big part is that the vaccine enters the body via the blood directly whereas the virus enters via the respiratory tract and thus has much more limited access to the blood and heart in most cases.
Further evidence supporting a role for the vaccines comes from the work of Professor Christine Stabell-Benn and colleagues, who looked at the vaccine trial data and found no overall mortality benefit from the mRNA vaccines, and a particular signal for increased heart deaths. This suggests that while the vaccines reduce Covid deaths they may increase other deaths, particularly from cardiovascular causes.
Some health experts in Japan have come to a similar conclusion. In that country, Covid deaths have actually been increasing after each booster campaign. Public health authorities have noted, however, that the ‘Covid’ deaths now are more likely to be test-positive deaths from cardiovascular problems rather than classic respiratory deaths. There are also many non-Covid excess deaths in Japan, again largely from heart problems.
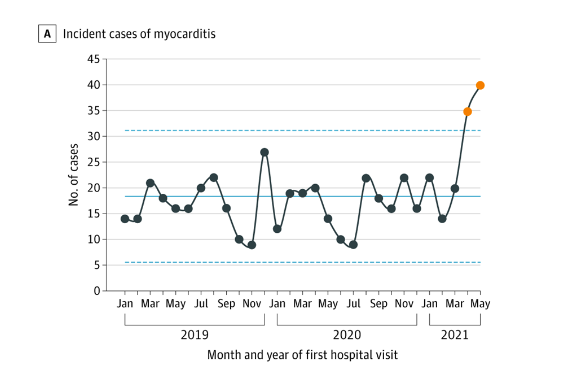
With respect to myocarditis in particular, a recent analysis by HART notes that elevated myocarditis admissions began with the vaccine rollout and did not occur in 2020, indicating a limited role for the virus and a major role for the vaccines.
Given this evidence that the vaccines may be playing a large role in excess deaths, why are working age deaths below average in many countries, as Unz observes?
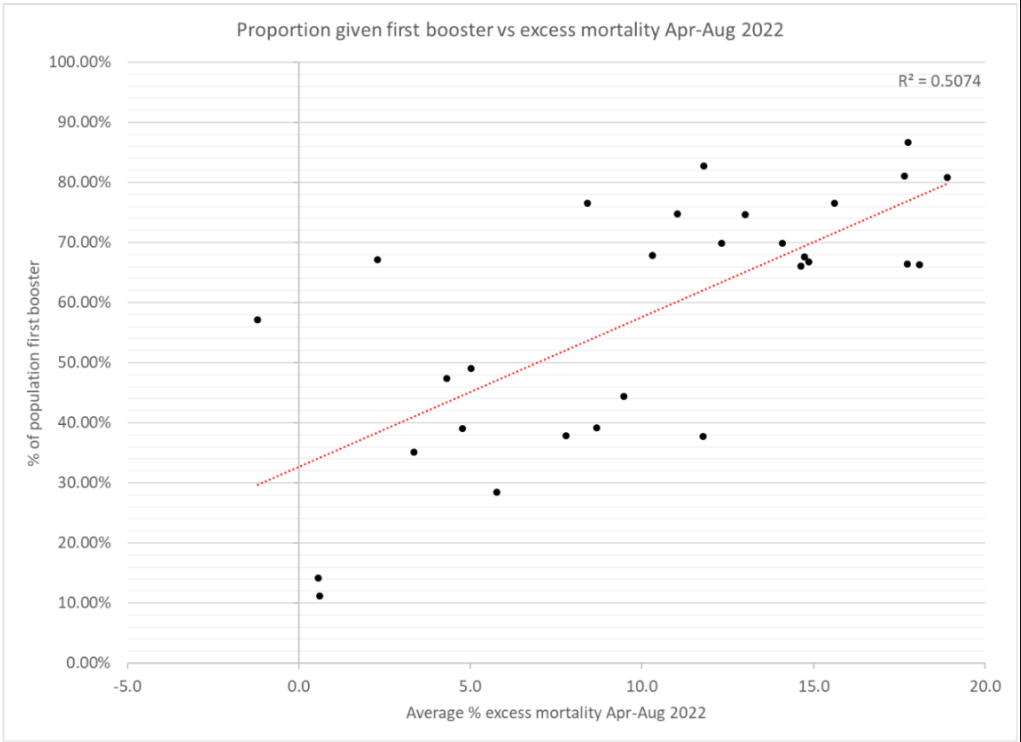
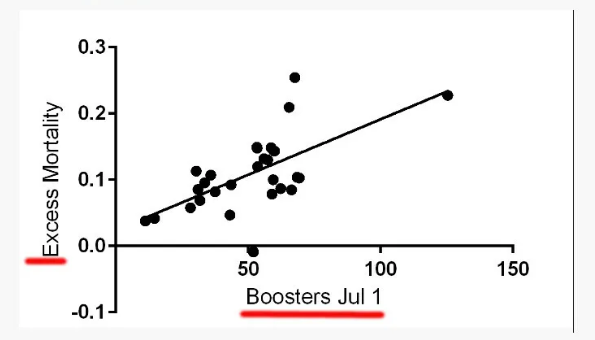
Differences in vaccination rates may be doing their bit here. Some analyses have suggested that higher booster rates are associated with higher deaths in 2022.
This may explain some of the variation. Also, recall that for working-age mortality, Unz’s analysis shows that one of the main predictors of 2022 mortality is 2020 mortality, suggesting a common cause in both years. A natural interpretation of this, given the drop in Covid severity and the arrival of the vaccines, is that populations less susceptible to COVID-19 are, for the same reasons – prevalence of obesity, heart disease and so on – also less susceptible to fatal vaccine injury.
What we really need are more and better data – split by vaccination status, age, health conditions, prior infection status and so on. Even better, we need well-designed, prospective, controlled studies that look into these things properly. The fact that, after more than two years, we still have none of these things should give even the most ardent defenders of the vaccines pause for thought. If the data were favourable to the vaccines, would they not have been made available with great fanfare long ago?
In the meantime, it’s clear that the vaccines are still a leading suspect in the question of why so many people have been dying, mainly from heart-related issues, in the last two years.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
‘Leading’ Suspect? This makes me laugh.
So what else do you have? Climate thingy, Eggs, Happiness, too much-something-or-other? Stress? Air pollution?
Face it. The Stabbinations in the UK have murdered 50–100 K. The terrifying Rona killed 20.000. Now, I know I am an idiot and not ‘The $cience’ but I do calculate that the stab deaths are 2.5-5 x higher than the Rona. And, notwithstanding my stupidity, I will add that heart disease, coronary, organ and brain issues, in train but not yet manifested, will only add to this total. I know. I know. I am just another racist Hitler, denying $cience…etc. And we should add in the 30.000 murdered by Midazolam and other LD dead as well. Obviously the farce checkers ‘protecting democracy’, will object.
I didn’t get vaccinated because I considered that the vaccines trials did not prove they are safe. However, I feel some caution is needed in assuming that the vaccine is the cause of increased deaths. Some inquests have concluded that the vaccine was the cause of death but I have yet to see the reasons published.
If you believe the vaccines are killing people then ask why it is not everybody who has been vaccinated. The answer is that there are other factors involved.
However, I believe there is sufficient concern to justify a halt to the vaccine programme.
Another interesting correlation is the continuing excess deaths and the withdrawal of the “vaccines” for under 50s. Just another coincidence?
I was coming on to post just that. And for those of us who remained unvaccinated, we can’t even get a dose without being recommended by a medical professional.
so rather than being ‘safe and effective’ (lol) they are tacitly admitting it’s not even as benign as the flu jab.
what a mystery.
It’s probably not as benign on the balance sheet either. It could be ironic if money is the cure in the longer term.
Yes, Joel Smalley does a great job of taking this apart in his latest substack;
https://metatron.substack.com/p/the-cat-is-out-of-the-bag
One possible mechanism for the deaths is that the jabs have damaged the immune system, a jabbed person gets infected with SARS-COV-2 which goes on to cause serious damage, killing a proportion of the jabbed, leading to excess deaths.
See for example Igor Chudov twitter from 24 Jan.
https://twitter.com/ichudov/status/1617735026518659073
Fundamental to this mechanism is the circulation of SARS-COV-2, which as we know is seasonal and comes in waves for reasons that we don’t understand and can’t predict. Maybe the highly jabbed countries currently experiencing no excess deaths are merely waiting their turn.
Possibly bad news for Sweden, which has been an anomaly to the trend during 2022 for more highly injected countries having higher levels of excess deaths.
I think that Sweden got a lot of natural immunity in 2020 and 2021 when they did not lock down and before everyone was vaccinated. Thus the vaccines will have done less harm to their natural immunity. They are now reaping the benefit of that natural immunity.
My feeling is that while there are specific dangers to the vaccines in the immediate post shot periods, which cause waves of sudden deaths, the real problem is the changes the vaccines bring about in the human immune system. The move to IgG4 antibodies in the multiple boosted is the tell tale sign – people’s bodies are coming to tolerate a covid infection rather than attack it, and it is doing damage to all manner of organs, resulting in deaths that are in fact covid related but don’t look like one.
This may continue indefinitely, or rather until all those who were multiple boosted have died.
I think that Sweden got a lot of natural immunity in 2020 and 2021 when they did not lock down and before everyone was vaccinated.
But this implies that lockdowns are effective in preventing spread, and I don’t believe that’s the case. So there must be some other explanation (and never forgot that we are dealing with inconsistent and even fraudulent data from across the world).
I do agree with your second paragraph – my feeling is that it’s the deeper, longer-term effects on the body from the stabs that are going to be the real legacy of this pinnacle of stupidity.
We know that not all batches of ‘vaccine’ are equally harmful, from research carried out in the USA. It could be that some jurisdictions were targeted with more deadly batches.
Didn’t Deagel predict much larger population reductions in some countries?
Such as the USA and UK?
Yes, there could be purposeful “adjustments” to batches, but consider how quickly the vaccines were produced. Safety shortfalls, dodgy ingredients, and careless mixing all could have an effect on what was in each syringe. Add in the method of injection–into the tissue or directly into the bloodstream–and the differing physiology of each person and we get a variety of reasons why there seem to be differing timelines on adverse effects and deaths.
And the people bowed and prayed
To the neon god they made
And the sign flashed out its warning
In the words that it was forming
And the sign said, “The words of the prophets
Are written on the subway walls
And tenement halls
And whispered in the sounds of silence.
Is it ok to post another link to this version?: –
https://www.youtube.com/watch?v=0_kGbNOXJjA
“What we really need, of course, are more and better data – split by vaccination status, age, health conditions, prior infection status and so on.”
What’s most fascinating psychologically to me is that the vaccinated public does not seem to want to know and does not demand this.
It’s almost as if they already know the result and prefer to put their head in the sand instead.
And when you add in the children and their parents responsibility for them, it becomes even more fascinating.
I think it’s a combination of being deeply uncurious and being in denial. I posted this a few weeks ago, but it bears reposting. The colleagues involved have IQ well above average so they are not “stupid” in the accepted sense, though they obviously have fundamental flaws in parts of their “intelligence”:
Recent conversation with some work colleagues:
Colleague 1: My dad has covid, he keeps testing positive
Colleague 2: Has he been vaccinated?
Colleague 1: Yes, four times. I’ve just had covid too. I’ve been vaccinated twice.
Me: I’ve not been vaccinated at all. I’m still alive and well.
Colleague 1: Are you one of those conspiracy people?
I thought that colleague 1 was going to blame you for their repeated illness and poor health. But that would’ve been too ridiculous. Oh, er.. never mind.
I’ve been called a conspiracy theorist by several of them, and compared to Hitler, but none of them have accused me of making them ill. I never go to the office, in part so I don’t have to see these people and listen to them talking shit about The Current Thing.
Glad to hear it tof, I suppose we should be grateful for small mercies. How some minds blame those who didn’t take the potion for it not working effectively in those who did though is quite the cognitive leap. No other medicine has people in such knots than the almighty v.
I guess if it’s 100% effective it could in theory stamp out a virus if everyone took it the same day, or within the same week? Maybe? How long does a virus take to mutate? The ultimate question I presume. And is the global dissemination & administration of a vaccine within such a short timespan ever a viable undertaking. Questions even now no one in authority seems to contemplate. Just take it – we’ll all be the better for it.. because!
My unvaxxed status came up in conversation with an ex-colleague at a social event while we were discussing foreign travel and vaxx passports. He chortled when I said I had a done a risk-benefit assessment of the vaxx and it had come up short, as if I was some kind of mad uncle. A week or so later I happened to be making a rare appearance in the office and a different colleague said to me, out of the blue, “so, I hear you’ve not been vaccinated”. So clearly my status had been a talking point among half the office to have got from an ex-colleague to someone completely unrelated. I don’t give a toss who knows about it, but I thought it was a bloody cheek. I don’t have much respect for them, TBH. Out of 70-odd there is one other definitely unvaxxed that I know of, and a couple who now admit to regretting it. The rest are probably vaxxed, certainly most of them as they were all chirping about it whenever they went to get their jabs, suffered side effects, got covid.
Yeah, it is remarkable how any risk assessment for a vaccine is considered crackpottery when it’s common practice for any other medicine to be risked vs any reward gained from taking it. Ol’ Billy has the vaccine industry set apart from all other medicines as far as.. it is the right choice for the patient in question? It just is .. and there’s no debating it. It’s bizarre how narrowminded the whole psyop has become around vaccines specifically.
Good to hear you’re not phased by it, and as much as it’s a little disconcerting hearing your medical choices being banded around the workplace – one can take great comfort in knowing you did the right thing. And they know it too, it’s simply the mass formation that forbids them from acknowledging it and having to open that whole can of worms.
I’m lucky in that I’m one of the bosses and my boss, the CEO, is a covid sceptic so I’ve never felt under pressure in any way, just a bit sad I can’t enjoy the company of most of my colleagues now but thankfully I can WFH full time so I never have to see them. The ones I still get on with I just see socially outside of work. Most sceptics are probably not so fortunate.
Am I wrong, I wonder, to refuse to reveal private medical information (whether or not I have had an experimental mRNA drug or not) as a sort of point of principle, in a similar way to how I don’t normally talk about who I have voted for (private ballot and all that)?
Anyhow, rest assured that this sort of ratio does not apply to all work places.
Not wrong at all
I personally don’t mind if people ask me, as I am happy to justify my decision, but equally people should be prepared to be told to mind their own business
What pissed me off was finding the whole office was gossiping about it behind my back- if I tell you something personal about me it’s not for you to chirp about it to all and sundry
They were all constantly chirping about having been jabbed and then chirping about getting Covid. I’d get emails along the lines of “sorry boss I can’t work today I’ve got Covid”. I don’t bloody care what’s wrong with you – keep it to yourself. All you need to say is that you’re sick.
I work with a bunch of virtue signalling metropolitan liberals and go along to get along types.
Don’t forget that anybody who wanted/needed to travel abroad in 2021-22 (my case) and anyone who worked for a large company or in a public-facing role had NO REAL CHOICE. It really was accept the jab or bear considerable costs. It really was the devil or the deep blue sea, no-win.
Yes until there is a written record of everyone’s vax status then there will always be denial and ignoring of the part the toxic jabs have played in the whole excess deaths shebang. The trouble is I can’t see this ever happening so we’ll never get to the truth. The authorities know this is the crux of the issue, they know the vax is responsible, that’s why they double down in ensuring victim’s vax status is never mentioned in media reports and it’s why they’ll never open an investigation into the safety of the very bioweapons they pushed on everyone. They’re guilty of democide so why would they? Denial and obfuscation of official data is the only thing standing between them and a ”guilty” verdict. It’s also, tragically, why nobody will ever be held accountable for their part in committing crimes against humanity. Everyone onside with the narrative has indemnity from liability so they’re all untouchable.
Future generations might deal with it. All the more so if they realise they have become victims of it all. Perhaps the timeframe is longer than the typical carrier duration of some of the current crew.
Another indication of serious harm through the gene therapies. Derived from official population-wide data in NZ. https://alexberenson.substack.com/p/urgent-a-big-new-zealand-study-reveals?utm_source=profile&utm_medium=reader2
I was in hospital for a kidney operation last year. The man in the next bed told everyone he met that one of his kidneys was 80% destroyed by COVID vaccine induced blood clots.
Speaking of excess deaths, here’s John Campbell’s latest. Excess deaths in 30 countries. Bradford-Hill criteria of consistency being met. Perhaps if 3000 people per week in the UK died in plane crashes or train wrecks it might actually get the attention it deserves, it is lives being lost one way or another after all, but how this is not being acknowledged by the authorities across the countries or deemed worthy of investigation is just another example of the ‘lockstep’ approach that we are all familiar with now. It’s like governments are hoping that if they ignore it it might go away. Pathetic.
https://www.youtube.com/watch?v=av4Ej6om0WI&ab_channel=Dr.JohnCampbell
I know, I’m like a broken old record.
But, for CVS problems look at paras. 10 and 14. You don’t have to be an “expert” to understand the gist of it.
https://www.sciencedirect.com/science/article/pii/S027869152200206X
For the rest of the harms attributable to the mRNA, just read the rest of it.
There has never been any coherent criticism of this paper and others similar, but the problem we have is that of the powers behind the MSM who will simply say continue to ignore everything. This is despite the clear temporal relationship between the jab and death/severe injury.
The problem will worsen because for the other jab induced injuries ie autoimmune disease, there will be no such temporal relationship.
We have real world concrete evidence that mRNA jabs are harmful.
We have have sound genetic and immunological evidence as to precisely how and why the harms are caused.
The MHRA and UKHSA are completely useless and or complicit in this debacle.
The individuals within, and I include the NHS here, should be prosecuted for Manslaughter and where applicable, AOABH.
You were told – and are still being told, that the jabs “are safe and effective”. This was always a lie.
Heads should roll.
They are making a huge mistake in sticking to their guns and yet their crime is so monstrous that they can;t do otherwise. In a sense this is the dynamic we need because the dynamic itself expresses the utter corruption of our paradigm. On the other hand we have all been compicit because from the latter half of the nineteenth century onwards was a move in this Ahrimanic direction and we were snapped out of it every now and then like in The Wizard of Oz. Just Glinda declaring herself a good witch was the introduction of the idea that these powers can be used in our favour.
When are you going to wait until next week next month? If you look at the graphs from various countries it is very very obvious. There will be no legitmate response when the truth gets out but I would advise being honest now. Because beyond this point there are n guarantees.
.
I got vaxd three times because I’m in the high risk category and am now the proud owner of a very expensive pacemaker. No doubt whatsoever that the former led to the latter. My cardiologist even said as much. He also said he’s busier than he’s ever been in his 30 years in the job. It’s yet another covid scandal and of course it’s ignored completely by the MSM cheerleaders.